Baby turns head while bottle feeding
Bottle Feeding Problems - Why Your Baby Squirms, Appears Uncomfortable – Baby Care Advice
When your baby squirms, appears uncomfortable during a feed, fusses, cries or refuses a bottle, seemingly fights the bottle despite being hungry, it can be challenge to figure out the cause. The timing and type of behavior she exhibits provides vital clues.
Signs of bottle-feeding problemsDoes your baby display troubled behavior in relation to bottle-feeding, such as….
- Refuses a bottle
- Turning away from the bottle.
- Refusing to close her mouth around the nipple.
- Holding nipple in the mouth but not sucking.
- Taking only a small amount and then refusing more.
- Screaming when placed into a feeding position or at the sight of the bottle.
- Milk pouring out of baby's mouth.
- Feeding too quickly.
- Feeding too slowly.
- Falling asleep before the feed is completed.
- Coughing and spluttering when feeding.
- Not consuming as much milk as expected.
- Wanting more milk than expected.
- Throwing up large amounts of milk.
Then there may be steps you can take to remedy the situation and get your baby to calmly and happily take a bottle.
Behavioral reasons‘Behavioral’ means baby’s behavior is in response to the circumstances rather than a physical cause. Behavioral reasons are the most common of all reasons for infant feeding problems. There are numerous behavioral reasons for a baby to experience feeding problems and/or display problematic feeding behavior. Common reasons include:
1. Misinterpreting baby's cues as signs of hunger Does baby at times refuse feeds?Does she take only a little and not want more?
Babies are in an oral stage of develop. Sucking is the primary way babies soothe. They also learn by sucking and mouthing objects. Many babies have a strong desire to suck for reasons that extend beyond hunger, such as tiredness, boredom, discomfort and soothing. There may be times when you mistake your baby’s desire to suck for these reasons as hunger.
Many babies have a strong desire to suck for reasons that extend beyond hunger, such as tiredness, boredom, discomfort and soothing. There may be times when you mistake your baby’s desire to suck for these reasons as hunger.
Newborn babies have an active sucking reflex. This means a newborn baby may accept a feed even when she’s not hungry, and she might guzzle down the bottle because she cannot choose to not suck when her sucking reflex is triggered. Once her sucking reflex has disappeared (usually by 3 months of age) she will willingly take only the amount she wants to take.
If you have mistakenly interpret her fussing or desire to such as hunger and offer her a feed, she might take a little and refuse the rest, or she refuse from the start. If you try to make her drink more than she wants, she will understandably get upset and fuss, cry and pull back from the bottle.
WHAT TO DO- See Hungry baby for more reasons why babies often appear
- See Infant reflexes
 Unrealistic expectationsIs baby not drinking as much as you expect?Is she fussing if you try to get her to finish a bottle?
Unrealistic expectationsIs baby not drinking as much as you expect?Is she fussing if you try to get her to finish a bottle?In around one third of consultations I have had with parents regarding an infant feeding problem, I found that parents were trying to make their baby drink more than he or she needed. In some cases, this was because of errors made their health professionals. They either failed to adjust calculations as baby matured or failed to consider baby as an individual. As a result, overestimated baby’s milk requirements.
If you think your baby is not drinking enough milk (breast milk or infant formula) you’re naturally going to feel concerned. If your concern translates into trying to pressure her to drink more than she wants or needs (gently or otherwise), you’re going to upset her. So it is very important for your peace of mind and your baby’s enjoyment at feeding times that you have realistic expectations about how much she needs.
- See How much milk does baby need for standard estimations for age and weight, and reason why a baby might take more or less than recommended.
- Follow your baby's feeding cues. Don't try to make her take more when she indicates she has had enough.
Sleeping and feeding are closely related when it comes to the needs of babies. Both are equally important to a baby's health, growth and development and feelings of wellbeing. You are no doubt aware that if your baby does not feed well she might not sleep well. But are you aware that the opposite is equally true. If she’s not getting enough sleep this has the potential to negatively impact on her feeding.
Physical fatigue can cause baby to fuss during feeds or falling asleep before the feed is completed. If you have a hungry/tired baby on your hands, tiredness will usually win out.
