Not enough milk to feed baby
Low Milk Supply | WIC Breastfeeding Support
Many moms worry about low milk supply, but most of the time your body makes exactly what your baby needs, even if you don't realize it. There are also ways to tell if your baby is getting enough milk. If you aren't making enough, there are ways you can build your supply. And your WIC breastfeeding staff is always there to help!
Am I Making Enough Milk?
First, look for these signs that your baby is getting enough milk. For example, pay attention to the number of wet and dirty diapers and your baby's weight gain.
Things you should NOT worry about:
- How your breasts feel. Your breasts will feel softer and less full as your milk supply adjusts to your baby's needs. This does not mean you have low supply.
- If your baby nurses for shorter periods of time, such as only 5 minutes on each breast.
- If your baby's feeds are bunched together. This is called cluster feeding and happens when your baby starts nursing more often and for longer.
This can happen in the evenings or because of growth spurts.
- Not getting much milk when you express. Your baby is much more effective than a pump or hand expression at getting out milk. Find tips to help you pump.
If you are still concerned, talk to your baby's doctor about their growth.
Causes of Low Milk Supply
While most moms make plenty of milk, some do have low milk supply. This might happen if you:
- Limit your baby's breastfeeding sessions. Remember, the more you feed on demand, the more milk you make.
- Give your baby infant formula instead of breastfeeding.
- Introduce solid foods before baby is 4-6 months old.
- Take certain birth control pills or other medicine.
- Don't get enough sleep.
- Drink alcohol or smoke.
- Have had breast surgery.
Talk to your doctor if you have hepatitis B or C, herpes, or diabetes. These conditions may also affect milk supply.
Increasing Your Milk Supply
Breastfeeding frequently—especially in the first hours, days, and weeks—is the main way to increase your milk supply. Your body will make milk to meet your baby's demand.
Try these tips to help you make more milk:
- Breastfeed every time your baby is hungry. In the early weeks, your baby will eat 8-12 times every 24 hours. It's best not to put your baby on a strict feeding schedule. Follow your baby's cues, and let your baby tell you when it's time to eat.
- Make sure your baby is latching well.
- Offer both breasts at each feeding. Let your baby finish the first side, then offer the other side.
- Empty your breasts at each feeding.
 Hand express or pump after a feeding to draw out all the milk and signal your body to make more.
Hand express or pump after a feeding to draw out all the milk and signal your body to make more. - Avoid bottles and pacifiers in the early weeks. Feed your baby from your breast whenever you can.
- Get plenty of sleep, and eat a healthy diet.
- Pump or express your milk. Pumping or expressing milk frequently between nursing sessions, and consistently when you're away from your baby, can help build your milk supply.
- Relax and massage. Relax, hold your baby skin-to-skin, and massage your breasts before feeding to encourage your milk to let down.
- Take care of yourself. Get plenty of rest, eat well, drink enough fluids, and let others help you.
Consider Charting Your Progress
Record how often your baby is breastfeeding, for how long, and on which sides. If you are supplementing with infant formula, record how much your baby is getting and decrease the infant formula as your milk supply increases. WIC breastfeeding staff can help you determine how much infant formula your baby needs.
WIC breastfeeding staff can help you determine how much infant formula your baby needs.
Still Have Questions?
Contact your WIC breastfeeding expert. They can talk to you about supply concerns and give you tips to increase your supply to meet your baby's needs.
10 reasons for low milk supply, plus tips to increase breast milk
Lactation expert, Teresa Pitman, discusses the top 10 reasons for low milk production and offers tips to find a solution
When baby’s fussy or wants to nurse just an hour after eating, it’s natural to worry that you’re not producing enough milk. However, these are normal behaviours and more often than not baby’s weight gain reassures everyone that things are going well. However, for some mothers the results of baby’s weight checks aren’t as encouraging and they may be experiencing low milk supply. Diana West, IBCLC (International Board-Certified Lactation Consultant) and co-author of Making More Milk says that changes in breastfeeding techniques or assistance from a breastfeeding expert can help boost milk production significantly.
Here are some of the most common reasons for low milk supply and some strategies that may help.
1. Insufficient glandular tissueSome women’s breasts don’t develop normally (for various reasons) and may not have enough “milk-making” ducts to meet their baby’s needs. Ducts do grow during each pregnancy and breastfeeding stimulates the growth of more ducts and tissue, so this may be less of a problem with a second or third baby. There are certainly steps you can take to maximize your milk production (these might include pumping and taking a prescription medication–talk to your doctor and a breastfeeding expert) but you may also need to supplement a low milk supply with formula. It’s worth the effort to continuing breastfeeding, though, as even a small amount of your milk will help support your baby’s immune system, brain development and nutritional needs.
2. Hormonal or endocrine problemsPerhaps you have polycystic ovary syndrome (PCOS), a low or high thyroid, diabetes, hypertension (high blood pressure) or hormonal problems that made it difficult for you to conceive. Any of these issues may also contribute to low milk supply because making milk relies on the hormonal signals being sent to the breasts. What can you do? In some cases, treatment of your health problem will help you to boost milk production, although supplementation may be needed. A visit to a breastfeeding clinic or lactation consultant can help you find an approach that will work with your specific condition.
Any of these issues may also contribute to low milk supply because making milk relies on the hormonal signals being sent to the breasts. What can you do? In some cases, treatment of your health problem will help you to boost milk production, although supplementation may be needed. A visit to a breastfeeding clinic or lactation consultant can help you find an approach that will work with your specific condition.
Breast surgeries can be done for both medical and cosmetic reasons. Breast reductions or enhancements, for example, are increasingly common. Nipple piercings can also be considered a kind of breast surgery and may damage milk ducts in the nipple. How much these surgeries affect breastfeeding varies widely, depending on how the procedure was done, how much time has passed between the surgery and the birth of the baby and whether there were any complications that might have caused scarring or damage to the breasts. Some women, especially those with breast enhancements rather than reductions, may be able to exclusively breastfeed without any difficulty. Others will need extra help and may have to supplement.
