Baby refusing feeds
Feeding Aversion - Why your baby is refusing bottles, breast or solids – Baby Care Advice
When we imagine what it should look like to feed a baby, we picture a scene of a hungry baby, gently cradled in our arms, who serenely gazes towards us as he contently feeds, peacefully stopping when satisfied. This is in stark contrast to the way in which babies who develop an aversion to feeding or eating behave. The scene is one of a screaming, hungry baby who acts like you're trying to poison him when you offer him a bottle of milk, breastfeed, or solid foods.
What is a feeding aversion?An aversion is the avoidance of a thing or situation because it is psychologically linked with an unpleasant, stressful, frightening, or painful experience. Basically, it’s fear that is displayed in anticipation of something bad happening again. A ‘feeding phobia’ and ‘feeding strike’ are other terms that may be used to describe a feeding aversion.
A feeding aversion refers to a situation where a physically well baby, repeatedly exhibits partial or full feeding refusal despite obvious hunger. A feeding-averse baby has a history that demonstrates he’s capable of feeding but for reasons yet to be identified and corrected, he refuses to feed or eats very little.
Babies as young as 7 weeks of age can develop an aversion to breastfeeding or bottle-feeding. Older babies can become averse to eating solids. Not just certain foods but the experience of eating solids. A baby could become averse to one, two, or all three feeding methods.
Feeding aversion signs and symptoms:A baby might display one or more of the following behaviors:
- Skips feedings or meals without distress.
- Appears hungry but refuses to eat.
- Fusses or cries when a bib is placed around his neck, or when placed into a feeding position, or when the bottle is offered or shown.
- Clamps his mouth shut or cries and turns his head away from the breast, bottle, spoon, or food.
- Takes a few sips or a small portion of the milk or food offered but then pulls away or arches back in a tense manner or cries.
 (NOTE: Babies back arch to distance themselves. Back arching does not provide evidence of acid reflux.)
(NOTE: Babies back arch to distance themselves. Back arching does not provide evidence of acid reflux.) - Feeds only while drowsy or asleep.
- Consumes less milk or food than expected.
- Refuses milk but eats solids.
- Displays poor or slow growth. May be diagnosed as 'failure to thrive'.
The type and intensity of behavior vary between babies. At one end of the spectrum, a baby might simply refuse to eat a particular food owing to a bad experience while eating that food. At the other end, a baby might display almost complete food refusal, eating very little, and require a feeding tube to ensure that he receives sufficient nourishment for healthy growth.
Feeding is not something that a baby can avoid entirely. A feeding-averse baby will reluctantly eat enough to survive but not voluntarily eat enough to thrive. Once averse to feeding a baby will try to ignore his hunger cues for as long as possible. Only willingly, but cautiously, eating when ravenous. Then eating quickly in fear of a repeat occurrence of whatever it is causing his fears. Eating just enough to soothe pangs of hunger, but not enough to feel completely satisfied.
Then eating quickly in fear of a repeat occurrence of whatever it is causing his fears. Eating just enough to soothe pangs of hunger, but not enough to feel completely satisfied.
A few behaviors displayed by some, but not all, feeding-averse babies require special mention due to the confusion they cause. These include:
- Conflicted feeding behavior
- Sleep-feeding
- Accepts water from a bottle
Many feeding-averse babies display conflicted feeding behavior - where the baby takes a few sucks, sharply turns away or arches back in a tense manner, possibly cries, quickly returns and wants to suck again, takes a few sucks, turns away or arches back, cries, and returns to feeding and so on. This disjointed feeding behavior is often interpreted by parents and others as an indication that the baby is experiencing pain, especially if he is intermittently crying, but it’s not necessarily due to pain. Babies who have become averse to feeding will behave in this tense or distressed manner regardless of the cause.
Feeding-averse babies often feed better or well when drowsy or during light sleep. When drowsy or asleep, a baby is not fully aware that he is being fed, and therefore he’s not on edge in anticipation of whatever it is that is causing him to fear feeding. In a drowsy or sleepy state, a hungry baby’s guard is down, instincts kick in, and he feeds well. A feeding-averse baby may refuse and fight feedings while awake but could complete a full feed without resistance when drowsy or asleep. (See other reasons for sleep-feeding.)
Accepting water from a bottleA small percentage of feeding-averse babies willingly accept water from a bottle but not milk. This causes parents to believe it’s the taste of the milk that baby objects to, which could be the case, but not necessarily so. It can be because the baby associates the taste of the milk with an unpleasant or stressful experience, for example, being pressured to feed.
Parents often pressure their baby to drink milk from a bottle but seldom pressure their baby to take water from the bottle. Babies are smarter than we give them credit for. They learn to link the taste of the milk with being pressured and therefore react as soon as they taste the milk.