If you have a hungry/tired baby on your hands, tiredness will usually win out.
- Ensure baby gets enough sleep.
- Feed her before she becomes too tired.
- Aim to establish a flexible feeding and sleep routine to minimize the risk of feeding and sleep times clashing.
If your baby is often irritable and not sleeping enough, (see Overtired baby for signs and symptoms) you might find that resolving any underlying sleeping problem will cause feeding difficulties to spontaneously resolve once she receives adequate sleep.
- See our sleep section.
- Download or order a paperback copy of my infant sleep book Your Sleepless Baby: The Rescue Guide. There you will find comprehensive information on the reasons and solutions to various infant sleeping problems.
Babies over the age of 4 months can easily become distracted while feeding. They are often much more interested in the activities going on around them than they are in feeding.
They are often much more interested in the activities going on around them than they are in feeding.
Feed your baby in a quiet environment away from noise and distractions of other children.
5. Feeding managementSome feeding problems can be related to what may appear like insignificant details but which can make feeding difficult or uncomfortable for a baby. For example, how you hold your baby will affect her ability to feed from a bottle. If her head is too far forward or too far back or her neck is twisted this can make it difficult for her to suck or swallow.
WHAT TO DOSee How to bottle-fed a baby
6. Feeding aversionDoes your baby refuse to feed even when hungry?Does she scream at the sight of a bottle or when placed into a feeding position?Have you resorted to trying to feed her while asleep?A baby can develop an aversion to feeding when past feeding experiences have taught her that feeding is unpleasant, stressful or painful. Typically, baby is diagnosed with reflux and/or milk protein allergy or intolerance to explain her aversive feeding behavior. However, a behavioral feeding aversion (related to feeding management rather than a physical cause) is a far more common cause of infant feeding aversion.
Typically, baby is diagnosed with reflux and/or milk protein allergy or intolerance to explain her aversive feeding behavior. However, a behavioral feeding aversion (related to feeding management rather than a physical cause) is a far more common cause of infant feeding aversion.
A feeding aversion is the most complex of all infant feeding problems. An effective solution relies heavily on accurate identification of the cause.
WHAT TO DOSee Feeding aversion for more information. Or purchase or download a copy of 'Your Baby's Bottle-Feeding Aversion: Reasons and Solutions'.
7. Feeding equipmentDoes your baby gag, cough or splutter during feed?Does baby make clicking sounds while feeding?It could be the nipple is too long, too short, too fast or too slow.
The most important piece of feeding equipment is the nipple. The nipple needs to be the right size and speed for your baby's size, age and sucking ability. If the nipple is too long, too short, too fast or too slow for your baby, she may experience feeding difficulties and express her frustration by fuss or crying.
If the nipple is too long, too short, too fast or too slow for your baby, she may experience feeding difficulties and express her frustration by fuss or crying.
- See Feeding equipment for more information on choosing a feeding nipple.
- Experiment with nipples of different lengths, shapes and speed.
It's possible her feeding difficulties could be due to the nipple ring being screwed on too tight.
In order to maintain a neutral balance in air pressure within the bottle air needs to be able to enter the bottle to replace the void left by the milk the baby is removing. If the bottle is vented, this is achieved via the venting system. However, in the case of a non-vented bottle, the only ways air can enter the bottle are between the nipple ring and the rim of the bottle and through the holes at the end of the nipple. While sucking, a baby will maintain a seal over the holes at the end of the nipple with her tongue and prevent air entry in this way. If the nipple ring is screwed down tightly this also prevents air entry.
While sucking, a baby will maintain a seal over the holes at the end of the nipple with her tongue and prevent air entry in this way. If the nipple ring is screwed down tightly this also prevents air entry.
If air is prevented from entering the bottle, this causes a negative pressure to build in the bottle. As the pressure builds, baby need to work harder and harder to extract further milk, until such time and the air pressure is returned to normal. The effort required to suck against the negative pressure can cause a newborn baby to tire and fall asleep before completing the feed. An older baby may simply give up or express her frustration.
