Baby cried immediately after feeding
Baby Cries After Feeding: What Should I Do?
Medically reviewed by Karen Gill, M.D. — By Chaunie Brusie on October 3, 2018
My daughter, the “crier”
My second daughter was what my oldest fondly referred to as a “crier.” Or, in other words, she cried. A lot. The crying with my baby girl seemed to intensify after every single feeding and particularly at night.
It was those hellish hours between darkness and dawn when my husband and I would take turns walking around the house with her in our arms, praying and, mostly in my case, sobbing because we couldn’t console our baby.
I didn’t know it then in my sleep-deprived state, but my daughter’s crying after feedings wasn’t that uncommon. In combination with her frequent spitting up, it was pretty much a classic textbook case of colic.
Colic
Colic, in technical terms, simply means a “crying, fussy baby that doctors can’t figure out.”
OK, so that’s not really the definition, but in essence, that’s what it boils down to. The British Medical Journal (BMJ) lists one criterion for colic: A baby that cries for at least three hours a day, three or more days a week, and is under 3 months old. Check, check, and check.
There isn’t one single known cause of colic. Even the actual clinical incidence of colic, estimated by BMJ to be around 20 percent of all babies, can be tricky.
Acid reflux
One of those causes of crying after feeding and spitting up in babies is actually acid reflux. This condition is known as gastroesophageal reflux disease (GERD) if it also causes significant symptoms such as poor weight gain.
When my “crier” daughter was 5, she frequently complained of her stomach hurting and as a result, had to undergo a series of testing with a gastroenterologist, a doctor that specializes in the GI system.
At our first appointment, the very first question he asked me was if she had colic as a baby and if she spit up a lot, to both of which I practically shouted, “Yes! How did you know?!”
He explained that acid reflux or GERD can manifest as symptoms similar to colic in babies, stomach pain in school-aged children, and later as actual heartburn pain in adolescents.
While many infants spit up, fewer have actual GERD, which can be caused by an underdeveloped flap between the esophagus and stomach or a higher-than-normal production of stomach acid.
In most cases, a diagnosis of infant reflux is simply based on your baby’s symptoms. If your doctor suspects a severe case however, there are several different tests that actually diagnose infant reflux.
Testing can involve taking a biopsy of your baby’s intestine or using a special type of X-ray to visualize any affected areas of obstruction.
Food sensitivities and allergies
Some babies, especially breastfed babies, may be allergic to certain food particles that their mothers are eating.
The Academy of Breastfeeding Medicine notes that the most common offender is cow’s milk protein in the mother’s milk, but even a true allergy is very rare. Only about 0.5 to 1 percent of exclusively breastfed babies are thought to be allergic to cow’s milk protein.
The other most common culprits, according to the ABM, are egg, corn, and soy, in that order.
If your baby is displaying symptoms of extreme irritability after feedings and has other symptoms, such as bloody stools (poop), you should speak with your healthcare provider about getting them tested for allergies.
Aside from a true allergy, there’s also been some evidence that following a low allergen diet while breastfeeding (essentially avoiding those top allergy foods, such as dairy, eggs, and corn) may be beneficial for infants with colic.
Strict elimination diets can have their own risks, so speak with your doctor before significantly changing your diet.
In our situation, I found that dairy, caffeine, and certain seeded fruit exacerbated my daughter’s crying and spitting up. By eliminating those foods and substances from my diet, I was able to help lessen her discomfort.
If you have a baby with colic, you might want to try anything at all to help ease your baby’s crying. If you’re curious to see if your diet has any effect, you can start by logging your food in a food journal and writing down your baby’s reactions after each meal.
Next, you can eliminate one food at a time and see if reducing your intake of certain foods seems to make a difference in your baby’s behavior. If you hit on one you feel helps your baby to cry less, this does not mean they will not be able to eat that food in the future.
Just be sure to keep in mind that a true allergy is rare. Also, be sure to monitor for any additional symptoms, such as blood in your baby’s poop.
Gas
If your baby is crying a lot after every feeding, it may simply be a buildup of air swallowed while eating. It’s thought that bottle-fed babes in particular may be more prone to swallowing a lot of air during a feeding. This can trap gas in their stomachs and be uncomfortable.
In general, breastfed babies swallow less air while eating simply due to the way they eat. But every baby is different and even breastfed babies may need to be burped after a feeding.
Trying keeping your baby upright after a feeding and burping gently from the bottom of their back and up through the shoulders to work the gas bubbles up and out. Also check out this illustrated guide to burping a sleeping baby.
Also check out this illustrated guide to burping a sleeping baby.
Formula
If your baby is formula-fed, swapping out the formula you use may be a simple solution to a crying baby after feedings. Every formula is a little bit different and certain brands make formulas for more sensitive baby tummies.
If you decide to try this, talk to your baby’s pediatrician about whether an elemental formula would be a good choice to try for a week. If you try one different brand and you see no change in your baby’s fussiness, continuing to try different brands is unlikely to help.
Takeaway
Colic, along with a few other common conditions, might be the culprit if you too have a “crier” on your hands.
If your baby doesn’t find relief after dietary changes or additional burping, then make an appointment to see their doctor.
Share on Pinterest
Chaunie Brusie, BSN, is a registered nurse with experience in labor and delivery, critical care, and long-term care nursing. She lives in Michigan with her husband and four young children, and is the author of the book “Tiny Blue Lines.”
She lives in Michigan with her husband and four young children, and is the author of the book “Tiny Blue Lines.”
