Baby sticking tongue out when bottle feeding
Baby Tougue Thrush Causes, Symptoms & Treatments
If you’ve noticed your baby poking out their tongue when nursing or drinking from a bottle, you may be wondering whether you should be concerned. Thankfully, what you’re seeing is most likely a perfectly normal reflex called tongue thrust.
Let’s talk about what baby tongue thrust is, why it happens, and when it may be a sign of a problem.
What Is Baby Tongue Thrust?Your baby is born with a tongue thrust reflex to prevent them from choking. Also known as extrusion reflex, the reflex is stimulated when something touches baby’s lips. They respond by using the tongue to push it away or, in the case of feeding, to latch on to the nipple or bottle.
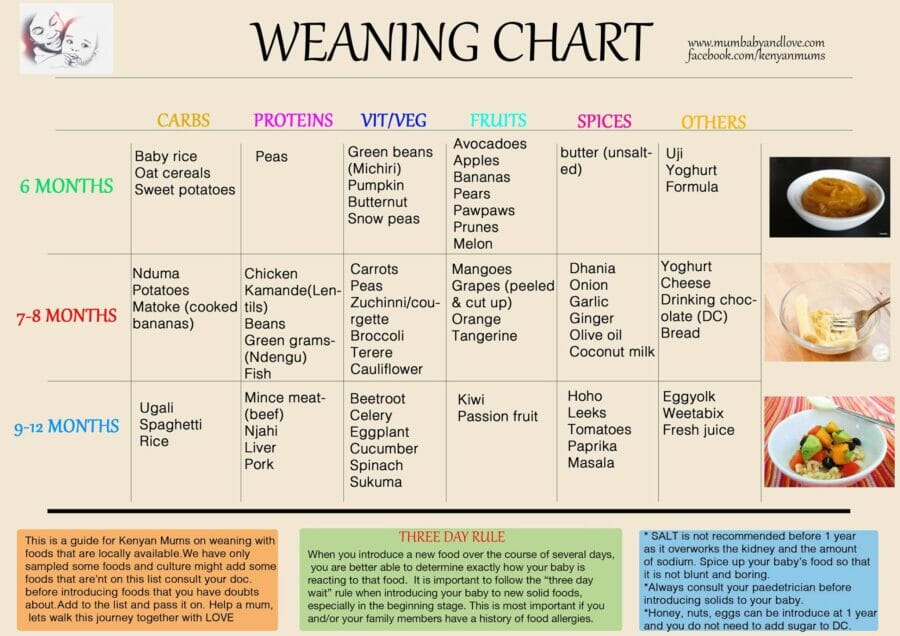
How Long Does Baby Tongue Thrust Last?The Australian Breastfeeding Association (ABA) says that most babies will grow out of tongue thrusting by around six months old. Around this age, the ABA says that you may notice baby showing an interest in your food, or reaching out to grab food and put it in their mouth.
This is a sign that your baby may be ready to start trying solid foods. You can test this by touching a spoon to the tip of their tongue. If the tongue doesn’t pop out to push the spoon away, then your baby’s tongue thrust reflex is subsiding and you can start to introduce solid food.
What If Tongue Thrust Doesn’t Go Away?All babies hit developmental milestones at different times, so if your baby’s tongue thrust reflex takes longer to subside, it’s usually nothing to worry about. However, if the reflex persists into childhood, it can potentially cause problems with speech and dental development.
The Effects of Tongue Thrust In ChildrenIn a normal swallowing pattern, Dental Health Service Victoria (DHSV) explains that the tongue is pushed up against the roof of the mouth. However, a child still displaying the tongue thrust reflex will push the tongue against the back of the front teeth instead, exerting enormous, sustained pressure. This can push the front teeth forward, creating an open bite and even altering the shape of your child’s face.
This can push the front teeth forward, creating an open bite and even altering the shape of your child’s face.
DHSV also warns that tongue thrust can interfere with a child’s ability to form certain words, particularly those with ‘s’ and ‘z’ sounds. This can lead to a lisp, which may need to be treated by a speech pathologist.