WHAT TO DOThe nipple collapsing (not all will) or stopping to burp baby allows air to enter through the holes and neutralize the pressure. But you don’t want to wait for this to resolve the problem. By then baby is already tiring or getting frustrated. See ‘Collapsing nipple’ for ways to manage this problem.
9. Feeding patternsIs your baby often take only small amounts, refuse more, but then wants to feed again an hour or two later?
Feeding patternsIs your baby often take only small amounts, refuse more, but then wants to feed again an hour or two later?Some babies develop a grazing or snacking feeding pattern where they will only drink small amounts of formula at a time and then want to be feed frequently, possibly every hour or two. Although this will not cause any problems for a baby, provided she drinks enough formula in total over a 24 hour period, it can become very tiring for parents to keep up with her constant demands for feeding.
WHAT TO DO- Try to encourage your baby to take as much milk as possible within 45 minutes. But don't try to make her feed if she doesn't want to. Stop sooner if she does not want to continue.
- Ensure baby gets plenty of sleep.
- Avoid allowing baby to fall asleep while feeding.
- Support your baby to extend the time between feeds, by offering a little water, a pacifier, a nap, playing with her, or taking her for a walk.
 Aim to encourage her to wait at least 3 hours from time you started her previous feed, but only if it's reasonable to do so without distressing her. If necessary extend the time between feeds gradually. As your baby gets used to going longer periods between feeds she will gradually take larger amounts at each feed.
Aim to encourage her to wait at least 3 hours from time you started her previous feed, but only if it's reasonable to do so without distressing her. If necessary extend the time between feeds gradually. As your baby gets used to going longer periods between feeds she will gradually take larger amounts at each feed.
Unless your baby was born prematurely or is very small for her age, developmentally she no longer requires feeding during the night beyond the age 6 months. If nighttime feeding continues past this age its not going to harm her but it could have a negative effect on her appetite and feeding patterns during the day.
Your baby only needs a certain number of calories in her day (24 hours) to provide for her growth and energy needs. If after the age of 6 months she continues to receive calories from nighttime feeds this will dampen her appetite during the day and she will not need to drink as much formula during daytime feeds. You might find she is content to go for long periods of time between feeds (which is usually what would happen at night). She might fuss or refuse some of her daytime bottles when they are offered simply because she's not hungry at the time. Or she might graze during the day.
You might find she is content to go for long periods of time between feeds (which is usually what would happen at night). She might fuss or refuse some of her daytime bottles when they are offered simply because she's not hungry at the time. Or she might graze during the day.
Nighttime feeding will cause your baby no harm, so if you're happy to continue feeding her during the night there's no reason to change a thing. However, it is important that you don't expect her to consume as much milk during the day as she may have otherwise taken if she did not feed at night.
Many babies will give up night time feedings on their own accord, but others will continue to wake and demand feeds overnight for months and possibly years while parents continue to provide feeds at night. Usually the reason babies continues to demand night feeds beyond the age of 6 months is because they have learned to rely on feeding as a way to fall asleep, or because their internal body clock gets turned around - where the baby has decreased appetite during the day because of the continued night feeds and as a consequence of small feeds during the day the baby wakes hungry during the night. Body clock problems can easily become a cyclical pattern that will continue over the long term unless parents take steps to change the situation. Healthy, thriving babies who continue to demand feedings at night beyond the age of 6 months often require guidance and support from parents to cease feeding at night and turn their body clock around to a normal day-night feeding pattern.
Body clock problems can easily become a cyclical pattern that will continue over the long term unless parents take steps to change the situation. Healthy, thriving babies who continue to demand feedings at night beyond the age of 6 months often require guidance and support from parents to cease feeding at night and turn their body clock around to a normal day-night feeding pattern.
Aim to cease overnight feeds after 6 months of age. However, before attempting to do this it's important to address any feeding to sleep issues your baby might have. She would need to learn to fall asleep in a different way before you will be able to successfully encourage her to cease night feeds.