Why babies become averse to feedingA baby could develop an aversion to feeding if an event occurring directly before, after, or while he is feeding triggers negative emotional responses, such as stress, pain, fear, or disgust. Several scenarios could potentially trigger such emotions. For example:
StressIf a baby is pressured or forced to feed against his will, this makes for an annoying, frustrating, or stressful experience depending on the feeding strategies parents employ, and how long they persist.
Being repeatedly pressured to feed against their will is without exception THE most common reason for babies to develop an aversion to feeding and then not want to eat. In most cases, it's the original and only cause of a baby's feeding aversion. However, in around 10 percent of cases, it's a secondary cause that develops after the baby's initial feeding refusal due to one or more of the reasons that follow.
In most cases, it's the original and only cause of a baby's feeding aversion. However, in around 10 percent of cases, it's a secondary cause that develops after the baby's initial feeding refusal due to one or more of the reasons that follow.
Sucking could be painful if a baby has mouth ulcers, and swallowing could be painful if a baby is suffering from esophagitis caused by acid reflux, or milk protein allergy. Chronic constipation or gastroparesis (delayed emptying of the stomach) could also cause a baby to associate eating with discomfort.
When a baby refuses to feed due to discomfort or pain, the parent might then pressure their baby by employing subtle or obvious forms of pressure to make him eat. This adds to the baby’s distress. The baby now has two reasons to want to avoid feeding – pain and the stress associated with being pressured to eat. It’s often the stress associated with being repeatedly pressured to feed that continues to reinforce the baby’s avoidant feeding behavior long after medications or dietary changes have removed pain from the feeding experience.
Medical procedures involving the baby's face or mouth, like nasal or oral suctioning, insertion of an NG (nasogastric) feeding tube, or intubation can be frightening, painful, and stressful.
Aspirating fluids or choking on solids would make for a frightening experience. A baby could aspirate owing to dysphagia (an uncoordinated sucking-swallowing pattern) or due to moderate or severe laryngomalacia (floppy vocal cords), or because the flow rate from the nipple of a bottle or breast is too fast, or due to poor head or bottle positioning negatively impacting on the baby’s latch, suction, and sucking and swallowing coordination, or when the parent persists in trying to make their baby eat while he is crying in distress.
Disgust at taste of milk or medicinesBeing forced to take foul-tasting medicines or milk (which can be the case for hypoallergenic formula or if a mother produces high levels of lipase in her breastmilk) could cause the baby to develop an aversion to feeding. If medications are added into a baby’s milk bottle, which then changes the flavor of the milk, or if given via a nipple-like device this could cause a baby to reject bottle-feeds. Parents often resort to pressure or force to get their baby to swallow something that tastes unpleasant, adding another reason for the baby to want to avoid feeding, or anything else the parent might try to place into his mouth.
If medications are added into a baby’s milk bottle, which then changes the flavor of the milk, or if given via a nipple-like device this could cause a baby to reject bottle-feeds. Parents often resort to pressure or force to get their baby to swallow something that tastes unpleasant, adding another reason for the baby to want to avoid feeding, or anything else the parent might try to place into his mouth.
Babies affected by a sensory processing disorder may find the sensation of the nipple, or anything else in their mouth, to be abhorrent. They can display aversive behavior to lumps in food or the smell, taste, or feel of certain foods.
The cause of an infant feeding problem could be due to one or a combination of different causes. A feeding aversion can become even more complex when other feeding problems are involved. (See bottle-feeding problems.)
Other reasons for why your baby won't take a bottle, breast or solidsThere are several other possible reasons for individual babies to display aversive behavior towards breastfeeding, bottle-feeding, or eating solid foods. Any situation that results in a baby becoming frightened, stressed or experience pain while feeding has the potential to trigger partial or complete food refusal.
Any situation that results in a baby becoming frightened, stressed or experience pain while feeding has the potential to trigger partial or complete food refusal.
A single occurrence of one of these events doesn't usually trigger an aversion, but it is possible, especially if the experience is traumatic for the baby. It would generally take repeated occurrences while feeding to cause a baby to become averse to feeding. When such episodes are repeated, the baby learns to link the sequence of events and expect a similar occurrence each time he feeds. And so, he tries to avoid feeding to avoid the situation that has caused him fright, stress, or pain in the past. It's at this stage he will react before the event because he knows what's going to happen. And so, he may become distressed as soon as he recognizes he is about to be offered a feed. Or even if he thinks he is about to be fed because of the position he is held.
Is pain the cause for your baby's feeding refusal?The distress displayed by many feeding-averse babies can be so intense that it appears like they are suffering from pain. Therefore, pain is typically the first thing blamed by parents, and by health professionals during brief consultations, when other causes for a baby's feeding refusal are not obvious. However, pain is not the only reason for babies to become distressed during feeds.
