Feeding bottle for cleft palate baby
Cleft Feeding Instructions - Seattle Children's
Why do babies with clefts have problems with feeding?
Babies with clefts have trouble with feeding because it changes how parts of the mouth are formed and how they work and fit together.
- Cleft lip makes it hard for babies to make a good seal around the nipple.
- Cleft palate makes it hard to create suction because the mouth cannot be closed off from the nose.
Normally, a baby pulls the nipple into their mouth and makes a seal with the lips around the nipple. When the baby sucks and swallows, the back of the roof of their mouth (soft palate) rises up and closes off the mouth from the nose. This creates suction and holds the breast or bottle nipple in the mouth, and the baby sucks to draw out milk.
How do I feed my baby with cleft lip?
Babies with only cleft lip can usually be fed by breast or regular bottle. Our nurses and infant-feeding specialists can help you make sure your baby gets a tight seal around the nipple.
Breast-feeding
- During breast-feeding, the soft breast tissue often will fill the opening in the lip and/or gum line. This seals off the mouth and lets your baby create enough suction.
- Sometimes it helps to hold a finger across the cleft while your baby feeds.
- Swallowing noises and normal weight gain are signs that breast-feeding is going well.
- If your baby is "noisy" with feeding, making clicking or kissing noises, they may not have enough suction.
Bottle-feeding
- If you bottle-feed your baby, feeding may work better using special bottles or nipples with a wider base.
- When starting a feeding, hold your baby in a slightly upright position.
- Touch the baby's lower lip with the nipple.
- When the baby latches on, direct the nipple slightly downwards.
- Try to keep the nipple in the center of the baby's mouth. Do not let it slip up into the cleft.
How do I feed my baby with cleft palate?
Babies with cleft palate usually need special bottles and techniques to feed well, whether or not they have cleft lip.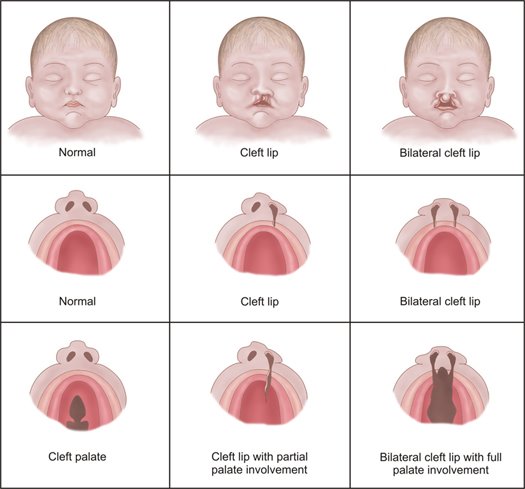 It is rarely possible to breast-feed or use a regular bottle.
It is rarely possible to breast-feed or use a regular bottle.
With cleft palate, a baby cannot create suction to get milk out of the breast or bottle.
A baby who is put to the breast may look like they are latching on and sucking well. But they are using up energy and getting little or no milk.
If you planned to breast-feed, we encourage you to express your milk and feed your baby using a special bottle.
Breast milk is considered the most ideal food for all babies. There are added benefits for babies with cleft palate, such as fewer middle ear infections.
Often, mothers who were looking forward to breast-feeding feel great sadness at the loss of this experience. We encourage you to acknowledge this loss and seek support. We can help with feeding techniques to help you maintain closeness with your baby.
What kind of bottle should I use for feeding with cleft palate?
There are 4 types of bottles for feeding babies with clefts:
- Cleft Lip/Palate Nurser by Mead Johnson
- SpecialNeeds Feeder by Medela
- Pigeon feeder with one-way valve
- Dr.
 Brown’s Specialty Feeding System with one-way valve
Brown’s Specialty Feeding System with one-way valve
The Pigeon nipple with one-way valve can be used with any bottle.
The Cleft Palate Foundation website has a video on feeding your baby and information on how to order supplies online.
Cleft Lip/Palate Nurser by Mead Johnson
Cleft Lip/Palate Nurser
by Mead Johnson
The Cleft Lip/Palate Nurser by Mead Johnson is a low-cost, soft, squeezable bottle.
We suggest that you replace the long yellow nipple that comes with the bottle. Use any shorter, softer nipple.
- Before using the bottle for the first time, put some water in it and practice squeezing the liquid out of the nipple. This will help you get a feel for how firmly you need to squeeze.
- When you squeeze the bottle, the liquid should flow easily but not too fast.
- As your baby begins to suck, squeeze the bottle with a firm, steady pressure to the count of "squ-e-e-ze-2, 3." Relax your squeeze on the 2, 3 count.
 This pauses the flow of milk.
This pauses the flow of milk. - You should only squeeze when your baby is sucking. Watch your baby closely and listen for swallowing sounds.
- If your baby pauses to breathe, you should pause also. If your baby is getting milk out of the bottle, you should see air bubbles in the milk.
- If you forget to stop squeezing the bottle when your baby pauses, your baby may cough and sputter. Just take the nipple out of the baby's mouth for a moment and let them settle. Then continue feeding.