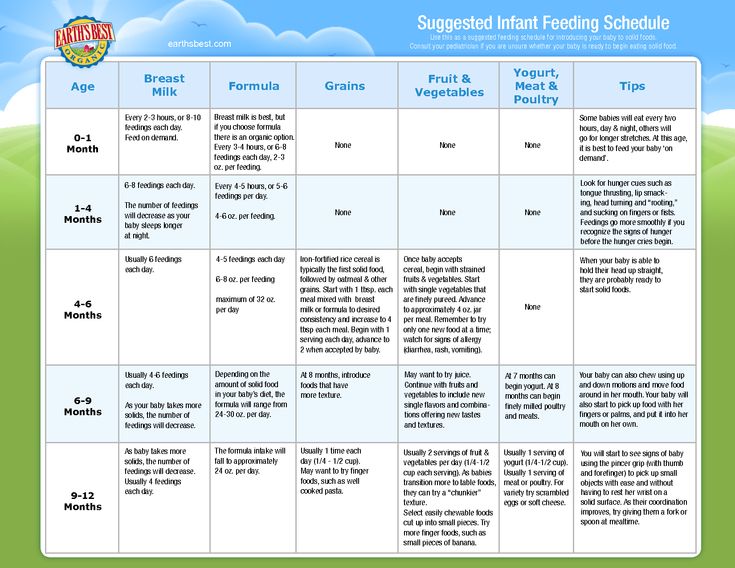
11. Starting solids earlyHave you started giving your baby solids before the age of 4 months?Have you been advised to start solids early?6 months is the recommended age for starting solid foods. Although a small number of babies may benefit from solids prior to this age, it's generally not recommended to start a baby on solid foods before the age of 4 months. An early start on solids has the potential to cause bottle feeding problems because solid foods may decrease the baby's appetite for milk (breast milk or formula).
Although a small number of babies may benefit from solids prior to this age, it's generally not recommended to start a baby on solid foods before the age of 4 months. An early start on solids has the potential to cause bottle feeding problems because solid foods may decrease the baby's appetite for milk (breast milk or formula).
- If your baby is less than 6 months old, either cease or reduce the amount of solids you offer to see if this helps to improve the situation.
- See our article on starting solids.
If solids are offered prior to bottle feeds, either directly before or mid way between feeds, when it's time for your baby's bottle feed she might be feeling full from the solids, in which case she's probably not going to take much milk from her bottle.
WHAT TO DO- For babies 4 - 9 months (when milk is still the most important food) offer solids 15 - 20 minutes after bottle feeds.
- For babies 9 - 12 months (when solids are becoming increasingly more important to a baby's diet) offer solids shortly before or shortly after her bottle, whichever you find works best. Babies at this age are often down to 3 bottles per day plus 3 main meals and 1 or 2 snacks.
In these early stages of learning to eat solids (4 - 7 months) solids are not needed to add value to a baby's nutritional intake, rather they are offered primarily to provide learning experiences. The baby is exposed to new food proteins that help prime her immune system. She gets to discover new tastes and textures and become accustomed to eating from a spoon. It is at this age that babies are most willing to accept new tastes. So variety rather than quantity is what solids are about.
Many babies, particularly very young babies, experience difficulty self-regulating their dietary intake. Some babies will continue to eat solid foods for as long their parents keep offering. Some babies will prefer eating solids compared to drinking formula. However, too much solids and not enough milk is not a balance diet for a baby. It may be necessary for parents to limit the amount of solids they offer in order to encourage their baby to have a greater appetite for milk feeds.
Some babies will continue to eat solid foods for as long their parents keep offering. Some babies will prefer eating solids compared to drinking formula. However, too much solids and not enough milk is not a balance diet for a baby. It may be necessary for parents to limit the amount of solids they offer in order to encourage their baby to have a greater appetite for milk feeds.
See our article on estimating how much milk your baby needs to make sure she's getting enough.
14. Weaning difficultiesDoes your breastfed baby refuse bottle-feeds?Does your baby have a breast preference?While some breastfed babies willing accept milk from a bottle many will not, at least not straight away.