Signs Your Child Still Has Tongue ThrustIt’s not always obvious that your child has tongue thrust. DHSV advises looking out for:
- An open bite.
- A lisp or difficulty saying ‘s’ and ‘z’ sounds.
- Grimacing or pursing the lips when swallowing.
- An open mouth and/or visible tongue when resting.
- Breathing with an open mouth.
According to DHSV, most children will have outgrown the tongue thrust reflex by the age of six, with only three percent still displaying the behaviour at 12.
However, it’s perfectly natural to feel protective of your little one, and it’s always best to err on the safe side.
If you’re worried that your baby’s tongue-poking is a sign of something more serious, or you’re concerned about the effects of tongue thrust on your child’s dental health or speech, your doctor or dentist can offer you advice and reassurance.
Is My Baby Sticking His Tongue Out Normal?
Baby reflexes
Babies have a tendency to use their mouth in a variety of ways. If you notice your baby frequently sticking their tongue out, you may wonder whether this is a normal behavior. The short answer is yes; sticking the tongue out is typically a totally normal infant behavior.
Babies are born with a strong sucking reflex and instinct for feeding. Part of this reflex is the tongue-thrust reflex, in which babies stick their tongues out to prevent themselves from choking and to help latch on to the nipple.
Using their mouths is also the first way babies experience the world. It’s very common for them to mouth things and stick out their tongues, both as part of the feeding instinct and exploring the new world around them. Part of this behavior is your baby noticing the feel of his or her own lips.
Part of this behavior is your baby noticing the feel of his or her own lips.
If you find that your baby’s tongue is always sticking out of their mouth, or they seem to be constantly drooling — more than is normally associated with spit-up and teething — or they have difficulty swallowing, call your doctor.
That said, here are 10 causes, some common and some rare, for a baby to stick his or her tongue out.
1. They’re playing
There has been some debate since the 1970s about whether newborn babies imitate adult behavior.
Older babies certainly mimic, but several studies, including one in the Journal of Developmental Science, have reported that babies as young as a few weeks old imitate adult facial expressions, including sticking out their tongues.
2. It’s a habit
The tongue-thrust reflex that babies are born with includes sticking the tongue out. This helps facilitate breast or bottle feeding.
While this reflex typically disappears between 4 to 6 months of age, some babies continue to stick their tongues out from habit. They may also simply think it feels funny or interesting.
They may also simply think it feels funny or interesting.
3. They’re hungry or full
Crying is not the only way that babies communicate they are hungry. Crying is actually a late sign of hunger.
According to the Centers for Disease Control and Prevention (CDC), early signs of hunger may include clenched hands, putting hands in the mouth, turning toward the breast or bottle, and smacking or licking the lips. Sticking the tongue out may be part of a baby’s hunger cues.
Babies may also stick their tongues out when they are full. Other signs of fullness may include turning the head away, spitting out food or milk, and simply refusing to suck or eat.
4. They have a large tongue
If a baby has a larger than average tongue, a condition known as macroglossia, they may stick their tongue out more than usual.
Macroglossia may occur because of genetics, or abnormal blood vessel or muscle development in the tongue. It may also be caused by conditions such as hypothyroidism or tumors.
Macroglossia may occur as one symptom in syndromes such as Down syndrome and Beckwith-Wiedemann syndrome.
If your baby’s tongue does not seem to fit into their mouth, or you notice other concerns, such as excessive drooling, difficulty swallowing, poor muscle tone, or difficulty feeding, call your child’s pediatrician to discuss your concerns.
5. They have a small mouth
There are a number of syndromes or conditions that may cause a baby to have a smaller-than-average mouth. Sometimes babies are genetically predisposed to have a small mouth.
One such condition is micrognathia, or a small jaw. Micrognathia may be genetic or part of a syndrome or condition such as cleft lip or cleft palate, Beckwith-Wiedemann syndrome, Pierre Robin syndrome, and several others.