If sputtering happens throughout the feeding, call the Craniofacial team for advice: 206-987-2208. Most parents quickly learn to adjust squeezing to their baby's sucking rhythm.
SpecialNeeds Feeder
SpecialNeeds Feeder
The SpecialNeeds Feeder by Medela has a one-way valve that keeps milk in the nipple. It does not require suction.
This bottle used to be called the Haberman feeder.
Sometimes babies can get milk from this feeder themselves by pushing the nipple against their gum line. The nipple is soft-sided. For many babies, it works best for the parent to squeeze the bottle to match their baby’s rhythm of sucking and swallowing (as described earlier for the Mead Johnson nurser).
The nipple is soft-sided. For many babies, it works best for the parent to squeeze the bottle to match their baby’s rhythm of sucking and swallowing (as described earlier for the Mead Johnson nurser).
There is a “Y” cut in the nipple. Turning the nipple in the baby’s mouth changes the orientation of the “Y” cut in the baby’s mouth. This varies the rate of flow. The nipple has 3 lines that indicate which flow rate is in effect.
Dr. Brown’s Specialty Feeding System with one-way valve
Dr. Brown’s Specialty
Feeding System
You can buy Dr. Brown’s Specialty Feeding System with one-way valve through Amazon. The Dr. Brown’s bottles sold in stores do not have the one-way valve.
Dr. Brown’s Specialty Feeding System uses a bottle with a one-way valve at the base of the nipple to keep the nipple full of milk. It does not require suction.
- When the baby bites or compresses the nipple, milk flows into their mouth and not back into the bottle.

- The one-way valve ensures that there is always milk in the nipple.
- The baby controls the rate of the feeding.
Pigeon feeder
Pigeon nipple with one-way valve
The Pigeon feeder has a nipple with a one-way valve. The nipple can be used with any bottle.
The nipple comes in 2 sizes. The smaller size has a slower flow. It is best for newborns.
The larger, faster-flowing nipple works well for babies 6 weeks and older.
The Pigeon nipple with one-way valve works by compression only. No squeezing is needed.
- A plastic one-way valve that fits into the nipple keeps milk in the nipple. Place the valve with the flat side toward the tip of the nipple.
- When your baby begins to suck, milk flows easily. Your baby controls the flow of milk.
- The nipple has a firm side that goes against your baby’s gum line and a softer side that goes on their tongue.
- A small notch near the rim of the nipple serves as an air vent.
 This notch should be under your baby's nose when feeding. This puts the nipple correctly in your baby’s mouth.
This notch should be under your baby's nose when feeding. This puts the nipple correctly in your baby’s mouth. - Tightening the nipple slows the flow of milk. Loosening it makes the flow faster.
- If the nipple collapses, loosen and retighten it.
The Cleft Palate Foundation website has information on how to order these supplies online.
How do I care for the bottles and nipples?
All of these bottles and nipples can be hand washed in hot soapy water. Rinse and allow to air dry.
Do not boil the bottles or parts. Do not wash them in the dishwasher or put them in a microwave. They may soften and start to leak.
How do I express breast milk for my baby?
If you want to express breast milk for your baby, we recommend a hospital-grade electric breast pump with a double pumping system.
Birth hospitals have pumps for mothers to use in the hospital. You can rent or buy a breast pump for use at home. Insurance can cover rental or purchase of a breast pump for a baby with a cleft palate.
At first, pump at least 8 times in 24 hours, including at least once during the night. After several weeks of frequent pumping, most mothers make enough milk by pumping about 6 times a day. Tips for pumping breast milk (PDF).
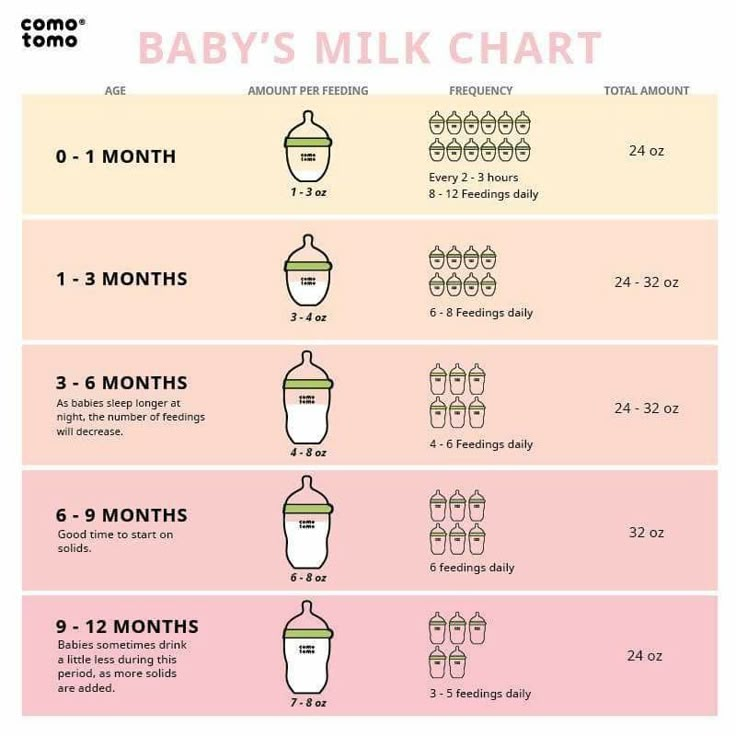
How much should my baby eat?