Some women, especially those with breast enhancements rather than reductions, may be able to exclusively breastfeed without any difficulty. Others will need extra help and may have to supplement.
Many mothers who breastfeed and take birth control pills find their milk production doesn’t change, but for some, any form of hormonal birth control (the pill, patch or injections) can cause a significant drop in their milk. This is more likely to happen if you start using these contraceptives before your baby is four months old, but it can happen later as well. The first step to increasing your milk supply again is to stop the medication, but talk to your doctor before you do and be prepared to change birth control methods. Some mothers also need extra help (such as a prescription medication, herbal supplements and/or pumping) to boost milk production.
5. Taking certain medications or herbsPseudoephredine (the active ingredient in Sudafed and similar cold medications), methergine, bromocriptine or large amounts of sage, parsley or peppermint can affect your milk. If you find your milk supply has dropped and realize you have taken one of the medications listed here, ask your doctor about an alternative treatment for your cold or health ailment. Increased breastfeeding and possibly pumping will help you build up your milk production again.
If you find your milk supply has dropped and realize you have taken one of the medications listed here, ask your doctor about an alternative treatment for your cold or health ailment. Increased breastfeeding and possibly pumping will help you build up your milk production again.
The problem may not even be low milk supply, but lie with your little one; it may be difficult for him to get the milk from your breasts. He may, for example, have a tongue-tie. That means the thin membrane of tissue at the bottom of his mouth is holding the baby’s tongue too tightly, so that he’s not able to use it properly to extract the milk. (A baby doesn’t really suck the milk out of your breast, he uses his tongue to help compress the breast and push the milk into his mouth.) In many cases this is fairly easy to see, but for some babies the restricting membrane is at the back of the tongue and harder to identify. Check to see if your baby is able to stick his tongue out (over his bottom lip) and that he touches it to the roof of his mouth when crying. If your baby is tongue-tied, the membrane can be clipped by a doctor and the baby’s ability to breastfeed will improve quickly. Other problems can also cause sucking difficulties (such as cleft lip and cleft palate), so if you suspect your baby isn’t feeding well, check with an expert or your doctor.
If your baby is tongue-tied, the membrane can be clipped by a doctor and the baby’s ability to breastfeed will improve quickly. Other problems can also cause sucking difficulties (such as cleft lip and cleft palate), so if you suspect your baby isn’t feeding well, check with an expert or your doctor.
There are many books and programs that offer sleep-training methods to get babies to sleep longer at night without waking for feedings. While these techniques can work for some families, the loss of those night feedings can mean problems with weight gain for some babies. Why? Mothers vary a lot in how much milk they are able to store in their breasts between feedings.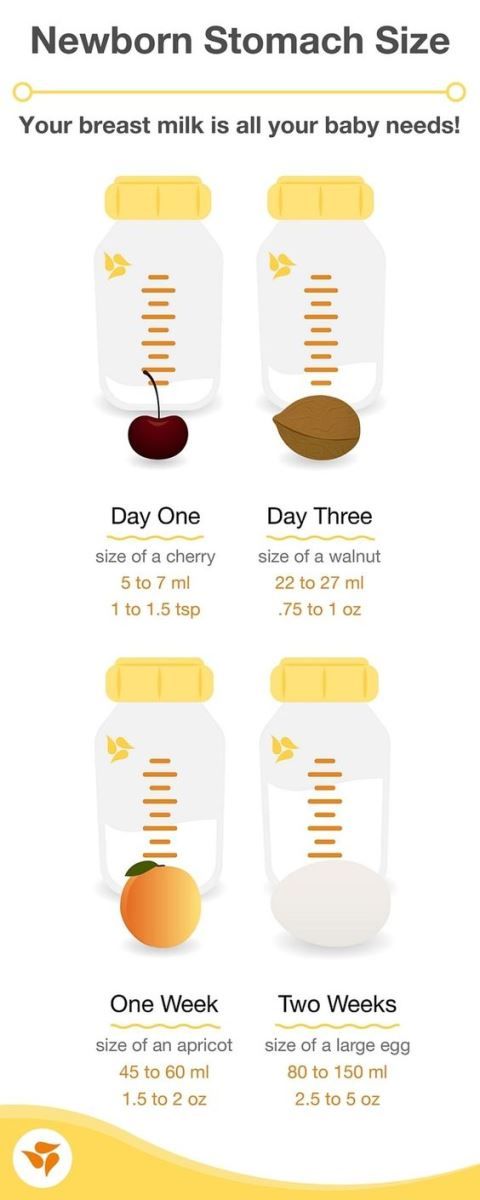 With no feedings overnight, their milk supply starts to drop. The level of prolactin (the hormone that signals the breasts to make milk) is also higher during night feedings, so the lowered overall prolactin can also contribute to a drop in milk. It’s hard to resist the lure of more sleep, but for many mothers, those nightly feedings are essential to avoid low milk supply. If you have started sleep training and find your milk supply going down, consider reintroducing one or two night feedings.
With no feedings overnight, their milk supply starts to drop. The level of prolactin (the hormone that signals the breasts to make milk) is also higher during night feedings, so the lowered overall prolactin can also contribute to a drop in milk. It’s hard to resist the lure of more sleep, but for many mothers, those nightly feedings are essential to avoid low milk supply. If you have started sleep training and find your milk supply going down, consider reintroducing one or two night feedings.