Children with Down syndrome may have a number of signs including smaller-than-average mouths, short stature, distinct facial features, and decreased muscle tone.
Babies with a condition called DiGeorge syndrome may also have small mouths due to changes in the shape of the palate. DiGeorge syndrome has a number of other symptoms, including heart defects and developmental delay.
DiGeorge syndrome has a number of other symptoms, including heart defects and developmental delay.
6. They have poor muscle tone
Some babies have decreased muscle tone. Since the tongue is a muscle, and is controlled by other muscles in the mouth, decreased muscle tone can cause the tongue to stick out more than usual.
Several conditions may cause decreased muscle tone, such as Down syndrome, DiGeorge syndrome, and cerebral palsy.
7. You’ve got a mouth breather
Babies typically breathe through their nose. If your baby has nasal congestion or large tonsils or adenoids, they may breathe through their mouth instead. This can cause the tongue to stick out.
If your baby seems to have difficulty breathing, flaring of the nostrils, wheezing, or other unusual breathing sounds, you should call your baby’s doctor immediately. If you have other ongoing concerns about your baby’s breathing or amount of congestion, call your baby’s doctor to help troubleshoot.
If your child has large tonsils or adenoids that are interfering with breathing or feeding, they may need to be surgically removed.
8. Gas
Some babies stick their tongues out when they are experiencing gas pains or passing gas. All babies pass gas as a normal part of digestion. Some babies react to the sensation more than others, and may cry, grimace, stick out their tongue, or even smile.
9. A mass in the mouth
Occasionally, babies may have a mass or swollen gland in their mouth, which can force the tongue to protrude.
Very rarely, this may be some type of oral cancer. More commonly, they may have an infection that causes a salivary gland cyst.
If your baby seems to stick out their tongue more than usual, drools excessively, is fussy with eating or refuses to eat, or you can feel or see a bump in their mouth, call your child’s doctor.
10. They’re not ready for solid food
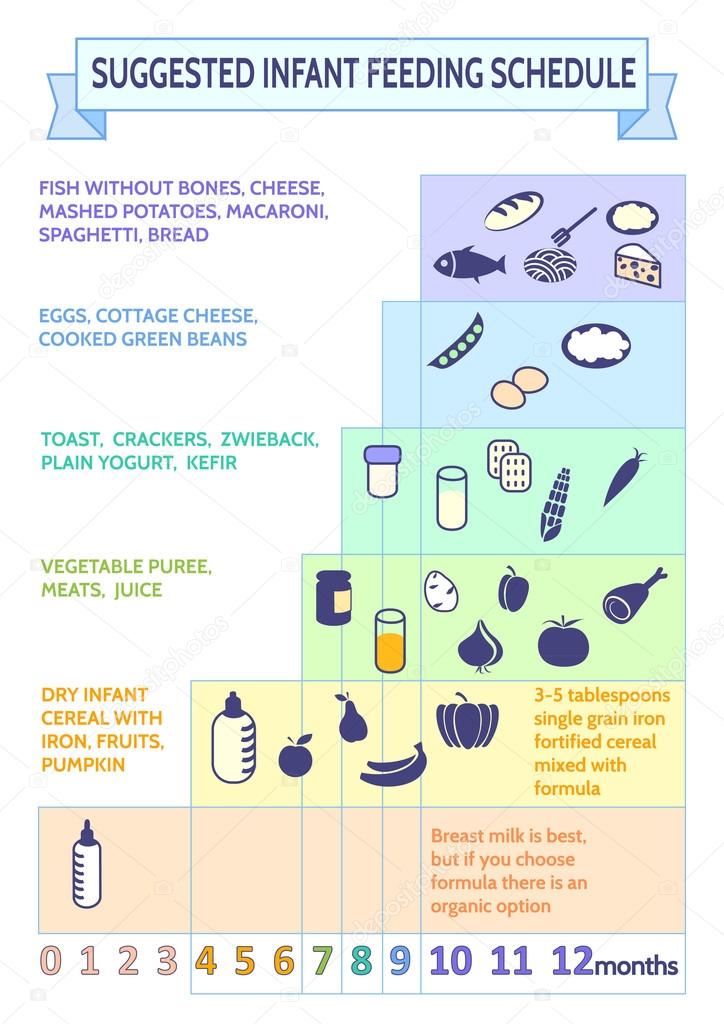
Babies receive most of their nutrition for the first year of life from breastmilk or infant formula. The CDC, and most pediatricians, recommend adding solid foods, starting with pureed baby food or cereal, around 6 months of age.