Therefore, pain is typically the first thing blamed by parents, and by health professionals during brief consultations, when other causes for a baby's feeding refusal are not obvious. However, pain is not the only reason for babies to become distressed during feeds.
So how can you tell if pain is the cause of your baby’s troubled feeding behavior?Check how he behaves at times outside of feeding as this will provide clues. For example:
- If your baby is happy once you stop trying to feed him, pain is unlikely. Pain fades away. It doesn't suddenly cease because the feed has ended.
- If your baby is content between feeds, pain is unlikely. Discomfort associated with acid reflux or milk protein allergy or intolerance, constipation or gastroparesis is not restricted to feeding times only. Your baby would display signs of discomfort or distress at other times in addition to feeding times.
- If your baby predictably feeds well in certain situations, for example during the night or while drowsy or asleep, pain is unlikely to be the cause of his oppositional feeding behavior.
 Sleep does not numb a baby to the sensation of pain. If it is painful for him to feed during the day or while awake, it’s reasonable to expect it would also be painful for him to feed at night or when sleep-feeding.
Sleep does not numb a baby to the sensation of pain. If it is painful for him to feed during the day or while awake, it’s reasonable to expect it would also be painful for him to feed at night or when sleep-feeding.
NOTE: If your baby displays any unusual signs that might indicate illness or a physical problem, or if you are worried that your baby is suffering from pain, have him examined by a doctor.
Conflicted feeding behavior where baby takes a few sucks, sharply turns away or arches back, cries, quickly returns and wants to suck again, takes a few sucks, turns away or arches back, cries, returns to feeding and so on, is often interpreted by parents and others as pain, but its not necessarily due to pain. Babies who have become averse to feeding will behave in this way regardless of the cause. If your baby is quickly soothed once the feed has ended, it's probably not pain.
Is pressure the cause of your baby's feeding refusal?Some parents will pressure or force their baby to feed out of loving concern for their baby’s physical wellbeing. They hate doing this but do so because they worry that their baby will fail to gain sufficient weight or become unwell if they don’t make sure he consumes what they believe, or have been told, is an acceptable amount of milk or food.
They hate doing this but do so because they worry that their baby will fail to gain sufficient weight or become unwell if they don’t make sure he consumes what they believe, or have been told, is an acceptable amount of milk or food.
Many of the feeding strategies that we believe are ‘encouraging’ or ‘supporting’ a baby to eat involve subtle forms of pressure. For example:
- Pushing the nipple into a baby’s mouth against his wishes.
- Preventing him from pushing the nipple out of his mouth with his tongue.
- Following his head with the bottle when he turns or arches back in tense manner.
- Restraining his head to prevent him from turning away.
- Restraining his arms to prevent him from pushing the bottle away.
- Offering repeatedly at a time when he's rejecting or upset.
- Upwards pressure under his chin in a bid to trigger his sucking reflex.
- Gently compressing his cheeks to apply pressure on his buccal pads (cheek pads).

- Jiggling or twisting the bottle to try and make him continue sucking.
- Squeezing milk into his mouth.
- Trying to trick him into accepting the nipple by switching his pacifier for the nipple.
If these things don’t upset your baby - which generally appears to be the case for babies under the age of eight weeks who due to immaturity have limited ability to complain during the feed but can after the feed – such strategies might be causing no harm. However, doing these things in a bid to control how much a baby eats has the potential to make the experience of feeding unpleasant or stressful for the baby. When repeated, a baby can develop an aversion to feeding.
As a result of developing a feeding aversion the baby will fuss or refuse to feed and the parents, not knowing any better, may then feel compelled to force their baby to eat, and by doing so they may be unknowingly reinforcing their baby’s feeding aversion.
Behavior that is reinforced will continue. Once averse to feeding, the situation spirals downwards as a result of the ‘fear-avoidance-cycle’.
Once averse to feeding, the situation spirals downwards as a result of the ‘fear-avoidance-cycle’.
The more the parent pressures their baby, the less their baby is willing to eat. The less their baby eats, the more the parent pressures. And around and around it goes. The 'fear-avoidance-cycle' can spiral downwards to complete feeding refusal while awake, poor growth, and possible hospitalization where a feeding tube might be inserted.
Direct and indirect reinforcementsAny pressure, even subtle forms, has the potential to directly reinforce a feeding aversion. However, there are other strategies, for example feeding a baby while sleeping, giving solids to compensate for the loss of calories from milk, providing milk in other ways such as spoon, syringe, or feeding tube, can indirectly reinforce a behavioral feeding aversion by enabling the baby to avoid feeding while awake during the day. All reinforcements – direct and indirect – need to be removed.
Medical treatments
A feeding-averse baby is often distressed at feeding times (an exception being those who mostly sleep-feed during naps and at night). Pain is typically the first thing blamed, but the least likely cause of aversive feeding behavior displayed by physically well, thriving babies.