Last medically reviewed on October 3, 2018
- Parenthood
- Baby
- 06 Months
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- ABM clinical protocol #24: Allergic proctocolitis in the exclusively breastfed infant. (2011). DOI:
10.1089/bfm.2011.9977 - Harrel MC, et al. (2015). Is there a correlation between maternal diet in breastfeeding mothers and infantile colic? DOI:
10.1097/01.EBP.0000541032.94135.ca - Mayo Clinic Staff. (2018). Infant reflux.
mayoclinic. org/diseases-conditions/infant-acid-reflux/diagnosis-treatment/drc-20351412
org/diseases-conditions/infant-acid-reflux/diagnosis-treatment/drc-20351412 - Rosen LD, et al. (2007). Complementary, holistic, and integrative medicine.
pedsinreview.aappublications.org/content/28/10/381 - Saavedra MA, et al. (2003). Infantile colic incidence and associated risk factors: A cohort study. .
ncbi.nlm.nih.gov/pubmed/14502331 - Sung V, et al. (2014). Treating infant colic with the probiotic Lactobacillus reuteri: Double blind, placebo controlled randomised trial. DOI:
10.1136/bmj.g2107 - Symptoms & causes of GER and GERD in infants. (2015).
niddk.nih.gov/health-information/digestive-diseases/acid-reflux-ger-gerd-infants/symptoms-causes
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Current Version
Oct 3, 2018
Written By
Chaunie Brusie
Edited By
Nizam Khan (TechSpace)
Medically Reviewed By
Karen Richardson Gill, MD
Share this article
Baby Crying After Feeding: What Should You Do?
Did you imagine watching your new bundle of joy gently slip off to sleep in your arms while eating? Is your reality a screaming baby who can’t seem to get comfortable after feedings?
You’re not alone; it happens more frequently than you think. As moms, we’ve dealt with this ourselves. And as medical practitioners, we’ve seen plenty of parents with the same issue.
As moms, we’ve dealt with this ourselves. And as medical practitioners, we’ve seen plenty of parents with the same issue.
There are several reasons your baby might be feeling discomfort after feeding. We’ll look at some of the main causes of why your baby cries after feeding, and we’ll share some proven techniques you can use to make your baby more comfortable and your evenings calmer.
Key Takeaways
- Babies may cry after feeding due to colic, acid reflux, gas, or food sensitivities.
- Colic involves excessive crying, with many infants outgrowing it by 3-9 months.
- Acid reflux, or GERD, affects up to 50% of babies, but most outgrow it by their first birthday.
- Reduce gas by burping your baby, feeding in an upright position, and adjusting your diet or bottle feeding techniques.
Why Do Babies Cry After Feeding?
If you’re dealing with an inconsolable child after feedings, you may have noticed some of the following symptoms of abdominal discomfort:
- Crying: Babies seem to experience more discomfort during the evening hours.
 If you’ve heard the cry before, you know it’s unmistakably a cry of pain. An urgency and intensity suggest it’s more than just complaining.
If you’ve heard the cry before, you know it’s unmistakably a cry of pain. An urgency and intensity suggest it’s more than just complaining. - Pulling up or extending their legs: Is your baby bringing their knees up to their chest or rigidly extending their legs? They are likely experiencing abdominal pain.
- Distended bellies: Most post-feeding discomfort can be linked to excessive gas in the baby’s system. If it’s trapped in their digestive system, it may lead to a hardened or swollen tummy. Their crying may be exacerbating the discomfort they’re already experiencing.
There are many possible causes of your baby’s discomfort. While this is not an exhaustive list, we’ll talk about some of the main sources of digestive discomfort in young babies.
1. Colic
Perhaps you’ve heard a baby referred to as colicky. Your pediatrician may have even given you the diagnosis. This designation came about after a pediatrician’s study on extremely fussy children and has been around for decades.
Having a colicky baby basically means you have a baby who cries — a lot. You can expect a baby with colic to cry at least three hours a day for at least three days a week (1). Using this definition, nearly a quarter of all infants will experience colic.
The good news is that 50% of babies with colic outgrow the condition by the time they’re three months old. By the time your baby reaches nine months old, there’s a 90% chance they’ll have outgrown the colic.
There’s usually no discernible cause for colic. But it’s clear your baby is uncomfortable. This discomfort is typically linked to the digestive system and follows feedings.
You may need to hold your colicky baby more often and provide lots of comfort. While it can be nerve-wracking and frustrating, having a colicky baby doesn’t mean your baby is unhealthy.
2.
 Acid Reflux
Acid RefluxAlso known as gastroesophageal reflux disease (GERD), acid reflux is a common cause of post-feeding discomfort. It can be upsetting to hear your baby is experiencing reflux. But reflux isn’t uncommon; it affects up to 50% of babies during the first few months of life.
If your child is suffering from GERD, there may be additional accompanying symptoms, like difficulty gaining or maintaining weight. Children with GERD frequently spit up and may even experience aggressive vomiting (2).
When your child is experiencing acid reflux, it’s usually because the gastrointestinal system is not working properly. If the difficulty your baby is experiencing is related to an immature digestive system, a child may outgrow GERD. When this happens — as it does for about 95% of children — it usually does so by their first birthday.
There’s also a remote possibility your baby will not outgrow GERD. If this is the case, your doctor can help you create an ongoing treatment plan to support your child’s needs. If you suspect your child has GERD, you should make an appointment with a pediatric gastroenterologist to discuss your concerns.
If you suspect your child has GERD, you should make an appointment with a pediatric gastroenterologist to discuss your concerns.
3. Gas
Another common reason babies cry after feeding has to do with gas. Babies’ bodies are still developing their basic skills. A baby who swallows too much air during feedings may not be able to process the extra gas easily.
