Baby gags on textured food
Textured Foods: How to Transition Baby from Puree to Table Food
Is your baby refusing to eat food other than purees? Not sure how to introduce textured foods to your baby? Here are some expert tips from a registered dietitian.
Jump to:- When to Move to Textured Foods
- How to Transition to Table Food
- What If your Baby Stops Eating
- Role Model!
- I want to leave you with this:
When to Move to Textured Foods
Generally speaking, most babies are ready to transition from purees to textured foods between 6-9 months.
Is your baby 6 months old and up?
Learn all the secrets to starting solids safely while optimizing nutrition!
I NEED IT NOW!
If you decide to take the baby led weaning approach, then your baby will learn to handle textures from the start.
If you’re starting out with purees, it's best to keep this stage pretty short. That’s because research shows that infants who are introduced to textures by 9 months generally have less feeding problems and greater food acceptance down the road.
Therefore, you need to gently challenge your baby with new food consistencies. Otherwise, they will get used to just swallowing and not learn to move food around in their mouth and chew. All this leads to an increased aversion to textures.
If you haven’t decided which feeding method is right for you and your family, then check out this post - Starting Solids - Purees vs. Baby led weaning.
And remember, babies don’t need teeth to chew! It's amazing what their gums are capable of!
The Benefits:
- Increased acceptance of variety
- Strengthening of baby’s jaw muscles
- Promotes speech development
How to Transition to Table Food
First, if you've started on purees and feel stuck, allow me to guide you!
Every child is different and contrary to what you may have been told, you don’t necessarily have to introduce textured foods in any specific order or stages. Everything you see in the visual is appropriate and safe to serve to your baby.
Everything you see in the visual is appropriate and safe to serve to your baby.
But your baby or you might need the gradual progression. Perhaps your baby has a very sensitive gag reflex or other underlying issues. ALWAYS do what feels best and comfortable for you and your family. Just remember not to stay at any one stage for too long.
You can start by thickening the baby purees to encourage the use of the tongue and muscles in the mouth to start the chewing process. This can be accomplished by adding less water or liquid when pureeing.
If you've been spoon-feeding, try preloading the spoon (here's one that I highly recommend!) and either place on the table or hold it out for them to grab.
Then move onto lumpy to mashed to soft minced and chopped up foods along with soft finger foods. Here are easy ways to incorporate vegetables for babies 6 months and up!
Oatmeals/porridges are a great place to start. Try offering these oatballs. Add finely chopped vegetables or fruits to quinoa cereal.
Additionally, don’t think you can’t serve the previous texture once you move on. It’s important to continue exposing them to a wide variety of textures.
Safety Tips
- Always stay close to your baby.
- Make sure your baby is secured tightly in a highchair, sitting upright and not leaning back. Their feet need to be supported as well!
- Be sure to serve age-appropriate food size and texture.
- Avoid foods that are small and round (e.g. grapes, blueberries), hard (raw vegetables, nuts), or sticky (thick nut butter, candy) as they are choking hazards.
Is it going to be messy? Absolutely! As hard as it may be, learn to embrace it as it's SUCH an essential part of the self-feeding journey. In the meanwhile, here are some products that I recommend
What If your Baby Stops Eating
from my IG account: @kidfriendly.mealsBe Patient
It’s normal for your baby to resist texture at first because it’s unfamiliar and feels unsafe. While it's tempting to continue serving just purees, DON'T fall back! Keep marching forward otherwise your baby will never learn.
While it's tempting to continue serving just purees, DON'T fall back! Keep marching forward otherwise your baby will never learn.
Of course you worry when your baby doesn't eat as much as you think they should, but by no means should you rush them or force-feed. You do need to gently and lovingly pressure/challenge them by continuing to offer.
Remember, learning to chew and swallow different textures takes time to master so keep giving them plenty of opportunities to practice in a safe, pleasant, and encouraging eating environment! That’s the best thing you can do!
Again, your baby is most likely not going to consume much, if any, at first. But remember, at this age, exploring all the different textures and advancing their oral motor skills (moving food around the mouth, chewing, etc.) is much more important than the amount of food that actually makes it into the belly.
With continuous exposure and practice, your baby will gain the skills and confidence needed to handle textured foods. And you'll be so glad that you stuck with it and didn't give in.
And you'll be so glad that you stuck with it and didn't give in.
As you navigate through this challenging transitional period, I hope these reminders provide some much needed reassurance and peace of mind.
- Your baby’s appetite will vary from day to day.
- Their tummies are tiny so they don’t need much.
- Breastmilk/formula will continue to be the main source of nutrition during the 1st year. If your baby didn't eat much, you can offer milk about 30-45 minutes after the meal has ended (don't offer immediately after). That way they're still getting the nutrition they need, and they won't make the association of "ooh if I don't eat, mommy will give me milk!"
Gagging
Most likely, there will be a lot of gagging. This is again quite normal as your baby learns to handle new textures. It’s a safety mechanism that actually helps prevent choking and helps your baby in learning to manage food safely.