If you go to the doctor with a fussy baby who cries and refuses to eat, he or she may tend to explore physical causes before all others. The following treatments are often recommended by medical practitioners in a bid to remedy a baby's fussy or distressed feeding behavior.
Medications: Acid suppressing medications may be prescribed to treat suspected esophagitis - inflammation of the baby’s feeding tube caused by repeated exposure to refluxed stomach acid. And perhaps prokinetic medication (also called propulsive agents) to treat gastroparesis - delayed emptying of the stomach.
Dietary changes: A hypoallergenic infant formula may be recommended to treat suspected eosinophilic esophagitis - inflammation caused by an allergic reaction to cow’s milk based infant formula or soy infant formula.
Once the condition causing the baby's discomfort is effectively treated, his troubled feeding behavior will fade and disappear.
NOTE: A doctor cannot see into a baby’s esophagus and therefore cannot confirm if he is suffering from esophagitis during a routine medical examination. h3 antagonists and proton pump inhibitors used in the treatment of acid reflux are extremely effective in reducing the production of stomach acid. If your baby is still fussing or fighting feeds two weeks after commencing medications, there's a good chance that acid reflux is not responsible for his troubled feeding behavior. Similarly, if your baby's avoidant feeding behavior continues two weeks after switching to a specialized hypoallergenic formula, the reason may be that milk protein allergy is not the cause. This does not imply that your baby is not affected by these conditions, rather that these conditions are unlikely to be the cause of his avoidant feeding behavior.
This does not imply that your baby is not affected by these conditions, rather that these conditions are unlikely to be the cause of his avoidant feeding behavior.
Band-Aid solutions: If medications and dietary change fail to resolve a baby's aversive feeding behavior, band-aid solutions such as high-calorie feeds, food thickeners, starting solids, sleep-feeding, might be recommended in an attempt to minimize the risk of poor growth caused by an unresolved feeding aversion. However, band-aid solutions are often ineffective in the case of a feeding aversion because they do not address the cause, which is the stimulus that is causing the baby to fear feeding.
If medical treatments fail to resolve your baby's feeding issues, consider the possibility of a misdiagnosis or that there is more than one cause involved. And extend your search to cover other potential causes, in particular behavioral reasons such as being pressured to eat.
Speech therapyIf your baby often chokes or experiences problems with aspiration while feeding, his doctor might refer him to a speech therapist to assess his ability to suck and swallow effectively. This can be helpful if choking episodes are reinforcing the baby's aversive behavior.
This can be helpful if choking episodes are reinforcing the baby's aversive behavior.
However, if your baby feeds well at some feeds for example in a sleepy state or has fed well in the past before developing a feeding aversion, it's unlikely that the source of his fussy feeding behavior or food refusal is due to a sucking or swallowing problem.
Occupational therapyIf an oral aversion due to a sensory processing disorder is suspected, your doctor might refer your baby to an occupational therapist for an assessment. Encouraging a child with oral aversion occurring due to a sensory processing disorder to feed as normally as possible requires a very long process that may last months or years.
An oral aversion is wide ranging with the baby not wanting anything near his mouth. A feeding aversion is specific, related to feeding, and requires very different treatment to resolve the problem compared to an oral aversion
NOTE: Some of the feeding strategies recommended to resolve an oral aversion, such as placing rubbery implements into the baby’s mouth to ‘desensitize’ him to the feel of things in his mouth, are counterproductive in the case of a behavioral feeding aversion that developed or is currently reinforced as a result of being pressured to feed. Placing things into a baby’s mouth without his permission will not regain his trust. Hence, the diagnosis must be correct. If your baby is happy to have anything other than the nipple of a bottle or food in his mouth, it’s probably a feeding aversion rather than an oral aversion.
Placing things into a baby’s mouth without his permission will not regain his trust. Hence, the diagnosis must be correct. If your baby is happy to have anything other than the nipple of a bottle or food in his mouth, it’s probably a feeding aversion rather than an oral aversion.
A behavioral approach views challenging infant behaviors such as incessant crying, fussy feeding behavior, feeding refusal, and sleeping problems in the context of the care the baby receives. In the case of physically well babies, it’s not assumed that the baby has a physical problem, rather the parent’s childcare practices are examined.
Infant behavior, whether this is desirable or undesirable behavior, is reinforced by the actions parents take or don’t take. To resolve a behavioral problem, and thus change a healthy baby’s behavior from fussy, distressed feeding refusal to enjoying feeding to satisfaction, it’s necessary for the parent to first make appropriate changes to their childcare practices.