Your breasts make milk continuously, but the rate at which milk is made depends on how empty they are. You’ll make more milk when your breasts are close to empty and less milk when they are already filled up. When your baby is feeding infrequently, because you have put him on a three- or four-hour schedule for example, or because you are giving him a pacifier to stretch out the time between feedings, your breasts are fuller for longer periods of time. That means milk production slows down. When babies are breastfed in response to their cues, they tend to have shorter, frequent feedings and this means the breasts are emptier most of the time and so they continue to produce plenty of milk.
That means milk production slows down. When babies are breastfed in response to their cues, they tend to have shorter, frequent feedings and this means the breasts are emptier most of the time and so they continue to produce plenty of milk.
Mothers don’t always realize that medications used in labour, such as epidural anaesthetic or Demerol, can affect the baby’s ability to latch on and breastfeed effectively. Some studies show these effects last as long as a month, depending on the medication used in the epidural and the length of time the mother received it. Jaundice, a common condition in newborns, can also make your baby sleepier than usual, so that he doesn’t wake up to nurse as often as he would otherwise. In both cases, you may need to pump your milk to build up a good supply. Once your baby has cleared the medications from his system and the jaundice has been treated, he will probably begin nursing well and you’ll be able to reduce and eventually stop pumping.
Especially in the first couple of weeks, supplementing with formula tricks your breasts into producing less milk. “In the early weeks, the breasts’ capacity for milk production is calibrated in response to the amount of milk that is removed,” says lactation consultant Diana West. “If less milk is removed, the breasts assume that less milk is needed, so the capacity is set at a lower point.” When your baby is given formula supplements, she naturally eats less at the breast, and the breasts respond by making less milk. If supplementation is necessary, pumping as well as breastfeeding can help to promote a higher volume of milk production.
If your baby is showing signs of not getting enough milk, don’t throw away your nursing bra just yet. Talk to a La Leche League leader, lactation consultant or other breastfeeding expert who can help you figure out and treat the cause of your low milk supply.
When you need to supplement breast milkIf you do experience low milk supply, you’ll need to give your baby some formula as well. Usually this is temporary, until your own milk supply increases or until your baby starts enough solid foods that the supplement isn’t needed. But too many mothers find that once they start giving formula they’ve take the first step on a path that leads to decreasing milk production and an early end to breastfeeding. But there are ways to successfully supplement and still keep breastfeeding. Try these approaches:
Usually this is temporary, until your own milk supply increases or until your baby starts enough solid foods that the supplement isn’t needed. But too many mothers find that once they start giving formula they’ve take the first step on a path that leads to decreasing milk production and an early end to breastfeeding. But there are ways to successfully supplement and still keep breastfeeding. Try these approaches:
Consider supplementing at the breast with a feeding tube that has one end in a container of formula and the other slipped into the baby’s mouth as he breastfeeds. Some mothers will tape the tube to their breasts, while others slide it into the corner of the baby’s mouth as he nurses. This method ensures that the baby gets both formula and breast milk at the same time and he’s encouraged to keep breastfeeding.
If you are supplementing with a bottle, give the bottle first and breastfeed second. Put a bit less formula in the bottle than you expect the baby to take. By giving the bottle first, the baby isn’t frantically hungry when he comes to the breast and may be more willing to work at learning to breastfeed well. He also gets to experience having a full tummy while he’s at the breast, which gives him positive feelings about breastfeeding. Let him nurse as long as he wants.
He also gets to experience having a full tummy while he’s at the breast, which gives him positive feelings about breastfeeding. Let him nurse as long as he wants.
When you give a bottle to supplement breastfeeding, take your time. Hold the baby in a semi-upright position (not lying on his back) and keep the bottle horizontal so that he has to work to suck the milk out. If he pauses or stops sucking, you can take the nipple out of his mouth to give him a little rest. This keeps the baby from expecting milk to just pour into his mouth (as it can with a fast-flowing bottle nipple when the bottle is held in a more vertical position), so he’s more willing to work at breastfeeding.
Encourage plenty of breastfeeding times that aren’t about food. If your baby gets fussy an hour or two after formula and nursing, offer the breast again. She might only nurse for a short time, but these brief but frequent feedings actually do a lot to encourage milk production and continued breastfeeding.
Watch Baby Grow!
Subscribe to Today’s Parent’s baby newsletter and find out what to expect for every stage and milestone, from birth to two years.- Email*
- Baby's due/birth date*
Month223456789101112
Day12345678910111213141516171819202122232425262728293031
Year2024202320222021
- CAPTCHA
- Consent*
Yes, I would like to receive Today's Parent's Baby newsletter. I understand I can unsubscribe at any time.**
FILED UNDER: baby health Breast milk breastfeeding problems health service seo Maternal health Milk consumption New baby New mom
Signs of lack of milk | Improving lactation
Many mothers are concerned about insufficient milk production, but it is not always easy to find out if milk is really low. Read our article to understand if this is true and what can be done about it.
Share this information
“Do I have enough milk?” - a question that is often asked by young mothers. If your baby is healthy and growing well, there is no reason to worry. However, if you are still worried about milk production, it is best to consult a specialist as soon as possible. If everything is in order, he will be able to calm you down. In addition, you will not needlessly feed the baby formula, because of which milk production can really decrease.
Causes of insufficient milk supply
Some mothers do not produce enough breast milk for medical reasons, which include: approximately three days after birth). 1
 3
3 If you have any of the conditions listed, contact your lactation consultant or healthcare provider.
How milk is produced
With the advent of milk, the breast begins to work on the principle of supply and demand. Each time after it is emptied, whether it is feeding the baby or pumping, even more milk will be produced.
This is why milk production may be reduced if you give formula to your baby - your body will not get the signal to produce more milk because it will remain.
The way your baby eats also affects milk production. The more often and better he sucks the breast, the bigger it will be. If your baby eats only a small portion at one feeding, it is necessary to express milk regularly to maintain the level of its production. Read more about this below.