So don’t fall back on offering the safer purees. Again, gently challenge them to accept new textures and to learn to chew by offering a variety.
Again, gently challenge them to accept new textures and to learn to chew by offering a variety.
On the other hand, if the gagging persists and your baby is visibly upset then it’s best to consult with your physician to make sure there aren’t any other underlying issues, like oral motor delays, sensory sensitivity, or a medical condition, that need to be addressed.
Spitting
As babies are learning to chew and swallow, they will likely spit out food that is too large to swallow. It's also a part of learning to chew. So don't intervene. Let it be.
Role Model!
It's important to keep the mealtime environment safe and positive. Offer different textured foods without pressure and encourage your baby's curiosity with exploring the food. The best thing you can do is have your baby join the family during mealtimes as much as possible. They learn so much from simply watching what you do. The more they see everyone enjoying their food, laughing, and having a grand ole time, the more they're going to want to be a part of it.
Show how you grab food with your hand and bring to your mouth. Exaggerate chewing with your mouth open. This is not the time to mind your table manners.
EACH and EVERY time your baby is exposed to new flavors and textures, they are learning and gaining confidence from it.
I want to leave you with this:
Be patient. Continue to offer a wide variety of textures (and flavors!). Trust the process! It's one bumpy ride and we need to be in it for the long-haul. And if you need a step-by-step guidance, check out my 3 month program below. It's complete with daily cooking demos, game plan, recipes, etc. to help you to move beyond purees!
Do you want to minimize picky eating and set a solid foundation for a lifetime of healthy eating habits?
Check out this 3 month mastering self-feeding program! It’s the closest thing to me being in your kitchen
What to do if your baby doesn't like baby foods, purees, or solids
Introducing your baby to solid foods can be fun and photo-worthy, but this milestone can also come with some challenges.
It's normal for babies to balk the first time (or many times) they try new solid foods, since they've only ever had breast milk or formula. Don't be discouraged if your baby refuses food at first – it can take 10 or more tries sometimes to get your baby to eat a new food.
The key at any age is to offer your baby a wide variety of foods and keep trying. Even if they don't like the food at first, keep offering it to them – babies learn to love what they're given. If they don't like sweet potato, maybe they'll like squash. Once they get used to squash, try mixing squash with sweet potato to get them used to the new flavor. If they don't like bananas, try avocado and then go back to bananas for another try.
But if you're serving your baby different foods and nothing's working, read on.
If your baby won't eat solids
If your baby is about 6 months old and is developmentally ready for solid foods (has good head control, is grasping, can sit up on their own), but doesn't seem interested in food, they may just not be ready to dive in yet.
Some babies need a little more time to develop curiosity around food. Take it slow – if you try to give your baby one kind of puree and they refuse it, wait a few days and try a different puree. In the meantime, make family meals fun and engaging by talking to your baby about the food you're preparing and letting them watch you eat.
If your baby is struggling with purees, baby-led weaning could be a good alternative. This method encourages your baby to explore food on their own. Simply offer your child safe foods, like soft scrambled eggs or long spears of very ripe banana, and let them experiment with how the food feels in their hands and mouth.
Keep in mind that whether you start with pureed foods or try baby-led weaning, gagging is perfectly normal while your baby learns to feed themself. The gag reflex helps bring food to the front of the mouth so your baby learns how to chew.
If your baby won't eat finger foods
If your baby is 9 months or older and they don't like finger foods and thicker purees, there could be a few reasons. If your baby has primarily been spoon-fed by you up until now, they may need some time to get the hang of feeding themselves finger foods.
If your baby has primarily been spoon-fed by you up until now, they may need some time to get the hang of feeding themselves finger foods.
Advertisement | page continues below
Or they may not be ready yet – babies can't pick up and feed themselves finger foods well until they learn the pincer grasp. This usually happens around 8 to 10 months, but if you're baby's a little behind, don't worry. They may just need some extra time to learn, and some encouragement from you can help.
You can help your baby master their grabbing skills by giving them lots of toys that are easy to grasp, like soft blocks, plastic rings, and board books. Play a little game with them by putting a colorful toy in front of them and encouraging them to grab it.
Some babies also have a sensitive gag reflex that makes them gag on lumpy food. (They may have had difficulty latching on when nursing as infants.) If your baby has trouble eating textured or lumpy food without gagging, sticking to thin purees may feel safe, but this could get in the way of helping your child learn how to chew.
Teach your baby to tolerate lumpy food by adding ingredients with a uniform texture – like wheat germ or cracker crumbs – to pureed food. Start with a small amount and add more as your baby gets used to the texture. You can also try giving them solids that will dissolve easily in their mouth, like baby crackers, to help them get used to new textures.
If your baby doesn't like the texture of meat, try a different preparation: For example, if your baby won't eat diced chicken breast, try giving them ground chicken or thinly sliced deli meat instead.