Newborn babies begin with frequent feedings of very small amounts of milk (1 ounce or less). Over time, they increase the amount they can take.
By 2 weeks of age, a baby needs at least 2 to 2.5 ounces of milk per pound of weight each day. For example, a 3-week old baby who weighs 9 pounds should have at least 18 to 22.5 ounces of breast milk or formula in 24 hours.
A feeding session should take no longer than 30 minutes. If it takes longer, your baby is working too hard and burning calories needed for growth.
We recommend weighing babies weekly until they show a normal rate of growth. Usually this happens in 4 to 6 weeks.
How often does my baby need to eat?
During the first month of life, a baby will feed 8 to 12 times per day — every 2 to 3 hours. A baby this young usually feeds at least 2 times during the night.
A baby this young usually feeds at least 2 times during the night.
At 2 to 4 months, a baby will feed 6 to 8 times per day — every 3 to 4 hours.
How will I know if my baby is gaining enough weight?
A baby usually loses weight the first week of life. The loss is usually 5% to 10% of their body weight. Your baby should regain this weight by 2 weeks old.
At first, we expect your baby to gain 5 to 7 ounces per week. At 4 to 6 months old, the rate of weight gain slows. Your baby should gain about 3.5 to 4.5 ounces per week.
What if my baby is not gaining enough weight?
Sometimes babies with cleft lip and palate have difficulties taking enough breast milk or formula to grow.
Ask your medical team for advice. They can give you an approved recipe for adding formula powder to breast milk or regular formula. This gives your baby extra calories, protein and vitamins. Talk to your healthcare team before doing this.
What about starting solid foods?
Babies with clefts can start solid foods at the same age as other babies. Most often, this is at 4 to 6 months.
Most often, this is at 4 to 6 months.
Experiment to find the right consistency for solids. It needs to be just right so your baby can eat without the food coming out their nose. This is not harmful to your baby. Sneezing will usually clear the food out of the nose. Most babies learn quickly to get the food down their throats rather than out their noses.
Can my baby drink from a cup?
Cup feeding can also be started at the usual age, 8 to 12 months. Cups with plain lids can help limit spills. Do not use spill-proof cups with valves. These require that baby create suction to get any fluid.
See the Cleft Palate Foundation website for a video on feeding your baby and information on how to order supplies online.
Cleft Palate: Feeding Your Baby
The palate, more commonly referred to as the roof of the mouth, separates the mouth from the nose. The palate is important for feeding and speaking. A cleft is an opening or split in the palate. This cleft can make feeding hard for your baby. Most babies with a cleft of the palate are not able to use standard bottles or solely breast feed because they cannot create the suction needed to draw the milk out of the nipple. Special bottles and nipples are available to help infants with cleft palate feed and grow. These bottles may be used with formula or breast milk.
Most babies with a cleft of the palate are not able to use standard bottles or solely breast feed because they cannot create the suction needed to draw the milk out of the nipple. Special bottles and nipples are available to help infants with cleft palate feed and grow. These bottles may be used with formula or breast milk.
Supplies for Feeding Your Baby
Several types of bottles and nipples are available to help you feed your baby. You may need to try more than one feeding system before finding the best one for you and your baby. Our feeding team will work with you and your family to make sure your baby is feeding well and gaining weight.
Examples of Feeding Systems
Assisted Delivery Systems
- Enfamil® Cleft Lip/Palate Nurser: This bottle is soft and squeezable and comes with a long, stiff nipple. It can also be used with any standard sized nipple, like an orthodontic nipple. To feed your baby, gently squeeze the bottle using a pulsing rhythm while your baby is sucking to help provide the milk (Picture 1).
- Medela® SpecialNeeds™ Feeder (formerly known as the Haberman Feeder™): The flow rate can be adjusted depending on which line is pointing toward the baby’s nose. This nipple has a one-way flow valve to allow the milk to enter your baby’s mouth when the nipple is squeezed. (Picture 2).
Infant paced systems
- Pigeon™ Nipple/Bottle: This Nipple fits on any standard bottle. It has a one-way flow valve that is inserted into the nipple. The special nipple has a soft side and a hard side (Picture 3). The hard side faces up and the soft side sits on the baby’s tongue. There is a notch (air vent) on the nipple that faces toward the baby’s nose during feeding. The baby compresses on the nipple during feeding to draw the formula or breast milk into their mouth.
- Dr. Brown’s Specialty Feeding System®: This feeding system also has a one-way flow valve that is placed into the nipple to help your baby feed.
 This valve is very important for feeding. It cannot be found in the bottles available at stores, so it must be purchased online. Please discuss this with our feeding team. The one-way flow valve allows your baby to self-pace by compressing on the nipple. The valve can be used with any level nipple, but you must watch your baby carefully during feeding to make sure the breast milk or formula is not flowing too fast.