This leads to pressure and distension and can cause crying and extreme discomfort after meals. It may not be possible to keep your baby from taking in too much air during feedings. However, there are some things you can do to keep air intake to a minimum:
- Frequently burp your baby: Burping can help remove some of the excess air from your baby’s system and leave them feeling more comfortable. To successfully burp your baby, hold them upright, supporting their head well, and pat or rub their back.
 Some babies seem to burp a lot, while others might have one good burp per feeding.
Some babies seem to burp a lot, while others might have one good burp per feeding. - Feed in a more upright position: Keep your baby upright for at least 20 to 30 minutes after meals to reduce gas discomfort. If your little one is uncomfortable during sleep, you can also try an inclined mattress, following safe sleep guidelines (3).
- Cycle your baby’s legs: If your baby is visibly uncomfortable, you can lie them on their back and cycle their legs as though they’re riding a bike. This can help push the air through their system and provide them with some relief.
- Try to catch the crying early: It can be tempting to let your baby work through the crying and get to sleep. If it’s likely your child won’t stop, intercept the crying as soon as possible. Crying usually involves gulping air, which will lead to more gas — and more crying.
- Don’t put your baby to sleep directly after a large meal: We all know it’s best for your baby to sleep on their back.
 But putting a baby down on their back with a full stomach can be a recipe for discomfort. Hold your little one for 20 minutes post-feeding, even if they’re already asleep.
But putting a baby down on their back with a full stomach can be a recipe for discomfort. Hold your little one for 20 minutes post-feeding, even if they’re already asleep.
These approaches are great whether you’re nursing or formula feeding. However, there are some specific things you’ll want to look out for, depending on how you feed.
Nursing
- Pay attention to how you eat: What you eat directly impacts your breast milk. Certain foods, including broccoli, beans, and onions, are notoriously difficult for your baby to break down. If you notice gas is especially bad for your baby after you eat a particular type of food, you can limit it in your diet.
- Food sensitivity: Something in your diet may be making your baby fussy. The most common culprits are dairy and caffeine. Usually, there are additional symptoms. Keeping a food journal may help you pinpoint the offending item so you can eliminate it from your diet.
- Nurse your baby in positions that keep their head above their stomach: This will help limit the amount of air intake and encourage digestion.
- Get rid of the excess gas: Plan on burping your baby before switching sides and after feeding.
Bottle Feeding
- Pay attention to the bottle nipple you’re using: If your bottle nipple releases fluid more quickly than your baby can comfortably eat, they will guzzle their meal. This leads to an increase in air intake and plenty of gas. Using a slow-flow nipple can help avoid this problem.
- Position your bottle properly: Make sure your bottle is tilted enough to allow the milk to cover the nipple completely. This will help prevent your baby from sucking in the air that’s in the bottle along with their meal.
- Force out the extra air: Expect to burp your baby after every ounce of milk or formula is consumed.
Gas can be highly uncomfortable for your little one. Following these tips will help you mitigate gas and discomfort for your baby.
4. Food Sensitivities
It’s possible that some of your child’s crying after eating is related to an intolerance or allergy.
Everything you consume is passed on to your child in your milk. Some foods — like dairy and eggs — are frequently associated with food sensitivities (4).
If you’re nursing, the best way to determine what’s agitating your child is by charting your food intake. Keep a food journal; you may be surprised at where correlations begin to appear.
Early on, my youngest was inconsolable after the last meal of the day — just when the time came to settle into sleep.
The common link to the discomfort? Spicy food and cheese during my dinner. I cut back on those, and my baby was happier for it.
We were fortunate our baby was only intolerant of these foods and didn’t have a true allergy. Sometimes a young system has difficulty handling certain foods.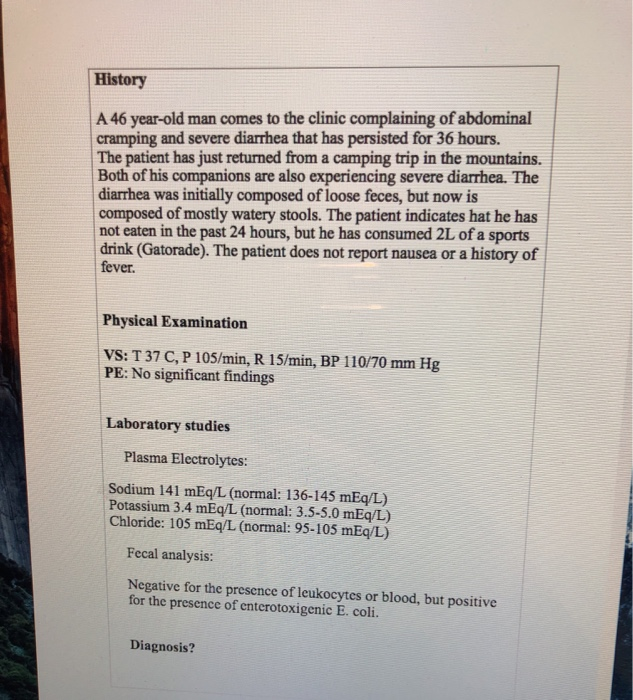 If your child has a true allergy, you’ll notice more symptoms than abdominal distress.
If your child has a true allergy, you’ll notice more symptoms than abdominal distress.
Be on the lookout for hives, skin rashes, vomiting, diarrhea, difficulty breathing, and any face or tongue swelling (5). If you suspect your child has an allergy, you should consult your pediatrician immediately. And if your little one is struggling with breathing after eating, call 911.