The parent’s infant feeding practices are the last suspected cause of a healthy baby's aversive feeding behavior when it should be one of the first. You will know how thoroughly your baby’s healthcare professionals have assessed the possibility of behavioral reasons for his feeding issues by the number of questions asked of you regarding his feeding history. For example, feeding equipment, feeding frequency and duration, milk type, and concentration, feeding pattern, total daily milk intake, his sleeping patterns (sleep has a profound effect on feeding behavior and milk intake) and most important of all, your infant feeding and sleep settling practices. Our Baby Care Advice questionnaire includes 80+ questions to pinpoint the cause.
No questions asked = minimal to no consideration given to behavioral causes.
MisdiagnosisAccurate identification of the cause is essential to finding an effective solution. This is not something that can be achieved during a brief consultation with a health professional. And it definitely cannot be achieved without asking the parents multiple questions about their infant feeding practices. An accurate, and thorough diagnosis of the cause, or causes as is often the case, requires a comprehensive understanding of infant development and behavior, and age-appropriate infant feeding practices, as well as an understanding of the reasons and solutions to infant feeding aversion. At Baby Care Advice we allocate 2 hours for feeding problems.
And it definitely cannot be achieved without asking the parents multiple questions about their infant feeding practices. An accurate, and thorough diagnosis of the cause, or causes as is often the case, requires a comprehensive understanding of infant development and behavior, and age-appropriate infant feeding practices, as well as an understanding of the reasons and solutions to infant feeding aversion. At Baby Care Advice we allocate 2 hours for feeding problems.
Misdiagnosis occurs when assumptions are made about the cause in the absence of a comprehensive feeding assessment. Failure to accurately identify the stimulus causing and reinforcing the baby's feeding aversion - which can vary for individual babies - is likely to result in an ineffective treatment plan.
Not only will a misdiagnosis fail to address the cause, but many of the strategies recommended based on a misdiagnosis, such as those described as indirect reinforcements, have the potential to reinforce a baby’s aversive feeding behavior. A baby’s feeding aversion will continue while it’s reinforced. An unresolved breast- or bottle-feeding aversion increases the risk of the baby developing an aversion to eating solids for the same reasons. Feeding issues can persist for weeks, months or years.
A baby’s feeding aversion will continue while it’s reinforced. An unresolved breast- or bottle-feeding aversion increases the risk of the baby developing an aversion to eating solids for the same reasons. Feeding issues can persist for weeks, months or years.
Few health professionals are familiar with age-appropriate infant feeding practices and/or the process involved in resolving behavioral feeding aversions experienced by normal developing babies and young children. Therefore, they are ill-equipped to guide and support parents to resolve this complex and highly stressful situation.
A baby's avoidant feeding behavior, poor milk intake, and poor growth could be due to one or a combination of the causes already mentioned. However, a feeding aversion can become even more complex if other feeding issues are involved. For example, unsuitable or faulty equipment, poor feeding position, or the parent’s providing an inappropriate response to their baby’s feeding cues. (See bottle-feeding problems for more.)
(See bottle-feeding problems for more.)
If you suspect that your baby has developed a feeding aversion, there are a couple of ways we can help.
You might choose to see if you can figure things out on your own as a result of being guided by my book 'Your Baby’s Bottle-feeding Aversion’.
You might prefer to have one of our experienced consultants undertake a comprehensive assessment of all causes and provide individualized feeding advice. You also have the option to receive daily email guidance and support as you work towards resolving your baby’s feeding aversion.
You can purchase Rowena's Online Bottle-Feeding Aversion Program - six modules with clear step by step instructions on how to overcome your baby's bottle-feeding aversion. With a 95% success rate using Rowena's Bennett's method.
‘Your Baby's Bottle-Feeding Aversion’ bookIn my book, ‘Your baby’s Bottle-feeding Aversion’, I have described physical and behavioral reasons for babies to develop an aversion to bottle-feeding. How to identify the cause and the solutions to match. Included are step-by-step instructions on how to regain your baby’s trust and resolve a feeding aversion caused or reinforced by repeated pressure to feed.
How to identify the cause and the solutions to match. Included are step-by-step instructions on how to regain your baby’s trust and resolve a feeding aversion caused or reinforced by repeated pressure to feed.
While the book was written for bottle-fed babies, many nursing mothers have found that applying the same strategies has also helped them to successfully resolve a breastfeeding aversion.
You might find that reading this book is all you need to do to understand the steps you need to take to resolve your baby’s feeding aversion and get him back to the point of enjoying eating until satisfied.
Baby Care Advice ConsultationsIf you would like an individualized assessment of all reasons for infant feeding problems, not just feeding aversion, we also provide a consultation service. Baby Care Advice consultants have extensive experience in pinpointing the cause of feeding aversion and other behavioral feeding problems such as those related to equipment and the parent’s feeding practices. (For more on what’s included in a consultation).
(For more on what’s included in a consultation).