This valve is very important for feeding. It cannot be found in the bottles available at stores, so it must be purchased online. Please discuss this with our feeding team. The one-way flow valve allows your baby to self-pace by compressing on the nipple. The valve can be used with any level nipple, but you must watch your baby carefully during feeding to make sure the breast milk or formula is not flowing too fast.
How to Feed Your Baby
Here are some tips for feeding:
- Prepare the formula or breast milk for the bottle. If you are using powered formula, mix it with bottled water. Follow the mixing directions carefully for your baby and use the right measuring scoops or spoons.
- Cuddle your baby for a few minutes before you start to feed. This will help you both relax to make feeding time more pleasant.
- Hold your baby in an upright position on your lap and tilt him or her back slightly (Picture 5).
 This helps the baby to swallow while preventing milk or formula from flowing into the nose or middle ear.
This helps the baby to swallow while preventing milk or formula from flowing into the nose or middle ear. - Rub the nipple of the bottle on the lower lip to help place the nipple into the mouth. This starts the sucking reflex.
- You should hold the bottle during the whole feeding time. The bottle should not be propped by a pillow or other item during feeding. This is not safe for your baby and can cause choking.
- Burp your baby often (after every 1/2 to 1 ounce). Babies may swallow air during feeding.
- Watch your baby closely during feeding to make sure the baby is eagerly and actively engaged in feeding.
- Feeds should be completed in 30 minutes so that your baby does not get too tired. This does not include time spent burping or changing the diaper.
If you put your baby to bed after the feeding, place the baby on their back.
As babies get older, they will need more than just formula or breast milk. Be sure to ask our feeding team about when you can start feeding cereal, fruits and vegetables.
Be sure to ask our feeding team about when you can start feeding cereal, fruits and vegetables.
If your baby has coughing, gagging, choking, milk running out of the mouth, or signs of distress, like labored breathing or watery eyes, they may be getting too much milk. If you notice these signs, please contact our team for help. You may see that some milk leaks out of the nose during a feeding. This is normal for a child with cleft palate that has not been fixed. It does not mean your child is choking. To help with this, keep your baby more upright during and after feeding. Most infants with cleft palate can feed successfully.
When to Call the Doctor
Call our feeding team or your child's doctor if your baby has:
- Weight loss or failure to gain weight
- Coughing or choking with feeding
- A sunken soft spot on the head
- Feeding takes longer than 30 minutes
- No wet diaper for 6 hours straight
- A hard time waking up for feeding.
 Some children who have other medical conditions along with a cleft palate may have a harder time with feeding and will need other changes in their feeding plan. If you have any questions, be sure to ask your baby’s doctor or nurse, or call 614-722-6449.
Some children who have other medical conditions along with a cleft palate may have a harder time with feeding and will need other changes in their feeding plan. If you have any questions, be sure to ask your baby’s doctor or nurse, or call 614-722-6449.
You can find more information about feeding on the web site of the Cleft Palate Foundation: www.Cleftline.org.
When Your Baby has Surgery
Children have surgery to repair a cleft palate when they are about 10 to 12 months old. Talk to the cleft palate team about surgery and post-operative feeding.
Cleft Palate: Feeding Your Baby (PDF)
HH-I-21 8/84, Revised 8/19 Copyright 1984, Nationwide Children’s Hospital
| Feeding a child with cleft lip and palate
Feeding a child with CLP
Babies with only cleft lip and palate do not usually have problems with nipple latch and suction. Whereas children with cleft lip and palate (CLPA) or only cleft palate require a different approach to feeding. The pathological communication between the nasal and oral cavities makes it impossible to create a vacuum in the oral cavity and thus prevents full sucking. As a rule, children with CCLP are transferred to artificial feeding quite early, but even at the same time, during feeding, part of the milk spills out, and swallowed large amounts of air causes frequent, profuse regurgitation. This requires frequent changes in the position of the baby when feeding to facilitate spitting up. The impossibility of proper feeding and mixed breathing in children with CCLP create favorable conditions for the development of inflammatory processes in the ENT organs, lungs and gastrointestinal tract. To avoid these complications, it is necessary to follow a number of simple recommendations.
The pathological communication between the nasal and oral cavities makes it impossible to create a vacuum in the oral cavity and thus prevents full sucking. As a rule, children with CCLP are transferred to artificial feeding quite early, but even at the same time, during feeding, part of the milk spills out, and swallowed large amounts of air causes frequent, profuse regurgitation. This requires frequent changes in the position of the baby when feeding to facilitate spitting up. The impossibility of proper feeding and mixed breathing in children with CCLP create favorable conditions for the development of inflammatory processes in the ENT organs, lungs and gastrointestinal tract. To avoid these complications, it is necessary to follow a number of simple recommendations.
Breastfeeding
There is no doubt that breast milk is the best food for a baby. Therefore, if a mother wants to breastfeed a child with CCLP, there are special recommendations that will facilitate this process.
• Massaging the breast before feeding promotes reflex milk ejection, which in turn makes it easier for milk to flow into the baby's mouth.
• Warm compresses applied to the breasts for 20 minutes before a feed will ensure good blood flow to them.
• Frequent breastfeeding (every 2-3 hours) in the first 2 weeks of life, which contributes to the establishment of normal lactation.