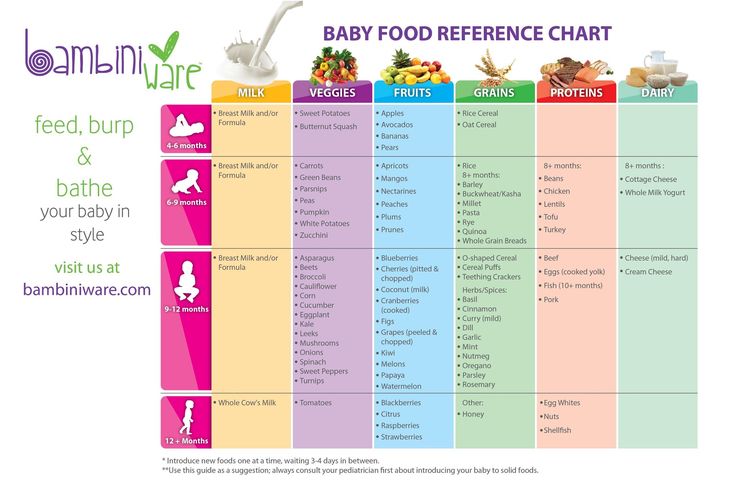
When starting solids, always introduce one new food at a time to your little one to determine what might have caused the response.
Formula feeding your baby? If you notice signs of a food allergy before introducing solid foods, your baby may be allergic to the formula (most commonly the cow’s milk protein). If you think this might be the case, work closely with your pediatrician to determine a suitable alternative formula.
Other Reasons For Crying After Eating
Many causes of post-feeding crying come back to the digestive process. They aren’t the only reasons, though. Some other things may cause your baby to cry.
They aren’t the only reasons, though. Some other things may cause your baby to cry.
5. Teething
Most babies will begin teething between 4 and 6 months of age. This doesn’t guarantee the teeth will show up shortly afterward, though. Some babies could go through several months of teething before the teeth break through the gums.
Unfortunately, your child will likely experience inflammation and extreme discomfort in the mouth and gums during this time. This can make even usually benign experiences, like nursing or bottle-feeding, incredibly painful.
If your baby is experiencing teething-related pain, you can help by numbing their gums with cool water before feeding. Just dip your thumb in water and rub directly onto the gums (6). Or let them chew on a washcloth that has been wet and then slightly frozen.
Other pain management approaches can include numbing oral medications and anti-inflammatories (though you’ll want to ask your baby’s doctor before using these). You’ll also want to provide plenty of opportunities for your baby to practice gnawing on things. This can help relieve the pressure, encouraging teeth to break through a little more quickly.
You’ll also want to provide plenty of opportunities for your baby to practice gnawing on things. This can help relieve the pressure, encouraging teeth to break through a little more quickly.
6. Thrush
Babies can experience an overgrowth of yeast in their mouths (7). While Candida, a parasitic fungus, is normally present in your body and in your baby’s mouth, excess yeast can be a problem. It’s extremely uncomfortable and may impact your baby’s ability to eat properly.
Excess amounts of yeast frequently happen after a course of antibiotics. Antibiotics will kill off the bad bacteria, but they don’t discriminate. This means they may also kill off good bacteria, leaving an imbalance that can lead to thrush.
Thrush is usually a visible condition. If you suspect your baby has thrush, look inside their mouth. If thrush is present, you’ll see filmy white patches that may look like milk. If the patch doesn’t come away with a swipe from your finger, you’re looking at thrush.
If your baby has thrush, make an appointment with your pediatrician. A simple course of prescription antifungal medication will help clean up the condition.
Yeast is quite persistent. If you’re dealing with thrush, plan on sterilizing every plastic nipple or pacifier you own to prevent recontamination. Nursing? You’ll need to be treated for thrush as well — or you will simply pass the infection back and forth between you and your baby.
Feedback: Was This Article Helpful?
Thank You For Your Feedback!
Thank You For Your Feedback!
What Did You Like?
What Went Wrong?
Why does the baby cry - articles from the specialists of the clinic "Mother and Child"
Bondarenko Margarita Gennadievna
Otorhinolaryngologist (ENT)
Clinic "Mother and Child" Kuntsevo,
I want to eat!
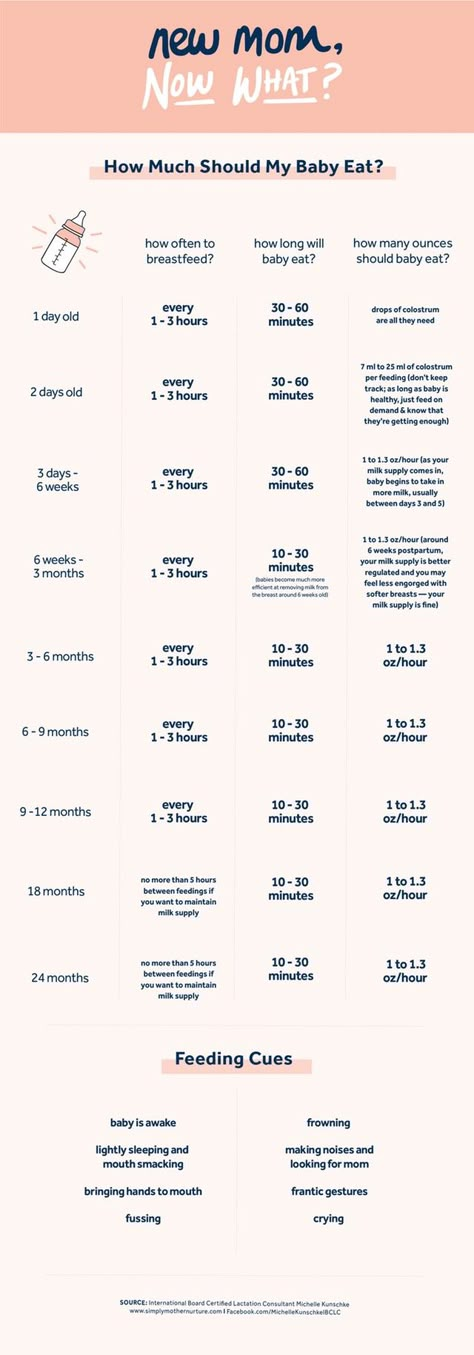
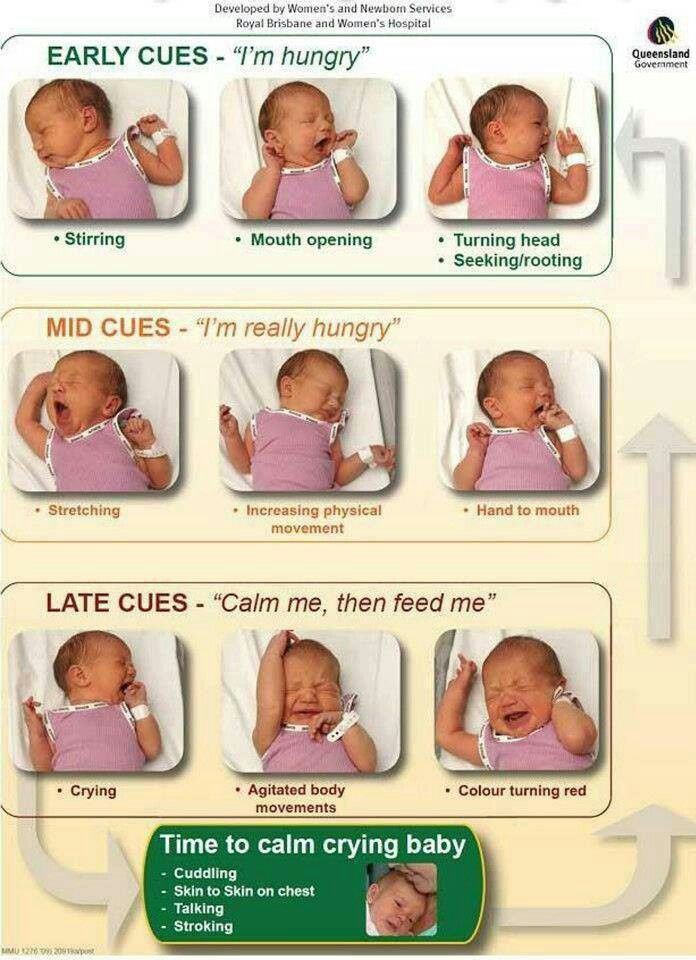