The CDC, and most pediatricians, recommend adding solid foods, starting with pureed baby food or cereal, around 6 months of age.
The amount of solid food a baby eats gradually increases, until the age of 1 year, when most of their nutrients come from solid foods rather than milk alone.
Some babies take readily to solids, while others dislike the taste or textures and may take longer to become accustomed. If a baby is not ready for solid foods, they may stick their tongue out to push the food away or get it out of their mouths. They may not yet have the oral coordination necessary to eat solids.
If your baby is sticking their tongue out persistently when you try solid foods, perhaps stop and try again in a week or two. If you have concerns about your baby’s eating, speak with your baby’s doctor.
Takeaway
Babies stick their tongues out for a number of reasons. Most of the time, this is completely developmentally normal. Occasionally, a baby who sticks their tongue out more than usual may have an underlying reason.
If you are concerned about your baby sticking their tongue out or other accompanying symptoms, it may be helpful to speak to your baby’s doctor.
Understanding tongue movement in infants
2 min.
Sept. 2021
This resource is for healthcare professionals
Researchers have used video recording for the first time to see differences in tongue movements between breastfed infants and adults when swallowing.
The tongue is an active muscle and a miracle of coordination. When we drink, the tongue prepares for swallowing by collecting liquid in the mouth, taking the shape of a bowl. It then quickly pushes the liquid back where it is swallowed, while still allowing us to continue breathing.
When we eat, the tongue works by holding the food in the mouth, moving it with saliva and turning it into a lump, which is then pushed back for swallowing. Both adults and infants use a peristaltic type of movement when swallowing.
Language training before birth
Teaching our tongue to do all this work begins in the womb. Before birth, the tongue begins to work by swallowing the amniotic fluid. After the birth of a child, the tongue plays a key role - it helps to squeeze milk out of the mother's breasts, working in conjunction with the jaws and lips.
When the baby is suckled to the mother's breast, the nipple and areola are retracted into the mouth so that the nipple reaches the junction of the hard and soft palate. After the baby has sucked well, the tongue begins to work, rhythmically squeezing the nipple with peristaltic movements that squeeze the milk from the mammary gland into the back of the throat, where it is swallowed. Babies naturally coordinate sucking, swallowing, and breathing.
Bottle feeding
This process changes slightly when a baby is bottle fed. The stiffness of the artificial material does not allow the nipple to stretch and take the shape of the baby's mouth. Peristaltic movements of the tongue are difficult and milk can flow almost without effort on the part of the child.
Peristaltic movements of the tongue are difficult and milk can flow almost without effort on the part of the child.
Parents should remember that during breastfeeding, babies make an effort to get milk. When bottle-feeding, milk often flows very easily and babies can drink the same amount of milk much faster (compared to breastfeeding). This may seem like a good way to save time, but as with many other things in life, slower is often better. If you choose a bottle that works more like a breast, with a slower flow, it allows the baby to stop and pause, the baby enjoys comfortable feeding, and the corresponding satiety signals are developed more slowly.
Research task
Usually everything goes smoothly. But from time to time, babies have difficulty swallowing. This may be due to various problems and they are not always easy to learn and understand.