Six time-saving modules to help your family enjoy feeding again with Rowena's step-by-step plan. Enjoy additional tools to manage anxiety, troubleshoot any issues, introduce new carers, how to manage illness/teething and much more.
Join Our Facebook Support CommunityBaby Care Advice has facebook support groups in various languages, for those who have purchased either Rowena's 'Your Baby's Bottle-Feeding Aversion' book/ Online program/ consultation. They are made possible by a volunteer group of parents, who offer empathetic, compassionate support and guidance as you work your way through resolving your baby's feeding aversion.
English
Spanish
Dutch
Romanian
By Rowena Bennett, RN, RM, CHN, MHN, IBCLC.
Written Sept 2013. Revised July 2021.
Copyright www. babycareadvice.com 2021. All rights reserved. Permission from the author must be obtained to reproduce all or any part of this article.
babycareadvice.com 2021. All rights reserved. Permission from the author must be obtained to reproduce all or any part of this article.
Baby Refusing the Bottle? Try These Tips
If you’re having trouble bottle-feeding your infant, rest assured that you are far from alone. Around 25 percent of parents report feeding-related problems with their child at some point in their development.
If your baby has been breastfeeding, trying to introduce a bottle can also introduce some challenges. Likewise, changes to the formula or breast milk you’re giving them or the bottle you’re using can lead to difficulties even for experienced bottle-fed babies.
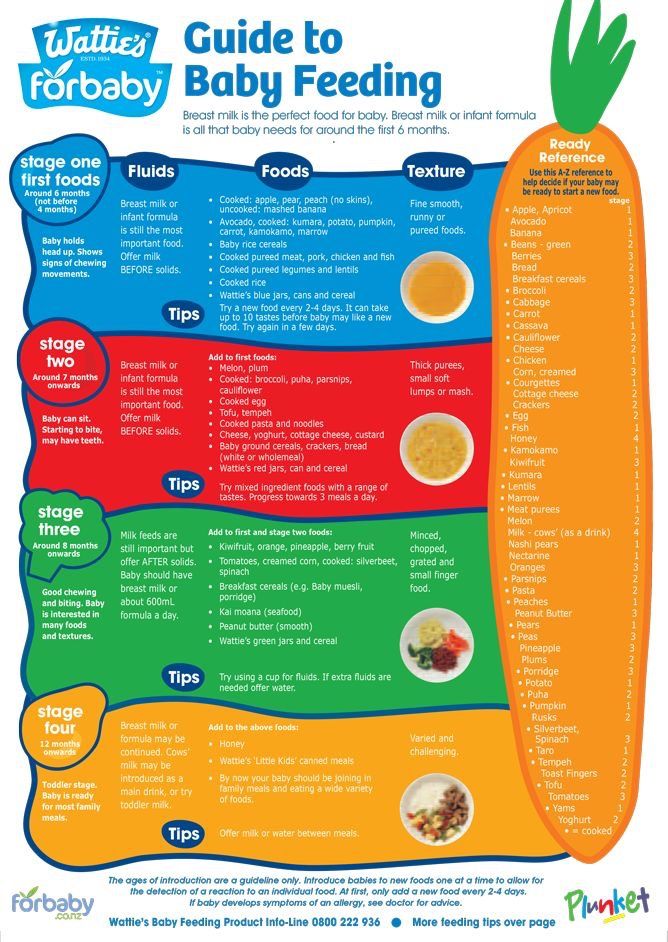
The American Academy of Pediatrics recommends delaying the introduction of foods other than breast milk until your baby is around 6 months old, suggesting exclusive breastfeeding before that time. However that’s not always realistic and you may find yourself introducing the bottle at any time during the first year.
Additionally, formula isn’t the only reason to use a bottle. Many breastfeeding parents want to incorporate bottle-feeding of breast milk for flexibility. The breastfeeding advocacy organization La Leche League suggests waiting until your breastfeeding baby is 3 to 4 weeks old before introducing a bottle.
Many breastfeeding parents want to incorporate bottle-feeding of breast milk for flexibility. The breastfeeding advocacy organization La Leche League suggests waiting until your breastfeeding baby is 3 to 4 weeks old before introducing a bottle.
Whenever you begin using bottles, it can be extremely frustrating trying to feed a baby who stubbornly refuses feeds. But with dedication, experimentation, patience, and love, you can eventually acclimate your baby to bottle-feeding.
Since babies can’t communicate clearly, parents and caregivers are left wondering and guessing why their baby refuses bottle-feeding. The following reasons are some of the most common things to look out for if your baby refuses the bottle:
- Your baby was recently weaned and wants to continue breastfeeding.
- Your baby isn’t hungry enough to want feeding.
- Your baby is feeling sick, colicky, or otherwise unwell enough to feed.
- Your baby is being held in an uncomfortable position.