Most often the baby cries because he wants to eat. And to understand that he is hungry is the easiest way. At first, the baby shows concern, smacks his lips, turns his head to his mother's hand, stroking his cheek, tries to put his own fist in his mouth. All this means that there is very little time left before the hungry cry. Noticing such signs, you should not wait: feed the baby on demand. Otherwise, starting to cry, he will have to spend a lot of energy trying to calm down, and therefore, he will eat less and the next time he will get hungry again too soon. In general, for children who are breastfed, during the first month of life there is no clear feeding regimen. A newborn can be applied to the breast up to 10-12 times a day.
At first, the baby shows concern, smacks his lips, turns his head to his mother's hand, stroking his cheek, tries to put his own fist in his mouth. All this means that there is very little time left before the hungry cry. Noticing such signs, you should not wait: feed the baby on demand. Otherwise, starting to cry, he will have to spend a lot of energy trying to calm down, and therefore, he will eat less and the next time he will get hungry again too soon. In general, for children who are breastfed, during the first month of life there is no clear feeding regimen. A newborn can be applied to the breast up to 10-12 times a day.
I want to sleep!
The next reason for screaming is, oddly enough, the desire to sleep. Many parents think that a baby can fall asleep anytime, anywhere, and even in almost any position. No, it's not like that - he needs help. How do you know if your baby wants to sleep? It's easy to guess. At first, he will behave restlessly, cry, push out the pacifier, rub his eyes, yawn. And then he starts crying. Here, too, it is necessary to try to calm the child as quickly as possible so that he does not disperse in crying, otherwise it will be more difficult for him to fall asleep. Rituals will help: you can shake the baby, sing a song, put it in the usual sleeping place.
And then he starts crying. Here, too, it is necessary to try to calm the child as quickly as possible so that he does not disperse in crying, otherwise it will be more difficult for him to fall asleep. Rituals will help: you can shake the baby, sing a song, put it in the usual sleeping place.
I'm wet!
Crying can be a signal that the baby is uncomfortable, such as a wet diaper. Cold and wet, they irritate the skin, so he screams: “Mom, dad, change me quickly!” Crying about this is whimpering, incessant, although it sounds either stronger or weaker, it may be accompanied by hiccups, as the child freezes in wet diapers. If the diaper is changed, and the baby is warmer to cover, he will calm down. If the child is not in diapers, but in reusable diapers, you should not relax either: they can leak or get wet inside. So, the baby is also wet and cold. If the child sleeps in one diaper all night, then he may be disturbed by a greatly increased diaper volume. And of course, children do not like to be in dirty diapers (diapers): feces quickly irritate delicate skin.
I'm hot!
If the baby is hot, he will also cry about it. He will begin to whimper, scatter his arms and legs, his skin will turn red, a small red rash (prickly heat) may appear under his clothes. At the same time, the temperature of the baby sometimes even rises to 37.5 ° C. This is what saves here: the child must be undressed (and removed diapers, especially disposable ones), wiped with a towel moistened with water at room temperature, and allowed to lie in the air for several minutes. Then you need to dress the baby, but in other, clean clothes. In the fight against overheating and prickly heat, a reasonable amount of clothing and a comfortable room temperature - no higher than 24-25 ° C will help, first of all.