At the beginning of the atomic era, diagnostics were carried out with the help of X-ray cinematography (filming of X-ray images). For the first time in history, people could see the amazing internal processes in the mouth and observe how the tongue helps to swallow. When concerns arose about the effects of radiation on technicians and patients, the practice was discontinued. Currently, video recording using ultrasound and MRI is often used. However, even with the use of less invasive methods or technologies, scientists still have to find ways to study babies while breastfeeding that do not affect their actions.
For the first time in history, people could see the amazing internal processes in the mouth and observe how the tongue helps to swallow. When concerns arose about the effects of radiation on technicians and patients, the practice was discontinued. Currently, video recording using ultrasound and MRI is often used. However, even with the use of less invasive methods or technologies, scientists still have to find ways to study babies while breastfeeding that do not affect their actions.
Tongue Movement Study
The 2020 study "Quantifying Tongue Movement During Feeding in Infants and Swallowing in Adults" shows patterns. The scientists used ultrasound video to study tongue movements.
“We observed the most organized and rhythmic tongue movements in exclusively breastfed infants, less mobility in those who had conditions that interfere with normal feeding, such as tongue tie, and more “disorganized” movements with bottle feeding than breastfeeding,” the researchers report. “This highlights the key role of tongue movements in breast or bottle sucking.”
“This highlights the key role of tongue movements in breast or bottle sucking.”
Disorganized movements with bottle feeding than with breastfeeding,” researchers report. “This highlights the key role of tongue movements in breast or bottle sucking.” They could also observe differences in tongue mobility before and after treatment in infants with tongue and lip frenulum. And for the first time, pictures of a baby with torticollis during breastfeeding and bottle feeding were obtained. The results showed "slightly less rhythmic sucking than usual during breastfeeding and irregular sucking during bottle feeding."
Although this study was limited, the use of ultrasound video was effective in obtaining objective information about tongue movements. As more scientists use this technique, we'll get more information about how language works and we'll be able to get more accurate information about natural feeding and how to deal with it.
Share this article:
Similar articles
Are you not a healthcare professional?
References
Genna CW, Saperstein Y, Siegel SA, Laine AF, Elad D. Quantitative imaging of tongue kinematics during infant feeding and adult swallowing reveals highly conserved patterns. Physiol Rep. 2021;9:e14685. doi.org/10.14814/phy2.14685
Quantitative imaging of tongue kinematics during infant feeding and adult swallowing reveals highly conserved patterns. Physiol Rep. 2021;9:e14685. doi.org/10.14814/phy2.14685
You are leaving the Philips Healthcare (“Philips”) official website. Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
I understand
You are about to visit a Philips global content page
Continue
Tongue sticking out: causes of malocclusion
- home
- Articles
- Children's orthodontics
- Is the child sticking out his tongue? Wait for malocclusion
There are many reasons for malocclusion, one of them is tongue dysfunction, or its permanent incorrect position. Let us tell you in more detail why the habits of sticking out the tip of the tongue, bending it, and the like are very likely to lead to orthodontic problems.
Let us tell you in more detail why the habits of sticking out the tip of the tongue, bending it, and the like are very likely to lead to orthodontic problems.
Tongue, nose, throat: everything is interconnected
The inside of a child's nasopharynx is covered with mucous, which normally should perform a protective function: to trap viruses, bacteria, dust particles and other allergens. But if the mucous membrane dries up, it becomes too thin and vulnerable.
Therefore, by the way, the child's room should be cool and quite humid.
If the house is hot, the air is dry, the nasopharyngeal mucosa dries up, and any virus can easily penetrate the thinned protective barrier. This causes frequent SARS associated with a runny nose and swelling of the nose.
Because of these diseases, the child's nasal breathing is disturbed, his mouth is constantly open and his tongue is visible. Gradually, the habit of breathing through the mouth in a dream develops.
Gradually, the habit of breathing through the mouth in a dream develops.
The mouth opens slightly, expanding the space for the tongue. And, of course, the child's tongue begins to take up this extra space in and out of the mouth.
This is how language dysfunction occurs, then it becomes fixed in the child's habits.