Signs that the baby is not getting enough milk
Although low milk production is rare, the baby may have difficulty feeding in the first few weeks, but for other reasons.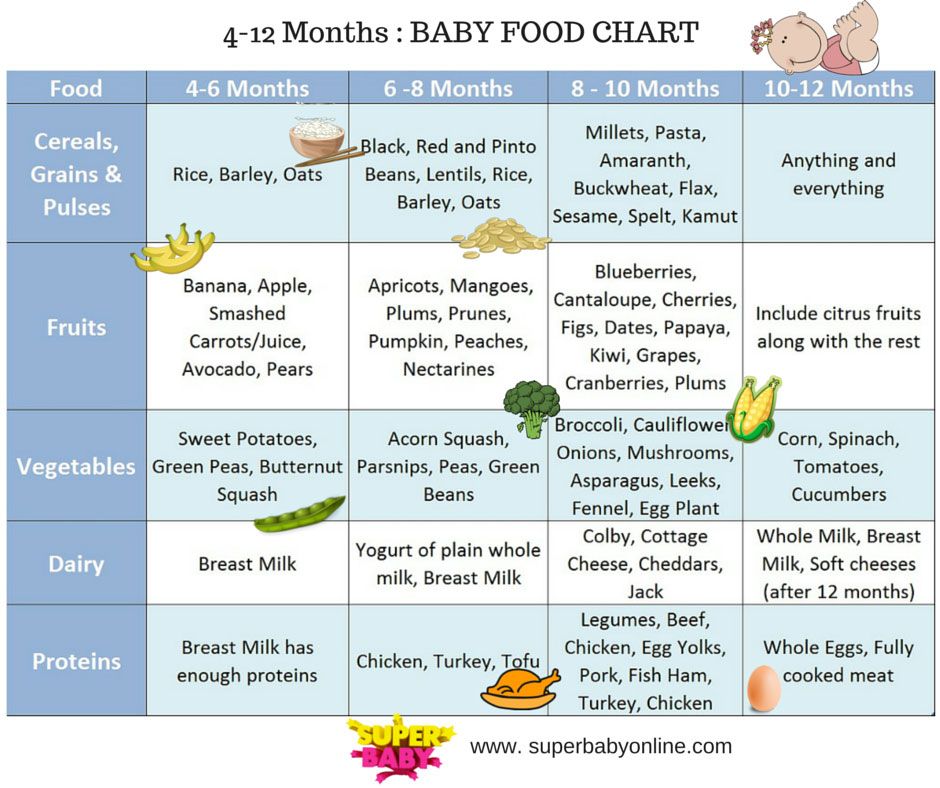 You may not be feeding him often enough or for enough time, especially if you're trying to stick to a specific schedule. The baby may not latch on properly, or it may have features that make it difficult to take in milk.
You may not be feeding him often enough or for enough time, especially if you're trying to stick to a specific schedule. The baby may not latch on properly, or it may have features that make it difficult to take in milk.
The following signs indicate that the baby is not getting enough milk:
- Poor weight gain. In the first few days of life, newborns normally lose 5 to 7%, and sometimes even up to 10%, of their birth weight. However, after that, they should gain at least 20–30 g per day and regain their birth weight by 10–14 days. 5,6,7 If your baby has lost 10% or more of their weight in the early days, or has not started gaining weight by 5-6 days, you should contact your doctor immediately.
- Not enough wet and soiled diapers. A good indicator of whether a baby is getting enough milk is the number of diapers used per day. Check out our article detailing the norm for wet and soiled diapers in Breastfeeding Your Newborn: What to Expect in the First Week.
 Seek medical advice if something bothers you or you notice that the number of soiled diapers has begun to decrease.
Seek medical advice if something bothers you or you notice that the number of soiled diapers has begun to decrease. - Dehydration. If your baby has dark urine, dry mouth or jaundice (yellowing of the skin or eyes), or baby is lethargic, has lost appetite, and may be dehydrated. 6 Dehydration can be caused by fever, diarrhoea, vomiting or overheating. If you notice any of these symptoms, seek medical attention as soon as possible.
Misconceptions about lack of milk
Newborns usually eat very frequently, about 10-12 times a day or every two hours. This does not mean that they do not have enough milk. Keep in mind that breastfeeding is also about comfort, so it's hard to tell how much milk a baby eats at each feed as the amount can vary.
You have enough milk even if:
- the child wants to eat often;
- the child does not want to be laid down;
- the child wakes up at night;
- feeding is fast;
- feeding takes a long time;
- after feeding, the child takes another bottle;
- Your breasts are softer than in the first weeks;
- milk does not leak or has stopped leaking;
- You cannot express much milk;
- You have small breasts.
What to do about insufficient milk production
If you suspect that your baby is not getting enough milk, contact a lactation consultant or your doctor. He will determine if you have enough milk and check how the baby is latch-on and if he is getting enough milk. He may also suggest changing the feeding position or the way the baby is attached to the breast to make it easier.
Also try holding your baby close to you more often to increase skin-to-skin contact before and during feedings. This stimulates the production of the hormone oxytocin, which promotes milk flow. Use relaxation techniques, such as listening to your favorite soothing music, to reduce anxiety that can negatively impact milk production. 8
With proper support, most under-lactating mothers can breastfeed their babies at least partially, and some manage to normalize production.
If your baby is unable to get enough milk directly from the breast (perhaps because he was born prematurely or has special needs), you need to express milk to support his production. Your doctor may prescribe you special drugs that stimulate lactation.
Your doctor may prescribe you special drugs that stimulate lactation.
If you are unable to express enough milk, you will need to supplement your baby with donor milk or formula. This should also take place under the supervision of a physician. The Supplemental Nursing System (SNS)* is a great way to help your baby get all the milk he needs at the breast.