- Your baby doesn’t like the temperature, flavor, or texture of the milk.
- Your baby doesn’t like the texture or feel of the bottle.
Depending on your previous experience with feeding you may be able to figure out the specific reasons why they’re refusing the bottle. Many times, knowing why they refuse can give you better insight into figuring out how to fix the problem.
Some of the most common and effective things you can try to help your baby accept bottle-feeding include:
- Slowly, consistently, and gradually transition from breastfeeding to bottle-feeding.
- Wait until your baby is sufficiently hungry before feeding.
- Try changing the bottle size and shape, the nipple, or other aspects of the bottle to see what your baby responds to.
- Experiment with the temperature of the milk or formula. Breast milk is lukewarm, so make sure the bottle isn’t too warm or cool.
- If your baby is teething, try changing the temperature of the milk (teething babies sometimes prefer cold milk), massaging their gums, or otherwise helping them with the pain of new teeth poking through.

- Hold your baby in a different feeding position and see what they respond to.
- Allow someone else to handle the feeding. This can be especially helpful during a transition from breastfeeding to bottle-feeding.
Before changing the formula you’re using you may want to talk to your pediatrician. There are different types of formula customized to different needs, but too many changes or certain types of formula can cause other challenges.
More tips to try
In addition to the list of possible remedies above, it is important to try to have a calm and consistent approach to bottle-feeding. Sometimes, your own frustrations with bottle-feeding can affect the infant and make it even harder for them to change.
In general, try to follow these behavioral tips for yourself when bottle-feeding a fussy baby:
- Maintain a comforting routine around mealtime.
- Avoid distractions, such as media, music, and toys when bottle-feeding.
- Feed your child at consistent time intervals of 3 to 4 hours.

- Stay calm and consistent. Don’t become angry, anxious, or overly excited with your feeding child.
- Limit mealtimes to 30 minutes.
- Try to avoid frustration during feeds. Consider having another caregiver offer the bottle if you need a break.
While it is normal for babies to sometimes refuse a bottle, there are some instances where chronic refusal to feed can be indicative of an eating disorder or an illness that requires medical attention.
About 1 to 5 percent of very young children have feeding disorder, which is characterized by an inability to consume an adequate amount of food, resulting in malnutrition.
Getting enough food is absolutely essential for a growing baby. If you think your baby is experiencing a feeding disorder making it difficult for them to gain weight, you should see a doctor immediately. Feeding disorders in early childhood are an important health issue.
In the short term, babies with feeding disorders will experience nutritional deficiency and weight loss (or inadequate weight gain), but in the long term, your baby can experience growth deficits, cognitive functioning problems, stunted neurodevelopment, and behavioral or emotional impairment.
Another time to talk to your baby’s doctor is if your baby refuses to eat due to an illness or pain. Call your doctor right away if in addition to refusing the bottle your baby is showing any of the following symptoms:
- fever
- vomiting
- constant crying
- diarrhea
- difficulty breathing
Consult with a doctor to determine whether there are any illnesses or physiological issues you are unaware of that might play a part in your child’s fussy eating.
Feeding difficulties are common problems in infants and toddlers. Don’t be too worried if your baby is struggling with the transition to bottle-feeding.
There are many different approaches you can take to fixing the problem, and if you are nervous or worried about any of your child’s eating habits, contact your doctor immediately.
With consistency, determination, and lots of attention paid to your baby, you can help them overcome their obstacles and anxieties around bottle-feeding.
8 reasons why a child refuses to eat
Our life is impossible without food. From birth, a child has an instinct for eating. And with age, he does not cease to understand whether he wants to eat or not. Therefore, forcing a child to eat on the part of the parents is wrong. If the child grows and develops normally, then let him eat what he wants and how much he wants. Forcing the baby to eat, you can easily break his natural sense of proportion, and then fight overeating and being overweight. All children are different and it is important to give the child the amount of food that will satisfy his needs. And these needs depend on various factors. If the little one refuses to eat, try to understand the reason for this behavior. nine0003
1. The child is not hungry. Even if a long time has passed since the last meal, it is possible that the child is still full. Parents should take into account the calorie content of food and the energy consumption of the child. If the meal was high in calories, but after that the child watched cartoons and did not run in the yard, then he may not want to eat for a long time. Physical activity encourages the body to expend energy and the child will get hungry faster.
If the meal was high in calories, but after that the child watched cartoons and did not run in the yard, then he may not want to eat for a long time. Physical activity encourages the body to expend energy and the child will get hungry faster.
2. The child does not have a daily routine. It is advisable to feed the baby at about the same time. The optimal portion for a child is two of his palms folded together. In addition, it is necessary that the child every day spend time in the fresh air and go to bed on time. If the child has little active pastime, then do not be surprised that he does not eat well. nine0007 3. The child is ill. Lack of appetite may be a symptom of some disease. Many children begin to eat badly when they are teething. Often the child refuses food when he has a fever. Before forcing a child to finish eating porridge, make sure that he is healthy.