I'm uncomfortable!
The reason for the inconvenience can be any: the child may scream when the temperature changes, when changing clothes, changing the diaper or wiping his bottom with a damp cloth. Newborns feel more comfortable when they are dressed or wrapped in diapers, because the touch of air on the skin is not always pleasant for them. In addition, children often do not like to be changed, especially if it is winter and you have to wear a lot of clothes. There is only one way out: learn to act as quickly as possible, causing the crumbs a minimum of inconvenience.
In addition, children often do not like to be changed, especially if it is winter and you have to wear a lot of clothes. There is only one way out: learn to act as quickly as possible, causing the crumbs a minimum of inconvenience.
A few words about clothes. It is better not to buy clothes with fasteners on the back and coarse seams inside - the baby may not like it. And sometimes even the slightest thread or hair caught between the clothes and the skin of the baby causes him great inconvenience.
I want attention!
Attention and tactile sensations are very important for a child. He loves to see the faces of his mom and dad, hear their voices, communicate with them. But so far, the baby cannot ask his parents to take him in his arms, read him a fairy tale, sing a song, play - but this does not mean at all that he does not need it. Therefore, crying, the baby wants to be paid attention to, requires communication. Do not worry that the baby will get used to the hands too much. While he is so small, he needs to feel a sense of security - it is this that will later help him gain confidence in his abilities. Well, different cradles, deck chairs, playpens, child seats will only help mom and dad free their hands and at the same time place their beloved child next to them.
While he is so small, he needs to feel a sense of security - it is this that will later help him gain confidence in his abilities. Well, different cradles, deck chairs, playpens, child seats will only help mom and dad free their hands and at the same time place their beloved child next to them.
Once you learn to understand your baby's “language”, you will see that the reasons for crying vary from case to case. A little time and patience - and very soon you will understand what the child wants, already from the first seconds of his discontent.
Make an appointment
to the doctor - Bondarenko Margarita Gennadievna
Clinic "Mother and Child" Kuntsevo
Pediatric otorhinolaryngologyFor childrenDispanserizationMonitoring of children at home0003
By clicking on the send button, I consent to the processing of personal data
Attention! Prices for services in different clinics may vary. To clarify the current cost, select the clinic
The administration of the clinic takes all measures to update the prices for programs in a timely manner, however, in order to avoid possible misunderstandings, we recommend that you check the cost of services by phone / with the managers of the clinic
Clinical Hospital MD GROUPClinical Hospital Lapino-1 "Mother and Child"Children's Clinic KG "Lapino" on New Riga (branch)Clinic "Mother and Child" KuntsevoClinic "Mother and Child" SavelovskayaClinic "Mother and Child" South-WestClinic "Mother and child "Novogireevo
All directionsKinesiotherapy for childrenSpecialist consultations (adults)Specialist consultations (children)Massage / manual therapy for childrenTherapeutic research
Massage therapy for children0003 05.
Therapeutic research
Nothing found
The administration of the clinic takes all measures to update the price list posted on the website in a timely manner, however, in order to avoid possible misunderstandings, we advise you to clarify the cost of services and the timing of tests by calling
Baby in the maternity hospital: the first days of life
Immediately after childbirth
As soon as the baby born, the midwife takes him in her arms and immediately begins to care for him. And there are no trifles here. Imagine: a baby is born wet, he has just been in his mother's body, where the temperature was 36.6 ° C, now he enters the maternity block, where the air temperature is about 24 ° C. This is a warm and comfortable environment for you and me, and for a baby, the difference of these 12 ° C is quite large. Thermoregulation in young children is still imperfect, they do not retain heat well and quickly cool down, and then there is also moist skin and a sharp temperature drop.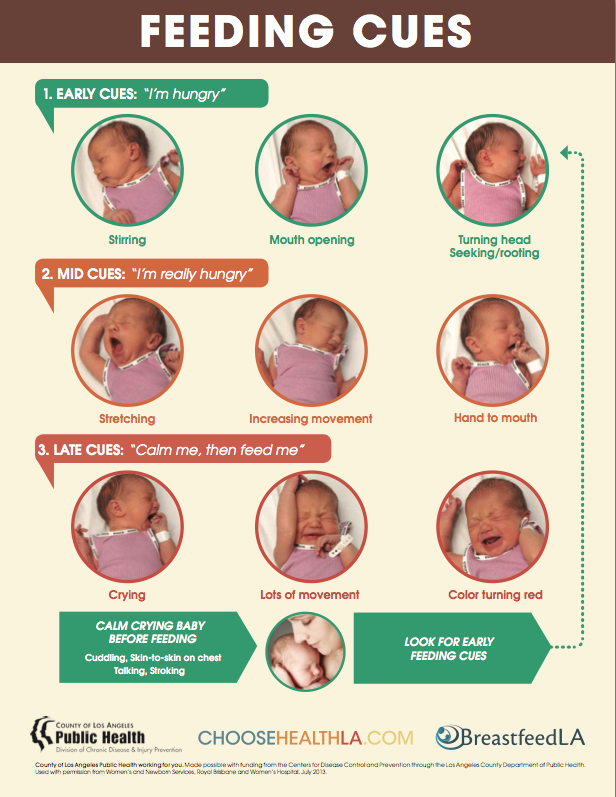 Therefore, the first thing the midwife does is wipe the baby with a warm diaper and lay it on the mother's stomach. Several factors come into play here: firstly, physical contact with the mother will maintain the child’s body temperature and warm him. Secondly, it will strengthen the psychological bond between mother and baby. And, thirdly, the child's sterile organism will be populated with new maternal microorganisms that will protect it from conditionally pathogenic or pathogenic microflora of the environment.