How to increase your milk production with a breast pump
If you need to increase your milk production in the first five days after giving birth, you can use a dual electronic breast pump with lactation start technology, such as the Medela Symphony**. Such a breast pump imitates the sucking of the breast by a child and helps to increase milk production in the future. 9
After your milk comes in, double pumping allows you to get more milk in less time. 10 This method helps to better empty the breast, which also improves lactation.
Although every mother is different, it is often recommended to express milk immediately or one hour after a feed. This may seem strange, since it is usually easier to express milk from a full breast. However, the pumping session should be seen as an "investment in tomorrow."
This may seem strange, since it is usually easier to express milk from a full breast. However, the pumping session should be seen as an "investment in tomorrow."
You will probably only be able to express a little milk at first, but don't be discouraged - if you express regularly, your milk supply will increase. Try to empty your breasts - by putting your baby to your breast or expressing milk - 8 to 12 times a day, including one nightly session, when your levels of prolactin (the hormone responsible for producing milk) are highest. The more often you empty your chest, the better. After two to three days of regular pumping, you will notice a significant increase in milk production. For tips on how to get more milk with every pump, see Tips for Using a Breast Pump.
Pumping with massage to get more milk
If your baby is not lating at all or you are not yet able to express enough milk for him, a technique called “massage pumping” may be helpful. It helps mothers increase the amount of milk they get in one pumping session. 11.12 The whole process takes about 25-30 minutes. Remember that the better you empty your breast, the faster milk is produced in it.
11.12 The whole process takes about 25-30 minutes. Remember that the better you empty your breast, the faster milk is produced in it.
A few simple steps are required:
- Massage your breasts.
- Perform a double pump while wearing a special bustier top that allows you to keep your hands free.
- While expressing, squeeze the chest with all fingers for a few seconds. Release and repeat. Squeeze both breasts until the milk flows in a thin stream.
- Massage the chest again.
- Express milk manually or with a single breast pump, squeezing each breast in turn to empty them as completely as possible.
When your baby starts to gain weight and milk production increases, you can switch to exclusive breastfeeding.
Literature
1 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia. 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." J Mammary Gland Biol Neoplasia. 2007;12(4):211-221. 9 E et al . Breastfeeding in polycystic ovary syndrome. Acta Obstet Gynecol Scand. 2008;87(5):531-535. - Wanky, I. et al., "Breastfeeding in the setting of polycystic ovaries." Akta Obstet Ginecol Scand. 2008;87(5):531-535.
- Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." J Mammary Gland Biol Neoplasia. 2007;12(4):211-221. 9 E et al . Breastfeeding in polycystic ovary syndrome. Acta Obstet Gynecol Scand. 2008;87(5):531-535. - Wanky, I. et al., "Breastfeeding in the setting of polycystic ovaries." Akta Obstet Ginecol Scand. 2008;87(5):531-535.
3 Neifert MR et al. Lactation failure due to insufficient glandular development of the breast. Pediatrics. 1985;76(5):823-828. - Neifert M.R. et al., "Inability to Lactate Due to Deficiency of Glandular Breast Tissue". Pediatrix (Pediatrics). 1985;76(5):823-828.
4 Neifert M et al. The influence of breast surgery, breast appearance, and pregnancy-induced breast changes on lactation sufficiency as measured by infant weight gain. Birth. 1990;17(1):31-38. - Neifert M. et al., "Influence of breast surgery, breast appearance, and pregnancy-induced breast changes on milk supply as measured by weighing the baby." Bers. 1990;17(1):31-38.
Birth. 1990;17(1):31-38. - Neifert M. et al., "Influence of breast surgery, breast appearance, and pregnancy-induced breast changes on milk supply as measured by weighing the baby." Bers. 1990;17(1):31-38.
5 C Tawia S, McGuire L. Early weight loss and weight gain in healthy, full-term, exclusively-breastfed infants. Breastfeed Rev . 2014;22(1):31-42. - S. Tavia S., McGuire L., "Natural Weight Loss and Gain in Healthy, Exclusively Breastfed Full-Term Infants." Brestfeed Rev (Breastfeeding Review). 2014;22(1):31-42.
6 Lawrence RA, Lawrence RM. Breastfeeding: A guide for the medical profession. 7th ed. Maryland Heights MO, USA: Elsevier Mosby; 2010. 1128 p . - Lawrence R.A., Lawrence R.M., "Breastfeeding: A guide for healthcare professionals." Seventh edition. Publisher Maryland Heights , Missouri, USA: Elsevier Mosby; 2010. P. 1128.
P. 1128.
7 World Health Organization. [Internet]. Neonatal Care . 2012;12(2):112-119 - Keith D.R. et al., "Effects of listening to music on the amount, fat content, composition and calorie content of breast milk in mothers of premature and seriously ill children." Adv Neonatal Care. 2012;12(2):112-119
9 Meier PP et al. Breast pump suction patterns that mimic the human infant during breastfeeding: greater milk output in less time spent pumping for breast pump-dependent mothers with premature infants. J. Perinatol. 2012;32(2):103-10. - Meyer P.P. et al., "Pumping patterns that mimic breastfeeding behavior: more milk and less time for constantly pumping mothers of preterm infants." J Perinatol (Journal of Perinatology). 2012;32(2):103-10.
10 Prime DK et al. Simultaneous breast expression in breastfeeding women is more efficacious than sequential breast expression. Breastfeed Med . 2012;7(6):442-447. - Prime D.K. and co-authors. "During the period of breastfeeding, simultaneous pumping of both breasts is more productive than sequential pumping." Brestfeed Med (Breastfeeding Medicine). 2012;7(6):442-447.