4. The child "interrupts" the appetite. Sometimes snacking can cause a child to eat poorly at lunch or dinner. Do not give any cookies or sweets if you plan to sit down at the table soon. nine0007 5. The child does not like a particular dish. The baby may not refuse food in general, but simply milk porridge or borscht. Everyone has their preferences and kids have them too. Consider your child's preferences when planning menus. Accustom the little one to new tastes gradually, in the same way as complementary foods were introduced. Children are reluctant to perceive new tastes, but if given often and a little bit, they get used to it.
Do not give any cookies or sweets if you plan to sit down at the table soon. nine0007 5. The child does not like a particular dish. The baby may not refuse food in general, but simply milk porridge or borscht. Everyone has their preferences and kids have them too. Consider your child's preferences when planning menus. Accustom the little one to new tastes gradually, in the same way as complementary foods were introduced. Children are reluctant to perceive new tastes, but if given often and a little bit, they get used to it.
6. The child has psychological problems. Children subtly feel the psychological situation in the family. Refusal to eat may be associated with a desire to attract the attention of parents to their person. nine0007 7. The child developed an eating neurosis. If parents force the child to eat regularly, without taking into account his desire, then the baby may develop food neurosis. Such children begin to cry at the sight of a plate, they can run away to another room and become hysterical.
8. All children are different. Do not compare your child with other children. All have their own physical characteristics. If the baby eats little, just make these small portions as healthy and nutritious as possible, but do not force him to eat more than he wants. nine0003
Do not treat the refusal of food as disobedience and whims. Try to understand what the problem is and solve it. Think and analyze your behavior, did you do everything as it should? If you realize what you did wrong, then try to quickly correct your mistakes. Use methods such as fairy tale therapy. Before going to bed, the child will listen with pleasure about his favorite fairy-tale hero, who ate well, so he was strong and courageous. Try to interest the child in the beautiful design of the dish. Ordinary products can become a castle, a car, a cute face - there is room for parental imagination to roam. nine0003
If the child does not eat well: what to do and what not to do
What to do if the child does not want to eat.
- Malyusik, well, one more spoon - and that's it! Last! I ate only two, let's have a little more, here's the most delicious piece for you! - says the average mother, offering a spoon with one hand, playing the accordion with the other, showing the trick with the disappearance of the handkerchief with the third, turning the cutlets over with the fourth, while doing somersaults on one leg.
Sound familiar?
Every dad has an instinct to bring home food, and mom has to feed the baby food. And if he refuses to eat, a signal is triggered - "I'm a bad mother" or "the child is sick."
In this case, the most important thing for a parent to understand is whether the child DOES NOT WANT or CANNOT eat?
If the baby is running around, having fun and looking good, without showing any signs of illness, then most likely he does not want to eat. There can be many reasons:
- A breastfeeding child prefers milk and dairy products, intuitively understanding that he needs calcium, and now milk is healthier for him than soup.
 nine0051
nine0051 - The child wants a cookie, not vegetables.
- He's really not hungry. For example, his metabolism is slow, breakfast has not yet been digested, and lunch is already being offered. Or the child was sitting in front of the TV after breakfast and his appetite had not yet had enough time to play out. Compared to the boy next door who was outside all day.
- If a child is not genetically destined to become Uncle Styopa, then he can eat much less than his peer, who has tall parents. nine0051
- Psychological problems. If earlier you accidentally gave your child a bitter cucumber, then he may refuse any green food. Or you yell at the child during the meal, and for him the food is perceived as a trauma.
If your child is lively, but at the same time he has a "bad appetite", then this is not his problem, but yours - the psychological problem of an unsatisfied instinct. If a child jumps, jumps, he has healthy nails, hair, etc., think less about what he lacks. Better think about something nice))
Better think about something nice))
An active child = not a hungry child.
Wait for the natural desire and correctly distribute energy costs - walk more often, send the child to the sports section, or simply say: “If you don’t want to, take a walk, dinner is not earlier than seven and no snacks.” That is, if your child simply does not want to eat, normalize feeding - strictly at a certain time and without snacks. The body will get used to secrete gastric juice strictly according to the schedule.
And one more thing. There are no rules about how much a child should eat. He can eat a kilo (and make you very happy) and 9Send 00 grams to the toilet. Or eat 100 g and learn everything.
But it is much more difficult if the child CANNOT eat.
Causes:
- If you are breastfeeding, you may have “tight breasts”, when it is very difficult for the baby to suck milk.
- A child has a runny nose, and when he eats, he begins to choke.
- Food hot, cold, sour, bitter.