There is a vicious circle: frequent acute respiratory viral infections - stuffy nose - the habit of breathing through the mouth - dry mucous membranes - frequent acute respiratory viral infections, and in addition there is a dysfunction of the tongue.
All this can lead to the growth of lymphoid tissue, and hence to adenoiditis and tonsillitis, since it is the nose that provides air filtration, and when breathing through the mouth, allergens and viruses enter directly into the oropharynx. At the same time, full oxygen saturation of the blood does not occur and night sleep is disturbed - in the morning the child gets up sleepy, during the day he feels drowsy and cannot concentrate on studying.
Please note: when a child sleeps with his mouth open - this is a very disturbing symptom. Such a habit easily passes into adulthood: snoring, apnea and numerous negative consequences from this occur.
Need help?
Need help?
Sign up for a free consultation
By clicking on the "Waiting for a call" button, you confirm your consent to the processing of user data
Thank you for your application, our manager will contact you
Tongue dysfunction: how it affects the teeth
The habit of breathing through the mouth, including during sleep, leads to an increase in tongue dysfunction. The child begins to stick out his tongue more often (and the tongue is the strongest oral muscle), make additional efforts and press his tongue on his teeth.
What will happen to the teeth if such a habit develops?
- A diastema, a gap between the front teeth, may form.
- The contacts of the teeth in the anterior region may be disturbed, then an open bite will appear - a pathology that is quite difficult to correct: it causes significant harm to the condition of the teeth, since all the load falls on the chewing teeth in the lateral regions.
- The front teeth can rotate (turn around their axis) or form a protrusion - tilt forward.
Children's teeth are quite malleable, as the child grows, the size of his jaws and the place in the row of teeth constantly increase. Therefore, the efforts that the tongue exerts are quite enough to move the teeth, but they will not be able to return back to the correct position on their own.
Another problem
In addition to orthodontic problems, there will be difficulties with pronunciation of sounds. Speech therapy correction is designed for the correct structure of the teeth and the functioning of the tongue, so classes with a speech therapist will be very long and ineffective if the main cause of poor diction is not eliminated.
How to help a child?
It should be understood that these habits do not arise by themselves and not because of bad behavior. Remarks and reminders that you can not stick out your tongue will not work - you need to work with the root cause of the violation.
- Restore nasal breathing.
Orthodontists often prescribe consultations with an otolaryngologist, since the dental system and the respiratory system are closely related. Removal of adenoids, therapy of chronic diseases, normalization of the microclimate at home to reduce the frequency of acute respiratory viral infections, hardening and other restorative procedures - all this can be prescribed by a doctor to achieve remission.
ENT can help restore health for the proper functioning of the tongue- See an orthodontist.
Only in this order, otherwise the treatment will not be effective. As soon as the child is able to breathe with his mouth closed, you can proceed to correct the position of the teeth and tongue.
For this, children's orthodontic appliances were created:
- Plates.
- Trainers.
- Twin Block Apparatus.
- Kinder Smile children's aligners.
All of these devices are removable, act quite gently, guiding the teeth during their active growth. Wearing requires parental control, but with proper use, problems are solved quite quickly - in a few months.
Only after that you can start classes with a speech therapist - when the malocclusion and the main manifestations of tongue dysfunction are eliminated, the correction of sound pronunciation will be much more successful.
You can get a free diagnosis and get free consultation
The orthodontist will give you a medical opinion whether you are better suited for braces, veneers or aligners
Book an appointment in your city
Need help?
Need help?
Sign up for a free consultation
By clicking on the "Waiting for a call" button, you confirm your consent to the processing of user data
Thank you for your application, our manager will contact you
Read also:
- Contraindications for orthodontic treatment
- What threatens the wrong bite and its violation?
- Surgical correction of the bite
- Orthodontic pacifier
- Plates for straightening teeth
- Lingual braces
A million dollar smile at a bargain price!
By clicking on the "Waiting for a call" button, you confirm your consent to the processing of user data
Thank you for your application! the manager will contact you shortly.