Therefore, the first thing the midwife does is wipe the baby with a warm diaper and lay it on the mother's stomach. Several factors come into play here: firstly, physical contact with the mother will maintain the child’s body temperature and warm him. Secondly, it will strengthen the psychological bond between mother and baby. And, thirdly, the child's sterile organism will be populated with new maternal microorganisms that will protect it from conditionally pathogenic or pathogenic microflora of the environment.
The next important moment is that the umbilical cord is cut for the newborn, the neonatologist examines the baby and puts an Apgar score. This scale is needed in order to determine which children need more attention. According to this scale, the health status of each newborn is assessed on five indicators: heart rate, respiration, muscle tone, reflexes, and skin color of the baby. During the examination, for each sign (heart rate, breathing, muscle tone, reflexes and skin color) give 0, 1 or 2 points. A score of 2 points in the delivery room is considered the highest and means that the sign is pronounced, 1 point - weakly expressed, 0 points - the sign is absent. The child is evaluated on the Apgar scale at the 1st and 5th minutes of life, so there are always two scores, for example 8/9points or 9/10 points. Children rarely score the maximum 10 points in the first minute of life, and usually the first score is always lower than the second. But the second assessment can just be equal to 10 points. Children who score between 7 and 10 are considered to be in good condition and generally require only routine care. Those who score between 4 and 6 are in fair condition and may only need some resuscitation procedures. Immediate life-saving assistance is necessary for those whose score is below 4. Apgar score - no matter what it will be (low or high) - this is not a diagnosis. This is a signal for the doctor about what measures are now needed or, conversely, the child does not need.
A score of 2 points in the delivery room is considered the highest and means that the sign is pronounced, 1 point - weakly expressed, 0 points - the sign is absent. The child is evaluated on the Apgar scale at the 1st and 5th minutes of life, so there are always two scores, for example 8/9points or 9/10 points. Children rarely score the maximum 10 points in the first minute of life, and usually the first score is always lower than the second. But the second assessment can just be equal to 10 points. Children who score between 7 and 10 are considered to be in good condition and generally require only routine care. Those who score between 4 and 6 are in fair condition and may only need some resuscitation procedures. Immediate life-saving assistance is necessary for those whose score is below 4. Apgar score - no matter what it will be (low or high) - this is not a diagnosis. This is a signal for the doctor about what measures are now needed or, conversely, the child does not need.
Next, the neonatologist continues to examine the newborn. The doctor looks at how the baby is formed, whether he has any developmental anomalies or any other problems. After that, the newborn is washed, measured, weighed, and a tag with the name of the mother and the time of birth is attached to the handles. Then the child is wrapped in a diaper and applied to the mother's breast. Almost always at this time (within 10–20 minutes after birth), the baby calms down and falls asleep. What happens next depends on the design of the maternity hospital. In some maternity hospitals, for the next two hours, the mother and the newborn are in the maternity ward, in others the child is taken to the children's ward. In any case, if there is an opportunity to be together, you must ask to leave the baby next to you, if the child feels well, this is quite possible.
The doctor looks at how the baby is formed, whether he has any developmental anomalies or any other problems. After that, the newborn is washed, measured, weighed, and a tag with the name of the mother and the time of birth is attached to the handles. Then the child is wrapped in a diaper and applied to the mother's breast. Almost always at this time (within 10–20 minutes after birth), the baby calms down and falls asleep. What happens next depends on the design of the maternity hospital. In some maternity hospitals, for the next two hours, the mother and the newborn are in the maternity ward, in others the child is taken to the children's ward. In any case, if there is an opportunity to be together, you must ask to leave the baby next to you, if the child feels well, this is quite possible.
With mother or in the children's department
Now almost everywhere you can be with a child both together and separately. But again, it all depends on the device of the maternity hospital. If a woman lies separately from the baby, then she will take him for feeding. The sisters of the children's department will take care of the child, wash, change diapers, change clothes. But you need to understand that they do this according to a schedule that is the same for all children in the department, and not according to the individual needs of the child.
If a woman lies separately from the baby, then she will take him for feeding. The sisters of the children's department will take care of the child, wash, change diapers, change clothes. But you need to understand that they do this according to a schedule that is the same for all children in the department, and not according to the individual needs of the child.
If the child lies with his mother, then his regimen is already determined by her. Mom can feed the baby on demand, and not by the hour, as with a separate stay. And she also changes the diaper or changes it when it is really necessary (the child peed and the diaper is full), and not according to some schedule that is the same for everyone. It turns out that a connection is established between mother and child faster, it is easier for a woman to understand what the baby needs, why he is crying and what to do with him. If a mother already at the maternity hospital learns to wash and change a child, change his diaper, upon returning home, she will adapt much easier to a new life and a new daily routine. The second important plus of living together is that breastfeeding is established faster, and when feeding on demand, milk will come faster.
The second important plus of living together is that breastfeeding is established faster, and when feeding on demand, milk will come faster.
Some women believe that after giving birth they need to rest, be apart from the child, they say, they are taking care of him in the children's department, and for now I will come to my senses and get used to my new state. Yes, if the birth was difficult and the mother endured it hard, then you need to rest. But since childbirth is still a physiological process, a woman recovers very quickly and even after a difficult birth, on the second day, she may well take the child to her ward. After all, judge for yourself - she won’t have to do anything special: she doesn’t cook dinner (the maternity hospital provides food), then she doesn’t wash the dishes, she doesn’t clean or wash anything (the maternity hospital even gives out clean clothes daily). Almost all newborns do not cry in the first days after childbirth, but sleep all the time, and it turns out that the only concern of the mother is to breastfeed the baby several times a day and change the diaper. So a woman will have enough time to rest, and why not use it for business? And one more thing: those who gave the child to the children's department like to blame later that he was supplemented with formula there, although the woman asked not to do this. But imagine the situation: the child cried, his sister examined him - he was washed, changed clothes, that is, everything is in order with him, but he, nevertheless, cries. What will mom do - take the baby in her arms, shake, calm. But the sister of the children's department has many more children nearby, they also need to be looked after. What is the way out - either give a bottle with a mixture or wait for other children to “turn on” from the endless crying of the child.