If your baby is sensitive to the texture of finger foods, experiment with introducing different textures in other ways – give your baby feathers, a bumpy ball, or cooked noodles to play with. (Just make sure to supervise in case small items end up in your baby's mouth.) Teething toys that have bumps may help, too. Getting used to new sensations at playtime might make your baby more open to unfamiliar food textures.
If your child still rejects lumpy or textured solid food at a year old, or if they aren't able to feed themself finger foods by 12 to 15 months, check in with your child's doctor. It could indicate that your child has a developmental problem or sensory issue that may be improved with the right help.
It could indicate that your child has a developmental problem or sensory issue that may be improved with the right help.
Severe difficulty eating a wide range of foods is common among kids with autism spectrum disorder (ASD) or sensory processing disorder (SPD), but picky eating isn't the only sign of these conditions. Talk to the doctor if you have any concerns.
Child chokes on food | Mamovediya
Although the reluctance to swallow solid food is a natural response in many situations, and not just those involving food, infants and young children should not constantly choke.
If your child is constantly choking, or the face starts to turn red, or the skin around the lips turns blue, take your child to the doctor. In rare cases, this may indicate a problem requiring medical attention. nine0005
Although your father may be alarmed that you choke on the first spoonful of solid food, this happens quite often when the child starts eating. You have to learn to eat solid food.
In the sucking reflex, babies move their tongue to the front of their mouth and then up to the palate. They make 10 to 20 sucking movements, and then a big gulp follows. With solid food, however, the tongue must almost reverse, sending the food to the back of the mouth. nine0010
Learning to swallow solid foods is not easy for an infant. And during the learning process, he may choke if food is directed to his windpipe instead of his stomach.
You can, however, make eating a much easier exercise when the baby does not choke. To do this, you need to master new feeding techniques.
Here are some expert tips.
Wait until the child starts to sit up. If your child is constantly choking on food while eating, it is possible that he has not yet reached the stage of development at which he is ready for this. Your baby must be at least four or five months old before you start solid food. nine0003
What is the advice? Give the child solid food when he has already learned to sit more or less confidently. When your child eats while seated, gravity will help guide the food from the mouth into the esophagus.
When your child eats while seated, gravity will help guide the food from the mouth into the esophagus.
Start with liquid food . When your baby is really hungry, breastfeed or give him a bottle first to satisfy his appetite a little. If your child is not so desperately hungry, he will be able to handle the difficult task of swallowing solid food more easily. nine0003
Eat rice. Rice grains are an ideal first food for children because children are rarely allergic to rice and can be thinned by mixing with plenty of milk.
Your baby will have less difficulty eating porridge if the consistency is more like liquids he is used to swallowing. Once your baby has learned to swallow rice porridge, you can gradually move on to thicker, coarser foods. nine0003
Let the first feedings be small . The first solid food feedings are for practice, not for real nutrition. An infant who is learning to eat only needs a few tablespoons of solid food a day to practice eating. The main nutrition should come from breast milk or artificial bottle feeding.
The main nutrition should come from breast milk or artificial bottle feeding.
Start with a small amount of food . When your child opens his mouth, place a pea-sized portion of food on the front of his tongue. A large portion of food will make the whole process of swallowing more difficult for him, and if you put it on the back of the tongue, your child is likely to choke on it. nine0003
Do everything calmly, carefully and slowly. Take your time if your child is having difficulty with a new food.
If your child chokes on a particular type of food, such as potatoes or minced meat, pediatricians recommend not eating the food for a few days, then trying it again in a thinner consistency.
Do not overfeed your baby. If your baby vomits or chokes on every feed, it is possible that you are giving him more than he can handle. nine0003
In the first year of life, the baby cannot properly control the intake of food, so your task is not to overfeed him.
Watch for signs that the baby is full. He may begin to turn his head away or close his mouth when the spoon comes close to his lips.
An aging person: about what happens to us with age
An aging person: about what happens to us with age
What is an aging person and what is developing? nine0010 The article focuses not on biochemical and morphological aspects, but on the personality - on the process of individual development of a person, because it never stops. There is no need to think that after adolescence, a person reaches a plateau, as scientists call "acme", the highest point of development, and then degrades. Aging is not degradation. This is a process of continuing development, a very peculiar one.