• Finger pressure on the areola (the dark area around the nipple) helps increase nipple prominence, making it easier to grab and hold in your baby's mouth. The nipple will enlarge during breastfeeding.
• To facilitate the feeding of the baby, special pads are used to ensure the normal shape of the nipple.
If, after several attempts, the baby is unable to hold on to the nipple, or if you feel that the baby is not fully satiated, collect the remaining milk with a breast pump and finish feeding this milk from the bottle. In any case, when you are supplementing your baby with a bottle, you should always give the baby the breast first, and only then the bottle. With gradual adaptation, increasing strength and patience of your baby, the process of breastfeeding can become longer.
With gradual adaptation, increasing strength and patience of your baby, the process of breastfeeding can become longer.
When feeding children with cleft palate, obturators (special palatal plates that repeat the curvature of the palate) can be used, as they separate the oral and nasal cavities, providing greater feeding efficiency. However, it should be borne in mind that such devices can damage the oral mucosa. To prevent this complication, fitting the obturator is carried out in the first few days of life. In the process of using the device, it should be tried on and adjusted, periodically replacing it with a new one.
Bottle feeding
In cases where it is not possible to establish a normal sucking force during attachment to the breast, especially in children with bilateral cleft lip and palate, a bottle with a nipple must be used for breast milk feeding. It is advisable to feed the baby with milk expressed using a breast pump for several weeks, and if possible, longer. Modern breast pumps significantly reduce the pumping time and ensure the maintenance of lactation for a long time. Currently, there are ways to harvest breast milk for a certain period. Questions about how and when to store milk should be discussed with your pediatrician.
Modern breast pumps significantly reduce the pumping time and ensure the maintenance of lactation for a long time. Currently, there are ways to harvest breast milk for a certain period. Questions about how and when to store milk should be discussed with your pediatrician.
Artificial feeding
If it is impossible to breastfeed, artificial feeding is used. This uses the same principles as for breastfeeding, with the exception of small additions to the technique. Easier food intake will compensate for the efforts that occur during pathological communication of the oral cavity and nose, especially with wide cleft lip and palate. When choosing a pacifier and a bottle, first of all, feeding efficiency should be taken into account, and it depends on several factors:
• nipple pressure on underlying tissues;
• nipple shapes;
• elasticity of the material from which it is made;
• Diameter of the hole in the nipple - it should not be very large, as the child will choke, and, in addition, under such conditions, he does not need to exert great effort when sucking, and therefore the lower jaw will be underdeveloped.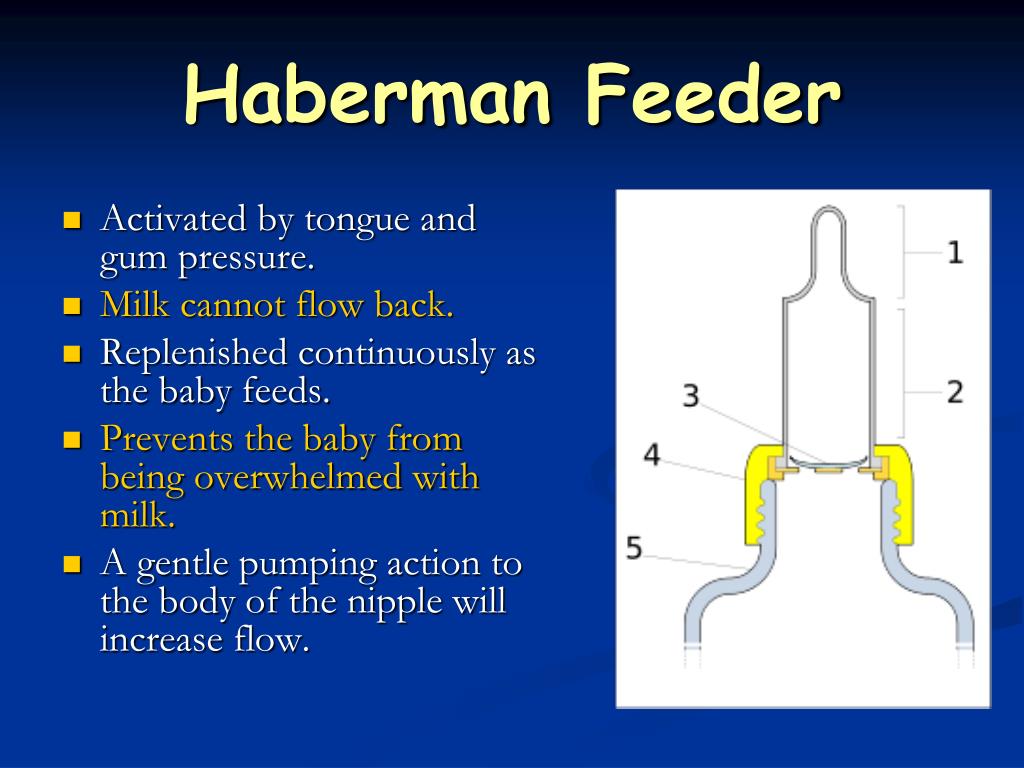
Orthodontic nipples and soft bottles are usually used. To begin with, a soft nipple is suitable for a child, but over time it needs to be changed to a more rigid one, for the optimal development of the baby's chewing muscles.