Breastfeed Med . 2012;7(6):442-447. - Prime D.K. and co-authors. "During the period of breastfeeding, simultaneous pumping of both breasts is more productive than sequential pumping." Brestfeed Med (Breastfeeding Medicine). 2012;7(6):442-447.
11 Stanford University School of Medicine [Internet]. Stanford, CA, USA: Maximizing Milk Production with Hands-On Pumping; 2017. [ Accessed 04/30/2018]. - Stanford University School of Medicine [Internet]. Stanford, CA, USA: "Increased milk production from hand expression"; 2017. [Page accessed 04/30/2018].
12 Morton J et al. Combining hand techniques with electric pumping increases milk production in mothers of preterm infants. J. Perinatol. 2009;29(11):757-764. - Morton J. et al., "Manual pumping combined with an electric breast pump increases breast milk production in mothers of preterm infants. " J Perinatol (Journal of Perinatology). 2009;29(11):757.
" J Perinatol (Journal of Perinatology). 2009;29(11):757.
Read instructions before use. Consult a specialist about possible contraindications.
* RU No. ФСЗ 2010/07352 dated 07/19/10
** RU No. ФСЗ 2010/06525 dated 03/17/2021
Breastfeeding a newborn | What to Expect in the First Week
The first week of a baby's life is a wonderful but hectic time, especially if you haven't breastfed before. Our breastfeeding tips will help you settle in as quickly as possible
Share this information
The first time after giving birth, mothers are often confused. The body is still recovering, and you are already starting to get to know your newborn baby. The emotional state during this period can be unstable, especially between the second and fifth days, when many women have milk 1 and at the same time postpartum depression begins 2 . In addition, people around often expect (and demand) that a woman come to her senses as soon as possible and become a “super mom”. But the best thing to do this first week is just to be with your baby and get breastfeeding going.
But the best thing to do this first week is just to be with your baby and get breastfeeding going.
When should I start breastfeeding my newborn?
Try to breastfeed your baby within the first hour after birth. When the baby latch onto the breast and begins sucking rhythmically, it stimulates the mammary gland cells and starts milk production. 1 It is not for nothing that this time is called the “magic hour”!
“Ideally, the baby should be placed on the mother's stomach immediately after birth so that it can immediately attach to the breast. He won't necessarily eat, but he should be able to,” explains Cathy Garbin, an internationally recognized expert on breastfeeding.
“Hold your baby and let him find the breast on his own and put the nipple in his mouth. This is called the breast-seeking reflex. On the Internet you can watch videos that show what this process looks like. If the baby does not latch onto the nipple on its own, the midwife will help to properly attach it to the breast. But for starters, it’s good to give the baby the opportunity to do it on their own. In this case, the optimal position for the mother is reclining. ”
But for starters, it’s good to give the baby the opportunity to do it on their own. In this case, the optimal position for the mother is reclining. ”
Don't spend that special first hour of your baby's life weighing and swaddling—or at least wait until he's suckling for the first time. Enjoy hugs and close skin-to-skin contact. This promotes the production of oxytocin, the hormone of love, in you and your baby, and oxytocin plays a key role in the supply of the first breast milk - colostrum. 3
“As soon as the obstetricians were convinced that our son was healthy, the three of us — me, my husband and our baby — were left to give us the opportunity to get to know each other. It was a very special hour - an hour of awkwardness, turbulent emotions and bliss. During this time, I breastfed my son twice, ”recalls Ellie, a mother of two from the UK.
Did you know that breastfeeding helps to recover after childbirth? This is because oxytocin stimulates uterine contractions. In the first hours after childbirth, this contributes to the natural release of the placenta and reduces blood loss. 4
In the first hours after childbirth, this contributes to the natural release of the placenta and reduces blood loss. 4
What if the birth did not go according to plan?
If you had a caesarean section or other complications during childbirth,
You can still establish skin-to-skin contact with your baby and breastfeed him in the first hours after birth.
“If you can't hold your baby, have your partner do it for you and make skin-to-skin contact with the baby. This will give the baby a sense of security, care and warmth so that he can hold on until you recover, ”Katie advises.
If the baby is unable to breastfeed, it is advisable to start expressing milk as early as possible and do so as often as possible until the baby is able to feed on its own. “While breastfeeding in the first hours after birth lays an excellent foundation for the future, it is not so important,” Cathy reassures. “It is much more important to start lactation so that in the future, if necessary, you can start breastfeeding.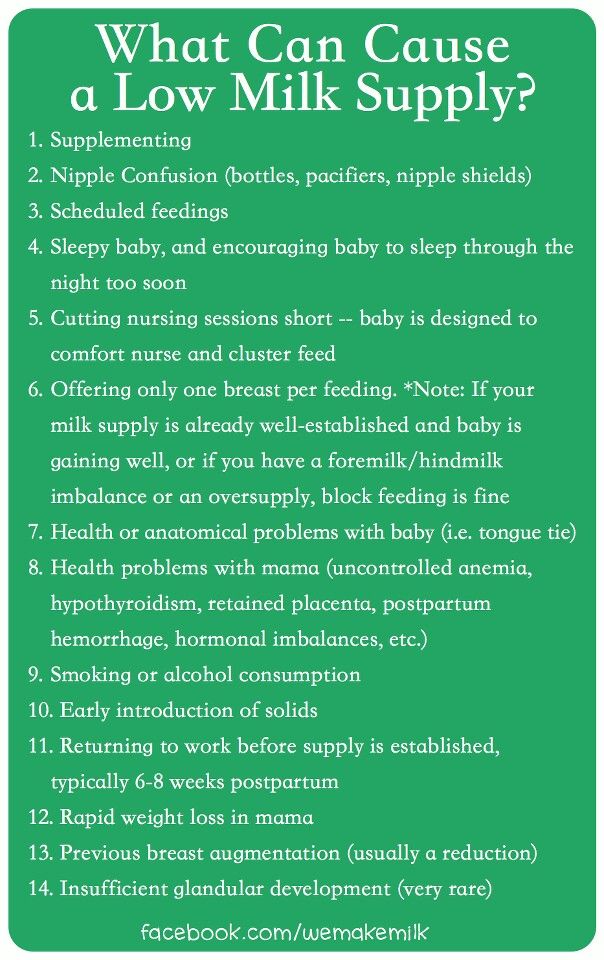 ”
”
To start milk production, you can express milk manually or use a breast pump that can be given to you at the hospital. 5 And it will be possible to feed a child with expressed precious colostrum. This is especially important if the baby was born premature or weak, since breast milk is extremely healthy.