Normal aging, according to our psychological school, is a process of continuous, progressive, uneven, complex growth of various limitations. There are purely physiological ones: hearing is reduced, specific forms of diseases appear that are not actually diseases, but there are normal symptoms of aging associated with movements, muscles, sensory systems, psychology, and so on, and, of course, social restrictions arise that are in the individual consciousness of an aging person are refracted and turn into existential ones. The unevenness of the process gives rise to individual differences. Modern methods of scientific research, prone to statistical processing and quantitative analysis of data, unfortunately, do not help to reveal the essence of the mechanisms that lie behind it, because aging is extremely individual. nine0003
The unevenness of the process gives rise to individual differences. Modern methods of scientific research, prone to statistical processing and quantitative analysis of data, unfortunately, do not help to reveal the essence of the mechanisms that lie behind it, because aging is extremely individual. nine0003
Why? Speaking rather roughly, here is a child. As soon as he is born, he immediately enters the society where he is looked after, but nature is arranged in such a way that a certain program is laid in the genetics of a new person that gives him a minimum range so that he survives. Therefore, early ontogeny, that is, early individual differences from birth to preschool age, is sufficiently programmed. We know the standards: when a child should be able to hold his head, say the first word, what kind of words should be, when he should have phrasal speech, when he should start walking, crawling, and so on. If there are deviations in the standards, we say that this is abnormal, pathological, something needs to be done about it - the correction should be medical, because these programs are biological. In adulthood, development is already more directed, social: a person shows his own activity, and so on. He reaches the third age, that is, the age of aging, with already very serious baggage - knowledge, experience, experiences, psychological trauma, views, meanings, values. All this colossal baggage, of course, makes the natural biological program very noisy. Therefore, aging is individual precisely because of individual experience. Thus, we are not very good at finding biological causes using natural science methods. Therefore, all the data on individual differences that I will give are clinical. That is, collected not on patients, but through long-term, many years of observation - including our department and me. nine0003
In adulthood, development is already more directed, social: a person shows his own activity, and so on. He reaches the third age, that is, the age of aging, with already very serious baggage - knowledge, experience, experiences, psychological trauma, views, meanings, values. All this colossal baggage, of course, makes the natural biological program very noisy. Therefore, aging is individual precisely because of individual experience. Thus, we are not very good at finding biological causes using natural science methods. Therefore, all the data on individual differences that I will give are clinical. That is, collected not on patients, but through long-term, many years of observation - including our department and me. nine0003
Nevertheless, it is possible to distinguish individual differences, which we call style, variant or type, that is, to distinguish a certain typology of normal aging based on how the brain works. In the 1930s and 1950s, a prominent Soviet researcher, psychologist Alexander Romanovich Luria, discovered the science to the world, which he called neuropsychology. She was born in the Soviet Union and is accepted all over the world. Indeed, this is our achievement, one of the few that is definitely ours. Luria studies patients with local lesions of the brain, presenting various kinds of tests, showing that when certain structures are damaged, certain symptoms of violations of higher mental functions arise, such as memory, thinking, attention, speech, and so on. He concluded that if a patient is given a certain test that will demonstrate certain disorders of mental functions, then these zones are responsible for the implementation of these mental functions. nine0003
She was born in the Soviet Union and is accepted all over the world. Indeed, this is our achievement, one of the few that is definitely ours. Luria studies patients with local lesions of the brain, presenting various kinds of tests, showing that when certain structures are damaged, certain symptoms of violations of higher mental functions arise, such as memory, thinking, attention, speech, and so on. He concluded that if a patient is given a certain test that will demonstrate certain disorders of mental functions, then these zones are responsible for the implementation of these mental functions. nine0003
In the 1970s and 1980s, Natalya Konstantinovna Korsakova, a student of Alexander Romanovich Luria, began working at the Mental Health Research Center, where she was offered to use the methods developed by Luria to diagnose Alzheimer's disease in order to understand exactly how the brain is affected. And indeed, by presenting these tests, the Lurian methods that were developed for people with brain tumors, she shows that patients with Alzheimer's disease experience very similar symptoms, similar to those that occur in patients with tumors of the parietal, frontal lobes. , temporal, subcortical structures of the brain. Korsakova concludes that in Alzheimer's disease and other forms of senile dementia, severe mental disorders of senile age, specific cognitive impairments are observed. This means that this pathological process, not tumorous, but atrophic, spreads in each individual case with a different disease to certain areas of the brain. This is how the science of neurogerontopsychology is born. Scientists became interested in what happens in old age in the norm. Having studied more than 300 healthy people from 50 to 100 years old who never went to the doctors about mental health and neurological problems, Korsakova identifies various neurocognitive styles, a typology of normal aging. It shows how we and our psyche are aging in connection with the work of the brain. These data are indirectly confirmed by Western studies using neuroimaging, functional tomography, positron emission tomography, and so on. nine0003
, temporal, subcortical structures of the brain. Korsakova concludes that in Alzheimer's disease and other forms of senile dementia, severe mental disorders of senile age, specific cognitive impairments are observed. This means that this pathological process, not tumorous, but atrophic, spreads in each individual case with a different disease to certain areas of the brain. This is how the science of neurogerontopsychology is born. Scientists became interested in what happens in old age in the norm. Having studied more than 300 healthy people from 50 to 100 years old who never went to the doctors about mental health and neurological problems, Korsakova identifies various neurocognitive styles, a typology of normal aging. It shows how we and our psyche are aging in connection with the work of the brain. These data are indirectly confirmed by Western studies using neuroimaging, functional tomography, positron emission tomography, and so on. nine0003
What is aging phenomenologically?
First, of course, this is a slowdown in the pace of activity. Latency is growing, people at the third age begin to work more slowly. This slowness becomes especially evident at the initial stage of activity. It becomes especially difficult to quickly extract information, to link it. You need to be able to negotiate with your memory after 55 years, so that it gives out what you need.