Recently NUK latex nipples have become popular. They allow you to feed the baby artificially, despite the presence of a cleft. There is no hole in the nipple - it is made individually for each baby in accordance with the doctor's recommendations and depending on the direction of the cleft, but not in the upper part of the nipple that closes the cleft. There should be several holes in the nipple, and their sizes are standard, so that when the bottle is turned upside down, the milk only drips, and does not flow out in a trickle. The nipples have a wide mouthpiece that promotes the natural sucking reflex.
In the process of feeding, it is necessary to control the swallowing of formula or milk. You should not allow the presence of a large volume of the nutrient mixture in the oral cavity. In all children, when using a pacifier, the nutrient mixture enters the oral cavity in drops, while the circular split muscle remains passive, the back of the tongue rises, separating the mouth and nose. At the same time, the most physiological sucking is noted in children, even with a cleft lip and palate.
In all children, when using a pacifier, the nutrient mixture enters the oral cavity in drops, while the circular split muscle remains passive, the back of the tongue rises, separating the mouth and nose. At the same time, the most physiological sucking is noted in children, even with a cleft lip and palate.
Some children with clefts may have difficulty with both very long and very short nipples. Short nipples cannot provide good contact with the tongue and palate, and long nipples can provoke a gag reflex.
One of the ways to regulate the flow of milk into the baby's mouth is the cross hole at the tip of the nipple. Such cuts facilitate the flow of liquid from the bottle. Cross-shaped incisions are very convenient, as they allow the child to regulate the strength and speed of milk flow with a constant sucking rhythm. Simply enlarging the opening in the nipple causes a steady increase in the flow of milk into the baby's mouth, resulting in difficulty in suckling control and disruption of the interaction between swallowing and breathing. On the contrary, a cruciform incision ensures the flow of milk only at the moment of squeezing the nipple. Any nipple can be made into a cross-cut nipple with a regular razor blade. If it is required to make an incision on the orthodontic nipple, then it is better to perform it not at the very top, but a little closer to the lingual surface, as this will contribute to the metered flow of fluid.
On the contrary, a cruciform incision ensures the flow of milk only at the moment of squeezing the nipple. Any nipple can be made into a cross-cut nipple with a regular razor blade. If it is required to make an incision on the orthodontic nipple, then it is better to perform it not at the very top, but a little closer to the lingual surface, as this will contribute to the metered flow of fluid.
Another way to make milk flow easier while conserving baby's energy is to use soft bottles. The compression of such a bottle should be carried out rhythmically and correspond to the frequency of sucking and swallowing food by the child (approximately every 2-3 sips). By following the rhythm of the baby, you can be sure that there will be no excessive intake of milk into the oral cavity and its reflux into the respiratory tract. The bottle must be squeezed and then released without continued compression. Feeding is usually easier if the bottle is angled away from the cleft side of the mouth so that the nipple can be squeezed between the tongue and the remaining normal maxillary alveolar bone and hard palate. Your baby will make the necessary adjustments by adjusting to the position of the nipple, making it easier for him to get milk from the bottle. To do this, it is only necessary to hold the bottle in one position and allow the child to shift the nipple from one corner of the mouth to another.
Your baby will make the necessary adjustments by adjusting to the position of the nipple, making it easier for him to get milk from the bottle. To do this, it is only necessary to hold the bottle in one position and allow the child to shift the nipple from one corner of the mouth to another.
Feeding position
It is very important that the breastfeeding parent finds the most comfortable position for himself. Sometimes, for comfort, it is useful to use a pillow to support the child. It also makes it easier to support the child with a footrest, on which the parent can lean with one or both feet. Since feeding a baby can take up to 30 minutes. several times a day, the adult feeding the baby should find the most comfortable and relaxed position for himself.
The baby should be well supported during feeding, usually in a slightly elevated position, or sitting. This position helps prevent milk from entering the baby's respiratory tract.
While breastfeeding, the mother can use several positions that make the process much easier. The first position is when the child sits on a mattress or pillow, his back is supported by the mother's forearm, and her head is supported by her hand. In this position, gravity helps the nipple to be placed in the baby's mouth.
The first position is when the child sits on a mattress or pillow, his back is supported by the mother's forearm, and her head is supported by her hand. In this position, gravity helps the nipple to be placed in the baby's mouth.
It is very important to push the chest away from the baby's nose so as not to interfere with adequate breathing.
Another position is when the child sits on the mother's lap, facing her, with the child's legs wide apart, embracing the mother's stomach. Sometimes it is necessary to use a pillow in order to lift the child higher.
In order to suckle effectively, the baby's lower jaw must be in a stable position. If the mother supports the child by the lower jaw or chin, then the baby will not get tired so quickly. It is also helpful to have the baby's head turned first to one side and then to the other during feeding. This change allows you to evenly work the circular muscles. When bottle-feeding, it is important that the baby is supported in an elevated position. The nipple should be placed in the area where all the tissues are most preserved.