If a baby was born prematurely or has a medical condition and cannot be breastfed immediately, this is no reason not to continue breastfeeding. “I have worked with many new mothers who were unable to breastfeed their baby for the first six weeks due to preterm labor or other reasons. Nevertheless, all of them later successfully switched to breastfeeding,” says Kathy.
Does the baby latch on correctly?
Correct breastfeeding is essential for successful breastfeeding 6 , as it determines how effectively the baby will suckle milk and hence grow and develop. Latching on the breast incorrectly can cause sore or damaged nipples, so don't hesitate to ask your doctor to check that your baby is properly attached to the breast, even if you are told that everything is fine and you do not see obvious problems - especially while you are in the hospital.
“While I was in the hospital, I called the doctor at every feed and asked me to check if I was breastfeeding correctly,” says Emma, mother of two from Australia. - There were several cases when it seemed to me that everything seemed to be right, but it was painful to feed, and the doctor helped me take the baby off the breast and attach it correctly. By the time I was discharged, I had already learned to do it confidently.”
When applying to the breast, point the nipple towards the palate. This will allow the baby to take the nipple and part of the areola under it into their mouth. It will be easier for him to suck if he has both the nipple and part of the areola around in his mouth. 6
“When a baby latch on properly, it doesn't cause discomfort and it causes a pulling sensation, not pain,” Cathy explains. - The baby's mouth is wide open, the lower lip may be slightly turned outward, and the upper one lies comfortably on the chest. The body language of the child indicates that he is comfortable. There isn't much milk at this early stage, so you probably won't notice your baby swallowing, but he will suckle a lot and nurse frequently."
There isn't much milk at this early stage, so you probably won't notice your baby swallowing, but he will suckle a lot and nurse frequently."
How often should a newborn be fed?
The frequency and duration of breastfeeding in the first week can vary greatly. “The first 24 hours of life are completely different for different children. Someone sleeps a lot (after all, childbirth is tiring!), And someone often eats, says Katie. - Such a variety greatly confuses young mothers. Everyone gives different advice, so it's important to remember that every mother and child is different."
“Colostrum is thicker than mature breast milk and is produced in smaller amounts, but has many benefits. When the baby eats colostrum, he learns to suck, swallow and breathe until milk begins to flow in more volume, ”explains Cathy.
Milk usually arrives on the second or fourth day after birth. Until this time, the baby is applied to the breast 8-12 times a day (and sometimes more often!), including at night. 7 Feeding may last 10-15 minutes at this stage, or 45 minutes or even an hour, as the baby is just beginning to develop the muscles and coordination for effective suckling.
7 Feeding may last 10-15 minutes at this stage, or 45 minutes or even an hour, as the baby is just beginning to develop the muscles and coordination for effective suckling.
“At first, the intensity of feeding is very high, often higher than many people realize, and this is shocking to most new mothers,” says Cathy. - Sometimes mom has no time to go to the toilet, take a shower and have a snack. It usually comes as a surprise."
Camille, a mother from Australia, experienced this. “The first week, Frankie ate every two hours, day and night, and each time it took half an hour to an hour to feed,” she recalls. “My husband and I were completely exhausted!”
Do I need to feed my newborn on a schedule?
The good news is that frequent feeding promotes lactation and stimulates milk production. 7 The more your baby eats, the more milk you will have. Therefore, forget about feeding your newborn on a schedule - this way he will have less chance of feeding. Try to feed your baby when he signals that he is hungry 8 :
Try to feed your baby when he signals that he is hungry 8 :
- tossing and turning in her sleep;
- opens eyes;
- turns his head if he feels a touch on his cheek;
- sticks out tongue;
- groans;
- licks lips;
- sucks fingers;
- is naughty;
- whimpers;
- is crying.
Crying is the last sign of hunger, so when in doubt, just offer your baby the breast. If he bursts into tears, it will be more difficult to feed him, especially at first, when both of you are just learning how to do it. As your baby grows, he will likely eat less frequently and take less time to feed, so breastfeeding will seem more predictable.
Does breastfeeding hurt?
You may have heard that breastfeeding is not painful at all, but in fact, in the early days, many new mothers experience discomfort. And this is not at all surprising, given that the nipples are not used to such frequent and strong sucking.
“Breastfeeding can be uncomfortable for the first couple of days – your body and your baby are just getting used to it. If a baby eats for too long and does not latch well, the sensations are almost the same as from unworn new shoes, Cathy compares. Just as tight shoes can rub your feet, improper suckling can damage your nipples. Prevention is always better than cure, so if the pain persists after a few days of feeding, contact a lactation consultant or healthcare professional.”
Maria, a mother from Canada, agrees: “Although my son seemed to latch onto the breast well, he damaged his nipples while feeding, and I was in pain. As it turned out, the reason was a shortened frenulum of the tongue. The breastfeeding specialists at our city clinic have been of great help in diagnosis and treatment.”