Latency is growing, people at the third age begin to work more slowly. This slowness becomes especially evident at the initial stage of activity. It becomes especially difficult to quickly extract information, to link it. You need to be able to negotiate with your memory after 55 years, so that it gives out what you need.
Secondly, a person starts to work as a single-channel system. If he reads a newspaper, then the TV no longer hears and does not think about things that are not related to this newspaper. nine0003
As for the speech sphere, an elderly person should speak not only slowly, but also in a low voice. Not necessarily loud, although age-related hearing loss can also occur, but a velvety baritone or even bass will be learned better than tenor and falsetto. This is a purely sensory thing, scientifically proven.
Fourth, tempo characteristics. Speech information can be absorbed more slowly than non-verbal information. There is a certain imbalance, stealing the right hemisphere in favor of the left. The left hemisphere begins to work more intensely due to the fact that it may lose some right hemisphere functions. But nevertheless, not always and quite fragmentarily, therefore, for example, music is assimilated well, and listening to songs of youth actualizes the deep layers of memories. nine0003
The left hemisphere begins to work more intensely due to the fact that it may lose some right hemisphere functions. But nevertheless, not always and quite fragmentarily, therefore, for example, music is assimilated well, and listening to songs of youth actualizes the deep layers of memories. nine0003
The tactile sphere literally comes to life, that's why people love to sort through things, dust, so it's better to give the elderly textured gifts, textured ones - this also actualizes the thresholds of memory layers.
About memory. Access to direct memories of what happened now is becoming more closed. Access to early memories of youth, youth and even childhood is opened. They become brighter and more distinct. Traces of memory are not erased: we remember everything, we just do not always have access to it. nine0003
And finally, this is a decrease in the ability to learn new things and difficulties in setting creative tasks. Not because the person becomes demented, but because there is not enough energy to keep the creative process going, which, as you know from all the metaphors, must gusher.
Types of normal aging
This typology is based on the concept of Alexander Romanovich Luria about the structures of the functional blocks of the brain. On the basis of his numerous studies, he divided the brain into three blocks not according to the morphological structure, but according to the roles that brain structures play for the implementation of higher mental functions. nine0003
Energetic neurocognitive style of aging
The most common, universal. It is associated with a decrease in the functions of the energy supply of mental activity: people become slower, they experience the “on-off” phenomenon - “on-off”. That is, a person starts reading a book, it’s difficult, it’s not vulgar, he closes it, goes to the kitchen and helps his wife cook borscht, that is, it is activated. These fluctuations can be observed quite gently, they should not disturb the adaptation. With vascular lesions of the brain, this effect can disrupt it. That is, a person may not cope with the task in the "off" state, and in the "on" state, he may become too excited. He cries, he laughs. There are such clinical examples. nine0003
That is, a person may not cope with the task in the "off" state, and in the "on" state, he may become too excited. He cries, he laughs. There are such clinical examples. nine0003
In addition, this is a narrowing of the volume of activity, a single-channel system of perception, slowness of memory traces and fatigue - non-specific characteristics of aging, not risk factors. The most important thing is that the cerebral cortex works well. That is, a person can come up with it himself, learn from past experience, plan, for example, that it will take him such a long time to get to the clinic, and in order to visit his grandchildren, such operations are needed; he can plan the day in a specific way. Inhibition, the inaccessibility of memories that are needed right now, means that you need to write it down, and a person understands all this. The risk factor that can lead a person to maladjustment is, of course, stress. Since the subcortical structures are emotions, stress resistance, the ways to regulate one's emotions become insufficient. That is, there may be emotional problems. nine0003
That is, there may be emotional problems. nine0003
This is also an exacerbation of bodily ailments. The most malignant one, which really unsettles a person and puts him into a state of disadaptation, anxiety, depression, is the femoral neck. Such a person needs special attention; perhaps professional psychological support. I'm not talking about cataracts and other purely age-related things - they, of course, also require special attention.