The nipple should be placed in the area where all the tissues are most preserved.
Help with food in the nose
Even when a fed baby is in a semi-elevated position, there is a risk of milk getting into the nose (nasal regurgitation). Sometimes such regurgitation can be associated with a sudden change in body position. Parents should not worry too much about this, as food entering the nose is quite common at first. It does not harm the baby and will gradually decrease as the baby grows. When regurgitation occurs, it is necessary to temporarily stop feeding and give the baby some time to cough or sneeze. This will allow the baby to clear the nasal passages and you can continue feeding. However, if the child has persistent regurgitation and the cough is frequent and severe, you should consult your doctor.
Solid food introduction
Your child should be ready for pureed food at the same age as other children. Pureed food should be introduced at 4-6 months. Feeding should be done with a spoon, not a bottle. At the same time, the transition from an elevated position to a sitting position reduces the number of episodes of regurgitation. Initially, the child should receive a small amount of liquid (no lumps) cereal porridge mixed with artificial formula until he can feel the pieces of food in his mouth. The child must be gradually accustomed to more adult food, which takes time and patience. At first, the baby will try to absorb new food, which can again lead to episodes of food entering the nose. In these cases, give the child some water to drink. As soon as the child learns to swallow food, the density of the porridge can be increased by mixing it with less milk.
Feeding should be done with a spoon, not a bottle. At the same time, the transition from an elevated position to a sitting position reduces the number of episodes of regurgitation. Initially, the child should receive a small amount of liquid (no lumps) cereal porridge mixed with artificial formula until he can feel the pieces of food in his mouth. The child must be gradually accustomed to more adult food, which takes time and patience. At first, the baby will try to absorb new food, which can again lead to episodes of food entering the nose. In these cases, give the child some water to drink. As soon as the child learns to swallow food, the density of the porridge can be increased by mixing it with less milk.
Frequently Asked Questions
1. How often does a child need to burp air?
Frequent spitting up usually occurs in children who swallow large amounts of air during feeding. The baby usually signals the impending regurgitation by slowing down or stopping suckling. It is at this time that the child should be given the opportunity to burp, and not at the moment of active sucking.
It is at this time that the child should be given the opportunity to burp, and not at the moment of active sucking.
2. Does the cleft area need to be cleaned?
A child's mouth, whether or not it has a cleft, tends to clean itself. Some newborns with cleft lip do not need additional cleaning, but this decision should be made with your pediatrician. A small amount of curdled milk in the area of the cleft can be successfully removed by giving the child a few sips of water. In any case, a small, gentle wipe over the child's face and mouth with a damp cloth may be required. The use of cotton swabs or rinsing with a syringe is not recommended, as this can damage the delicate lining of the child's mouth.
3. How to feed during the early postoperative period?
The surgeon who will operate on your child will definitely tell you about the peculiarities of feeding the baby after the restoration of the lip or palate. Mostly, parents should change the way of feeding immediately after surgery, and then the usual way of feeding will be restored. You will no doubt receive advice on restrictions and the introduction of a new way of feeding a few weeks before the operation in order to gradually get used to this method.
You will no doubt receive advice on restrictions and the introduction of a new way of feeding a few weeks before the operation in order to gradually get used to this method.
4. When can cup feeding be introduced?
A cleft baby can be cup fed at the same time as other babies. Most children are ready for this way of eating at the age of 8-9 months. Drinking from a cup does not adversely affect the newly operated lip and will allow you to return to your usual way of feeding after surgery. Since bottle-feeding is not allowed after a palatoplasty, gradually weaning your baby from bottle-feeding will allow you to avoid unnecessary whims after the operation.
The experience of feeding a child is extremely important for both parents and their child. Newborn children adapt more easily, and infants learn faster if the parents have the necessary support, patience and love. Remember that there are many experienced professionals ready to provide you with the support you need.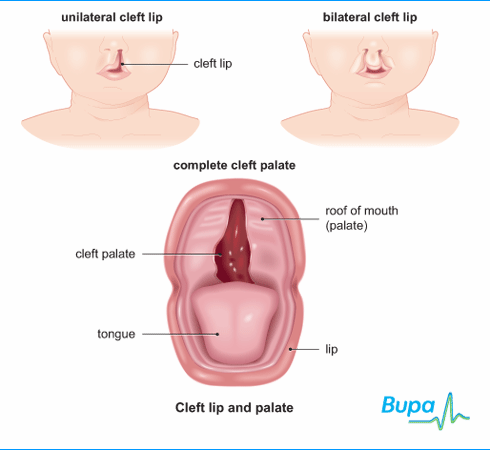
How to feed a child with a congenital cleft lip and/or palate - Baby's Face
According to the official statistics of the World Health Organization, published in April 2012, every 500-700 people on earth are born with a congenital cleft lip and/or palate. Thanks to advances in the field of maxillofacial surgery, operations to eliminate this defect are very successful today. Whether earlier or later, any child born in the Russian Federation must be operated on without fail. Another question is that until the surgeons do their job, parents will have to learn how to water and feed the child so that he grows and develops just like his peers.