In addition, you may experience period cramps during the first few days after breastfeeding, especially if this is not your first baby. This is the so-called postpartum pain. The fact is that oxytocin, which is released during breastfeeding, contributes to further contraction of the uterus to restore its normal size. 4
The fact is that oxytocin, which is released during breastfeeding, contributes to further contraction of the uterus to restore its normal size. 4
When milk arrives, the breasts usually become fuller, firmer and larger than before delivery. In some women, the breasts swell, harden and become very sensitive - swelling of the mammary glands occurs. 10 Frequent breastfeeding relieves these symptoms. For more breast care tips, read our article What is Breast Swelling?
How often does a newborn urinate and defecate?
What goes into the body must go back out. Colostrum
has a laxative effect, helping to eliminate meconium - the original feces. It looks a little scary - black and sticky, like tar. 11 But don't worry, it won't always be like this. Breastfed babies usually have a slightly sweet smell of stool.
How many times a day you will need to change diapers and how the contents should look like, see below.
Day one
- Frequency: once or more.

- Colour: greenish black.
- Texture: sticky like tar.
Second day
- Frequency: twice or more.
- Colour: dark greenish brown.
- Texture: less sticky.
Day three
- Frequency: twice or more.
- Colour: greenish brown to brownish yellow.
- Texture: non-sticky.
Fourth day and then the entire first month
- Frequency: twice or more.
- Color: yellow (feces should turn yellow no later than by the end of the fourth day).
- Texture: grainy (like mustard with grains interspersed). Leaky and watery.
The baby's urine should be light yellow. On average, babies urinate once a day for the first two days. Starting around the third day, the number of wet diapers increases to three, and from the fifth day onwards, diapers have to be changed five times a day or more often. In addition, during the first few days, the weight of wet diapers increases. 11
11
Is the baby getting enough breast milk?
Since very little milk is produced at first,
you may feel that your baby is not getting enough milk. But if you feed your baby on demand, you will produce exactly as much milk as he needs. If you want to keep the process under control, be guided by the frequency of diaper changes above. If your baby soils less diapers, check with your doctor.
“For the first three or four weeks, most babies just eat and sleep. If the child is worried and constantly asks for a breast, you should consult with your doctor, ”Katie recommends.
Sometimes the baby may vomit after feeding. If the vomit is the color of milk, this is not a cause for concern. But if there are orange, red, green, brown or black blotches in it, or the child vomits with a "fountain", consult a doctor. You should also consult a doctor if the baby has a high temperature, the fontanel (soft spot on the head) has sunk, blood is found in the stool, and also if the weight recorded at birth has not recovered within two weeks. 11
11
But if there are no frightening symptoms and the baby is growing at a normal pace, then he has enough milk. Soon you will both get used to breastfeeding and establish a more stable routine.
For the next step in breastfeeding, see Breastfeeding the First Month: What to Expect.
Literature
1 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
2 Shashi R et al. Postpartum psychiatric disorders: Early diagnosis and management. Indian J Psychiatry . 2015; 57( Suppl 2): S 216– S 221. - Shashi R. et al., Postnatal mental disorders: early diagnosis and treatment. Indian J Saikiatri. 2015; 57(App 2):S216-S221.
- Shashi R. et al., Postnatal mental disorders: early diagnosis and treatment. Indian J Saikiatri. 2015; 57(App 2):S216-S221.
3 Moberg KU, Prime DK. Oxytocin effects in mothers and infants during breastfeeding. Infant . 2013;9(6):201-206. - Moberg K, Prime DK, "The effects of oxytocin on mother and child during breastfeeding." Infant. 2013;9(6):201-206.
4 Sobhy SI, Mohame NA. The effect of early initiation of breast feeding on the amount of vaginal blood loss during the fourth stage of labor. J Egypt Public Health Assoc . 2004;79(1-2):1-12. - Sobhi SI, Moham NA, "Early initiation of breastfeeding and its effect on vaginal bleeding in the fourth stage of labor." G Egypt Public Health Assoc. 2004;79(1-2):1-2.
5 Meier PP et al. Which breast pump for which mother: an evidence-based approach to individualizing breast pump technology. J Perinatol . 2016;36(7):493. - Meyer P.P. et al., Breastpump Selection: A Scientific Approach to Customizing Pumping Technology. J Perinatol (Journal of Perinatology). 2016;36(7):493-499.
J Perinatol . 2016;36(7):493. - Meyer P.P. et al., Breastpump Selection: A Scientific Approach to Customizing Pumping Technology. J Perinatol (Journal of Perinatology). 2016;36(7):493-499.
6 Cadwell K. Latching - On and Suckling of the Healthy Term Neonate: Breastfeeding Assessment. J Midwifery & Women ’ s Health . 2007;52(6):638-642. — Cadwell, K., "Latching and sucking in healthy newborns: evaluation of breastfeeding." F Midwifery Women Health. 2007;52(6):638-642.
7 Kent JC et al. Principles for maintaining or increasing breast milk production. J Obstet , Gynecol , & Neonatal Nurs . 2012;41(1):114-121. - Kent J.S. et al., "Principles for Maintaining and Increasing Milk Production". J Obstet Ginecol Neoneutal Nurs. 2012;41(1):114-121.
J Obstet Ginecol Neoneutal Nurs. 2012;41(1):114-121.
8 Australian Breastfeeding Association [ Internet ]. Feeding cues ; 2017 Sep [ cited 2018 Feb ]. - Australian Breastfeeding Association [Internet], Feed Ready Signals; September 2017 [cited February 2018]
9 Jacobs A et al. S3-guidelines for the treatment of inflammatory breast disease during the lactation period. Geburtshilfe Frauenheilkd . 2013;73(12):1202-1208. - Jacobs, A. et al., Guidelines S -3 for the management of inflammatory breast disease during breastfeeding. Geburtskhilfe und Frauenheilkünde. 2013;73(12):1202-1208.
10 Lawrence RA, Lawrence RM. Breastfeeding: A guide for the medical profession.