Spatial neurocognitive style of aging
The second type is a decrease in the ability to orientate in real and internal space. Already a specific type of aging, in which it becomes very difficult to holistically perceive various things. Reading even a short story and understanding what the point is can already become a problem. You must first read one paragraph, comprehend it, remember it, take a breather, then the second and so on. Technically, you can read a story, a person will not be exhausted, but he will not understand it. And the most important thing is “disadaptation” in the new space. Please note this is not a spelling error. That is, the person is not completely lost, but it is difficult for him in the new space, he begins to grab his right hand, thinking: “The right hand means I need to go to the right.” They have a marker that is actually programmed: “I write with my right hand,” which means you need to orient yourself to the right. They can stray for a very long time, but not in the sense that they are really lost, but because they have such difficulties in a new space. In the old familiar space, everything can be quite safe. nine0003
And the most important thing is “disadaptation” in the new space. Please note this is not a spelling error. That is, the person is not completely lost, but it is difficult for him in the new space, he begins to grab his right hand, thinking: “The right hand means I need to go to the right.” They have a marker that is actually programmed: “I write with my right hand,” which means you need to orient yourself to the right. They can stray for a very long time, but not in the sense that they are really lost, but because they have such difficulties in a new space. In the old familiar space, everything can be quite safe. nine0003
That is, the risk factors here are a change in the environment, for example, emigration. Our colleagues, Russian psychologists abroad, at one time published articles in journals devoted to Russian emigrants in France and the USA. They describe these phenomena on a very large scale, also in connection with the linguistic side. For example, the phenomenon of “pathological nostalgia”: an emigrant woman believed that she was in her Moscow apartment, she saw people from that life. These were not hallucinations due to mental illness, but a temporary condition, stress, culture shock. It has to do with the right hemisphere. nine0003
These were not hallucinations due to mental illness, but a temporary condition, stress, culture shock. It has to do with the right hemisphere. nine0003
The important thing to understand here is that these kinds of things can be very similar to Alzheimer's disease, but they need to be distinguished. Here are the statistics. Schizophrenia is 1%, but 10% is Alzheimer's disease, where 4% is early Alzheimer's. In our clinic, these are all women 40 years old. I remember the last case: 40 years old, a nurse and really severe symptoms associated with profound memory impairment. If you want to understand what it is, watch the amazing film "Still Alice" about early Alzheimer's. What happens to a person is shown with maximum reliability, with deep psychologism, insight into the essence of this painful condition. After 55–60 years old, this is already classic Alzheimer's, and the later one is called senile (lat. “senile”). Scientists say it's genetically programmed. Unfortunately, there are no methods to identify a person's risk of developing this disease before the disease occurs. The genetic constellation leads to an imbalance of acetylcholine and other neuropeptides, which leads to the formation of Alzheimer cells, that is, atrophy of nerve cells in certain departments, which leads to the fact that these cells do not work and the brain functions poorly. nine0003
The genetic constellation leads to an imbalance of acetylcholine and other neuropeptides, which leads to the formation of Alzheimer cells, that is, atrophy of nerve cells in certain departments, which leads to the fact that these cells do not work and the brain functions poorly. nine0003