So a woman will have enough time to rest, and why not use it for business? And one more thing: those who gave the child to the children's department like to blame later that he was supplemented with formula there, although the woman asked not to do this. But imagine the situation: the child cried, his sister examined him - he was washed, changed clothes, that is, everything is in order with him, but he, nevertheless, cries. What will mom do - take the baby in her arms, shake, calm. But the sister of the children's department has many more children nearby, they also need to be looked after. What is the way out - either give a bottle with a mixture or wait for other children to “turn on” from the endless crying of the child.
First examinations, tests, vaccinations
While the newborn is in the hospital, he will be examined by a neonatologist every day. The doctor will either come to the ward to see the mother and the baby, or the child will be taken to the children's department. The doctor must coordinate all manipulations, appointments with the mother, and be sure to tell about all the results of the examination. But he himself will not be able to guess what exactly the woman is interested in, so doctors usually say the main thing, for example: "Everything is in order with the child, he has been examined, no pathology has been detected, he is gaining weight." If you need a more detailed answer, formulate your questions in advance, let's say again: the doctor does not know what interests you - how to care for the navel or why the child has a red spot on his face.
The doctor must coordinate all manipulations, appointments with the mother, and be sure to tell about all the results of the examination. But he himself will not be able to guess what exactly the woman is interested in, so doctors usually say the main thing, for example: "Everything is in order with the child, he has been examined, no pathology has been detected, he is gaining weight." If you need a more detailed answer, formulate your questions in advance, let's say again: the doctor does not know what interests you - how to care for the navel or why the child has a red spot on his face.
If necessary, the child will be examined by other specialists: an ophthalmologist or a neurologist. The newborn will be required to determine the blood type and Rh factor, and also take a blood test for severe congenital diseases (the so-called screening). The fact that these tests have been carried out will be indicated in the children's part of the exchange card (it will be issued upon discharge). The child may also be assigned some additional studies: a general and biochemical blood test, a general urine test. Also, if necessary, the newborn will undergo an ultrasound examination of the abdominal organs, brain (neurosonography), heart (echocardiography).
The child may also be assigned some additional studies: a general and biochemical blood test, a general urine test. Also, if necessary, the newborn will undergo an ultrasound examination of the abdominal organs, brain (neurosonography), heart (echocardiography).
As for vaccinations, according to the national vaccination calendar, the first vaccinations are done at the maternity hospital. On the first day of life - from hepatitis B, on the full second day - from tuberculosis. If parents do not want to be vaccinated, then you must inform the doctor about this in advance and write a refusal to vaccinate.
Upon discharge from the maternity hospital, the mother will be given two parts of the exchange card. One of them will contain information about childbirth, and it will have to be taken to the antenatal clinic. The second part of the exchange card will contain data on the child, screening, vaccinations and examinations - it is given to the children's clinic. The next day after the mother and baby return home from the maternity hospital, they will be visited by the health visitor of the polyclinic, and the next day by the pediatrician. And now the specialists of the children's polyclinic will monitor the newborn.
And now the specialists of the children's polyclinic will monitor the newborn.
As you can see, the child in the maternity hospital will be under control all the time. Mom, doctors, children's sisters - they will all give him the attention he needs. The main thing for a woman in a maternity hospital is to be active, ask doctors, nurses, learn how to care for a baby, and establish breastfeeding. And then she will return home as a confident and savvy mom!
- Apgar score - no matter what it will be (low or high) - this is not a diagnosis. This is a signal for the doctor about what measures are now needed or, conversely, the child does not need
- If a woman lies separately from the baby, then she will take him to feed. The sisters of the children's department will take care of the child, wash, change diapers, change clothes. But you need to understand that they are doing this according to a schedule that is the same for all children in the department, and not according to the individual needs of the child
- Laying the baby on his stomach after childbirth will maintain his body temperature, strengthen the psychological bond between mother and baby.
 And the child’s sterile organism will be populated with new maternal microorganisms that will protect it from conditionally pathogenic or pathogenic microflora of the environment
And the child’s sterile organism will be populated with new maternal microorganisms that will protect it from conditionally pathogenic or pathogenic microflora of the environment
Memo for moms
While you are in the hospital
- If possible, take the child to your room. So you will quickly get used to it, establish breastfeeding and learn how to care for the baby.
- If you don't know how to wash, change or swaddle your baby, ask the Nursing Nurse to show you how to do it. Do it yourself at least a few times.
- Ask your midwife in the postnatal unit to show you how to properly latch your baby to the breast.
- Ask the neonatologist what examinations the child has had and what he would like to do in the future.
- Be active - ask the doctor and nurses any questions about the baby.
Attention! Prices for services in different clinics may vary. To clarify the current cost, select the clinic
The administration of the clinic takes all measures to update the prices for programs in a timely manner, however, in order to avoid possible misunderstandings, we recommend that you check the cost of services by phone / with the managers of the clinic
Clinical Hospital IDKChildren's Clinic "Mother and Child" Samara
All directionsSpecialist consultations (children)Massage / manual therapy for childrenTherapeutic research
01.