That is why it is so important for young parents to take this process seriously. Most likely, in the maternity hospital, you will be advised to try to keep the baby on breast milk as long as possible, ensure the maximum vertical position of the baby's body when feeding, and also observe hygiene. And so, the recommendations were given, the child was discharged, and then questions arise, the answers to which parents have to look for by trial and error.
If, despite a birth defect, your baby is able to latch on, don't bottle just because it's more comfortable for you. The sucking reflex, developed during feeding, is important for the correct formation of the bite and maxillofacial apparatus, and will also play a role in the development of speech. Remember that breast milk is the best food for your baby.
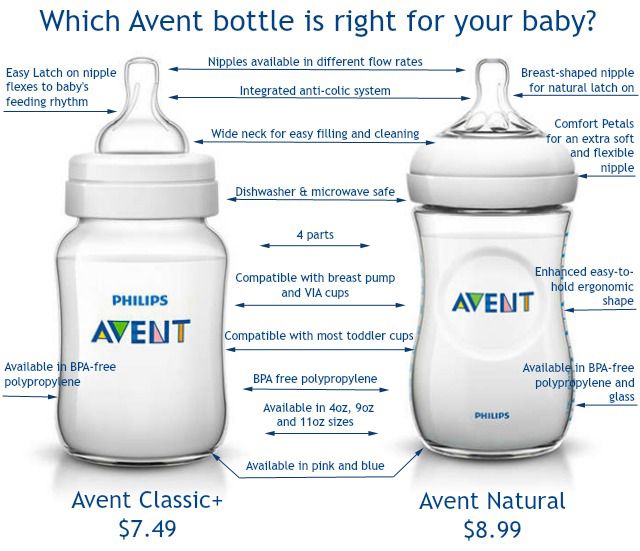
If breastfeeding is not possible for one reason or another, do not despair. The modern market offers bottles and nipples for them in various shapes and from various materials. Instead of hard silicone, a more pliable latex may suit a child, you may prefer a plastic bottle to a heavy glass bottle, and if you have to dilute the mixture in it, then the one that has already been marked in milliliters will be convenient. The main thing is to take care of children's dishes. Before the first and each subsequent use, the nozzle should be boiled and sterilized for 5 minutes. “Never wash nipples in the dishwasher, as this can damage the material. When heated in the microwave, filled and closed bottles may explode or be damaged. It is also important to remember that when food is heated in this way, it heats up unevenly, which can lead to burns.
When heated in the microwave, filled and closed bottles may explode or be damaged. It is also important to remember that when food is heated in this way, it heats up unevenly, which can lead to burns.
As mentioned above, keep your baby as elevated as possible while feeding to reduce the chance of unwanted choking. Some manage to adapt an ordinary pillow for this, others - a child seat allowed for newborns, the third finds it convenient to feed children in a 0+ car seat.
Unfortunately, when a child with a cleft palate, in particular, drinks from a bottle, he sometimes needs to take frequent breaks, and when he is in a hurry, some of the milk may spill out of the spout. This is not a great danger - such are the costs of this defect. But you should always remember this and keep a napkin or diaper on hand in order to quickly wipe your nose. The child may have to move around to continue eating afterwards. Some babies are more comfortable eating smaller portions, but 1-2 more feedings than others at the same age.
When buying teats, you should pay attention to the fact that the packages are traditionally marked with the age category of children for whom they are intended (0-6, 6+/9+). The difference is in the width of the nipple itself, and in the diameter of the hole through which the liquid enters: a small hole for breast milk or water, a medium one for breast milk substitutes, a large one for thicker foods. There are even those whose manufacturers, instead of the traditional round shape, apply cruciform notches that allow older children to switch to very liquid cereals.
If you feel that your baby is not strong enough to eat through a silicone nipple, you can offer a latex one, but be aware that this material loses its shape very quickly and becomes brittle, which can injure the baby's delicate tongue or cause the nipple itself to burst. “Check the nipple before each use for signs of wear by stretching it in all directions, especially if the baby already has teeth. If there are signs of aging, cracks or bite marks, replace it, as the child may swallow the separating parts. For hygiene and safety reasons, nipples should be changed every 1-2 months,” the manufacturers of latex nipples recommend. To facilitate the process, you can use several nipples: start feeding from the older one, and finish from the newer one, so you will always have 2-3 softened nipples.
For hygiene and safety reasons, nipples should be changed every 1-2 months,” the manufacturers of latex nipples recommend. To facilitate the process, you can use several nipples: start feeding from the older one, and finish from the newer one, so you will always have 2-3 softened nipples.
Some parents try to make large holes in the nipples themselves, but at home it is impossible to achieve complete sterility of the needle, therefore, in order to avoid the negative consequences of this kind of amateur activity for the health of the child, try different nipples from different manufacturers to find one that will be comfortable, and most importantly - safe for your child.
In most cases, parents manage to adapt to feeding their baby, but for those who cannot find a comfortable shape, Medela (Switzerland) offers two alternative options: a soft spoon SoftCup and a Habermann sippy cup.
The soft spoon is a bottle with a special valve and a self-filling reservoir that makes it easy to dose food, and the special design prevents milk from spilling.