There is no cure for Alzheimer's disease: all drugs prescribed are symptomatic and do not significantly improve the state of mental functions. And even more so, unfortunately, they do not prevent further malignant development (after the onset of the disease, a person lives no more than 10 years). This is gross exhaustion, that is, a person cannot actively work for 45 minutes, gross memory impairment, inability to remember material, spatial orientation disorder, confusion, that is, a person may not understand where he is, on the street or at home. You could once watch a grandfather in slippers on the street with an absolutely bewildered expression on his face, who sometimes screams, tries to call for help.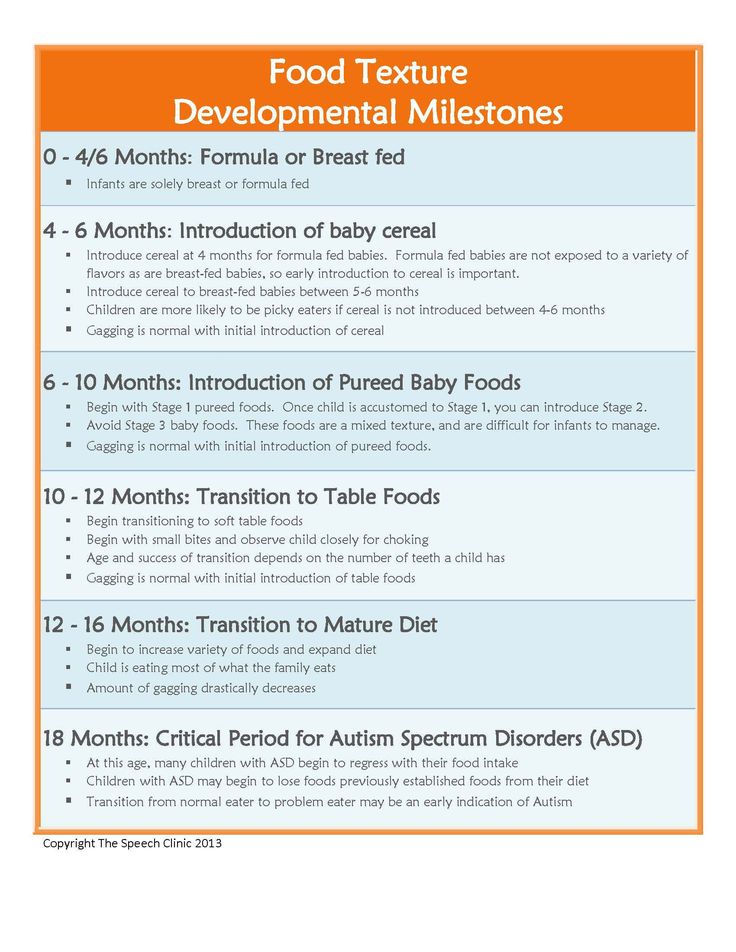 Of course, this is not yet a reason to diagnose him with Alzheimer's disease, but this is a pathological condition that very often accompanies it. Spatial disturbances come to the fore, that is, people cannot remember where the toilet is, where the kitchen is. But it is worth noting that their facade of personality is preserved, they experience this state, they are critical of it. Perhaps the whole tragedy lies in the fact that they understand that they are losing what makes up their personality. Because, according to one of the founders of Russian psychology, Sergei Leonidovich Rubinshtein, one of the central functions of memory is the structuring of personality. If memory disintegrates, all our experience disintegrates, the experience of communication with our personality, that is, the personality leaves. nine0003
Of course, this is not yet a reason to diagnose him with Alzheimer's disease, but this is a pathological condition that very often accompanies it. Spatial disturbances come to the fore, that is, people cannot remember where the toilet is, where the kitchen is. But it is worth noting that their facade of personality is preserved, they experience this state, they are critical of it. Perhaps the whole tragedy lies in the fact that they understand that they are losing what makes up their personality. Because, according to one of the founders of Russian psychology, Sergei Leonidovich Rubinshtein, one of the central functions of memory is the structuring of personality. If memory disintegrates, all our experience disintegrates, the experience of communication with our personality, that is, the personality leaves. nine0003
Regulatory neurocognitive style of aging
This is not yet a pathology, but it is already a truly risky option when the anterior parts of the cerebral hemispheres age first. This is where self-control comes in. This is the most central symptom as the frontal lobes are involved. Luria calls the third functional block of the brain a block of programming, regulation and control of mental activity, therefore here regulation and control suffer first of all. When they weaken a little, this is still the norm - what we in everyday life call “gray hair in a beard, demon in a rib”: a person is over 60, and he believes that he, as a young man, can do his job, behave like a young man, dress in torn jeans, walk with a player, say: “I listen to Dima Bilan, I won’t listen to Shulzhenko and Utyosov, I’m not that old yet.” There may also be sexualization of behavior. nine0003
This is where self-control comes in. This is the most central symptom as the frontal lobes are involved. Luria calls the third functional block of the brain a block of programming, regulation and control of mental activity, therefore here regulation and control suffer first of all. When they weaken a little, this is still the norm - what we in everyday life call “gray hair in a beard, demon in a rib”: a person is over 60, and he believes that he, as a young man, can do his job, behave like a young man, dress in torn jeans, walk with a player, say: “I listen to Dima Bilan, I won’t listen to Shulzhenko and Utyosov, I’m not that old yet.” There may also be sexualization of behavior. nine0003
In activities there may be problems with building plans, getting stuck at some points, inflexibility. Apathy, disturbance and decrease in motivation, which must still be preserved. Including the motivation to transfer semantic value experience to other generations: “Well, why should I call my grandson, he doesn’t need me.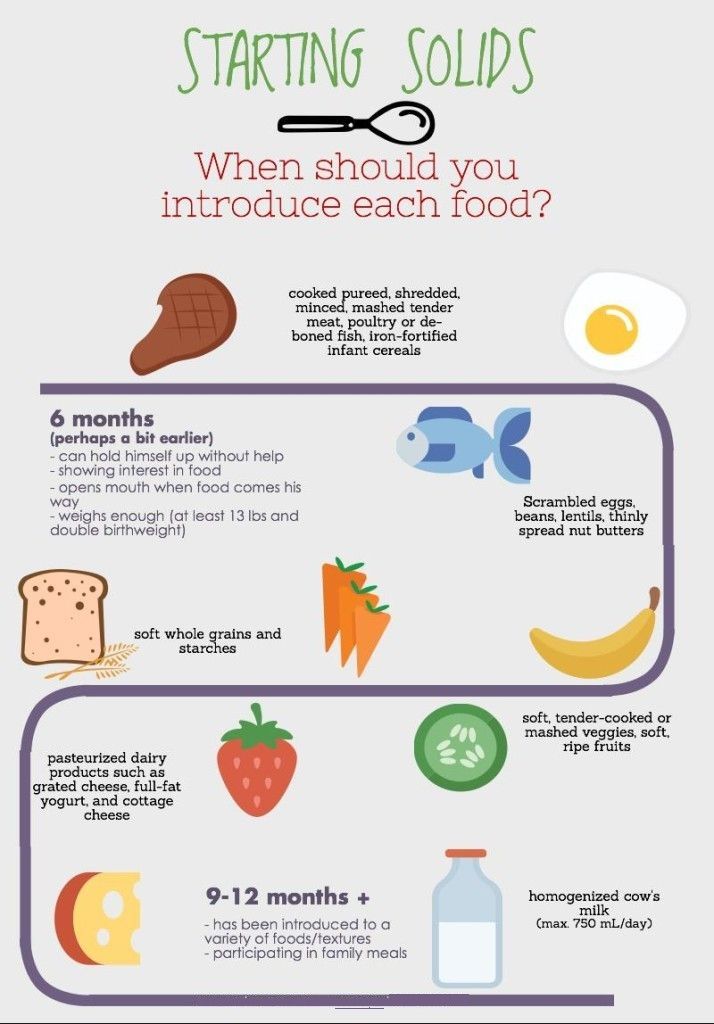 That I will get him." Experience of failure, loneliness, changing living conditions - all this can be a risk factor. Emotional, brutal reactions may follow. Against the background of stress, an elderly person may think: “What is it, my son came, he stole my passport. I can’t find my passport, because he came, he wants to do something with me.” That is, crazy ideas arise, but against the background of some kind of stress. nine0003
That I will get him." Experience of failure, loneliness, changing living conditions - all this can be a risk factor. Emotional, brutal reactions may follow. Against the background of stress, an elderly person may think: “What is it, my son came, he stole my passport. I can’t find my passport, because he came, he wants to do something with me.” That is, crazy ideas arise, but against the background of some kind of stress. nine0003
The extreme case, the pathological prototype here, is Pick's disease, which is also a classic disease, the pole of Alzheimer's disease. If the facade of the personality is preserved there, and the person is aware of and suffers from increasing cognitive impairment, then in Pick's disease (or, as it is now customary to say according to the newfangled psychiatric classification, in frontotemporal dementia), the anterior sections of the cerebral cortex are dysfunctional. Such patients are emotionally blunted, passive, indifferent, inactive, lying down, doing nothing. They are impoverished in motor skills, writing, reading, counting and are not critical of what is happening, but they are euphoric, they are complacent, they can laugh. At the same time, they are absolutely inactive, empty, moral and ethical attitudes are lost. There may be stereotypes, perseverations, that is, obsessive actions, and gross cognitive impairments, that is, speech disorders, grammatical structure, impoverishment of speech production, unwillingness to speak, build a detailed statement, and so on. First of all, and at the beginning, this emotional and personal dysfunction appears, at a later stage, some cognitive impairments are added. Now that's maladjustment. nine0003
They are impoverished in motor skills, writing, reading, counting and are not critical of what is happening, but they are euphoric, they are complacent, they can laugh. At the same time, they are absolutely inactive, empty, moral and ethical attitudes are lost. There may be stereotypes, perseverations, that is, obsessive actions, and gross cognitive impairments, that is, speech disorders, grammatical structure, impoverishment of speech production, unwillingness to speak, build a detailed statement, and so on. First of all, and at the beginning, this emotional and personal dysfunction appears, at a later stage, some cognitive impairments are added. Now that's maladjustment. nine0003
What prevents pathological aging?
People who have been engaged in intellectual work throughout their lives suffer from dementia of late age less. Gymnastics technologies for the brain have been developed separately, that is, if there are already some limitations in the cognitive sphere, then you can turn to psychologists who will develop an individual training program. Of course, I know old people who learn poetry themselves. It’s like a separate activity: we got up, had breakfast, walked the dog, then a couple of hours to learn a new poem, called a friend in the Moscow region, read it by heart, played chess on the phone, which is also good, you can see how e2-e4 correlate, then you can eat again, then walk the dog again. That is, it is a planned activity, where there is a cognitive and intellectual component to maintain tone. The tone is maintained in this way - through intellectual activity. nine0003
Of course, I know old people who learn poetry themselves. It’s like a separate activity: we got up, had breakfast, walked the dog, then a couple of hours to learn a new poem, called a friend in the Moscow region, read it by heart, played chess on the phone, which is also good, you can see how e2-e4 correlate, then you can eat again, then walk the dog again. That is, it is a planned activity, where there is a cognitive and intellectual component to maintain tone. The tone is maintained in this way - through intellectual activity. nine0003
In people who constantly maintained physical activity, the risk of dementia of late age decreases due to the fact that the metabolism works better, which means that atherosclerotic plaques do not form, sugar normalizes, and so on. That is, things that are purely connected with the vessels no longer make a pathological contribution.
Mode. It has been shown that people who drink alcohol are more likely to suffer from dementia of late age. The so-called Mediterranean diet is useful: proteins, seafood, phosphorus, fresh vegetables. Those who have a clear pattern of sleep and wakefulness get sick less. nine0003
Those who have a clear pattern of sleep and wakefulness get sick less. nine0003
And then pure psychology. People who experienced psychotraumas and did not turn to a specialist with these psychotraumas, did not get rid of them, suffer more often. People who experienced a lot, but mini-stress, that is, who had vigorous activity, who lived in constant stress, suffer less from Alzheimer's disease and other dementias.
Reflective people (who reflect on their inherent neurocognitive style) can use this. As in the example with borscht. If he has a spatial option, but he remembers well which ingredients to put. And she has the first option, she doesn’t remember it, but her frontal lobes are intact, that is, she remembers the procedure: first you need to pass, then lay out, and so on. And now they cook borscht together, because they understand that it is impossible to cook it not together. That is, they really bring freshness to their relationship, because they go to a new level. They form a joint activity, which was not.