Difficulty weaning from breast to bottle is rarely resolved by finding the 'right' feeding nipple. (All feeding nipples will feel equally foreign to a breastfed baby. ) Nor does a solution lie in finding a formula with the 'right' taste. All formula will taste strange to a breastfed baby). The difficulty associated with weaning to a bottle most often lies in the fact that bottle-feeding requires a very different sucking action to breastfeeding. While breastfeeding the movement of your baby's tongue milks the breast, where as bottle-feeding requires a sucking action. A baby who has been exclusively breastfed beyond the age of 3 months will often refuse milk from a bottle because it "doesn't feel right" and she doesn't know how to suck from a bottle.
) Nor does a solution lie in finding a formula with the 'right' taste. All formula will taste strange to a breastfed baby). The difficulty associated with weaning to a bottle most often lies in the fact that bottle-feeding requires a very different sucking action to breastfeeding. While breastfeeding the movement of your baby's tongue milks the breast, where as bottle-feeding requires a sucking action. A baby who has been exclusively breastfed beyond the age of 3 months will often refuse milk from a bottle because it "doesn't feel right" and she doesn't know how to suck from a bottle.
It takes time and practice before a breastfed baby learns how to suck on a bottle.
WHAT TO DO- Try offering expressed breast milk in a bottle initially. (Don't be too optimistic and put too much in to start with. It would be a shame to waste it).
- A soft flexible nipple often works better.
NOTE: Many breast fed babies will refuse to accept a bottle while they are still being breastfed at times. They will simply wait until a breastfeed is offered. For these babies it will be the case of breastfeeding or bottle-feeding, but not both.
They will simply wait until a breastfeed is offered. For these babies it will be the case of breastfeeding or bottle-feeding, but not both.
- Your Baby's Bottle-feeding Aversion book
- Baby Care Advice consultation
- Rowena Bennett's Online Bottle-Feeding Aversion Program
In my book, ‘Your baby’s Bottle-feeding Aversion’, I have described physical and behavioral reasons for babies to develop an aversion to bottle-feeding. How to identify the cause and the solutions to match. Included are step-by-step instructions on how to regain your baby’s trust and resolve a feeding aversion caused or reinforced by repeated pressure to feed.
While the book was written for bottle-fed babies, many nursing mothers have found that applying the same strategies has also helped them to successfully resolve a breastfeeding aversion.
You might find that reading this book is all you need to do to understand the steps you need to take to resolve your baby’s feeding aversion and get him back to the point of enjoying eating until satisfied.
Baby Care Advice ConsultationsIf you would like an individualized assessment of all reasons for infant feeding problems, not just feeding aversion, we also provide a consultation service. Baby Care Advice consultants have extensive experience in pinpointing the cause of feeding aversion and other behavioral feeding problems such as those related to equipment and the parent’s feeding practices. (For more on what’s included in a consultation).
By Rowena Bennett, RN, RM, CHN, MHN, IBCLC.
Copyright www.babycareadvice.com 2021. All rights reserved. Permission from the author must be obtained to reproduce all or any part of this article.
Rowena's Online Bottle-Feeding Aversion ProgramSix time-saving modules to help your family enjoy feeding again with Rowena's step-by-step plan. Enjoy additional tools to manage anxiety, troubleshoot any issues, introduce new carers, how to manage illness/teething and much more.
Enjoy additional tools to manage anxiety, troubleshoot any issues, introduce new carers, how to manage illness/teething and much more.
- Module 1: Understanding feeding aversions
- Module 2: Identify the cause
- Module 3: Prepare for success
- Module 4: How to resolve your baby's bottle-feeding aversion
- Module 5: What to expect
- Module 6: Troubleshooting
- BONUS: Guided meditations
Why they do this and when to see a doctor
In most cases, a baby will begin deliberately moving their head in the first months of life. They can usually turn it toward a sound by 2 months. By the end of the first year, and often much earlier, many babies begin shaking their head.
Head shaking can be a normal developmental milestone relating to reflexes and motor skills. However, some types of head shaking may signal a problem.
However, some types of head shaking may signal a problem.
In this article, we examine the reasons why a baby may shake their head. We also look at related medical conditions for head shaking and explain when to contact a doctor.
Gaining control of the head is a major developmental milestone.
At about 2 months old, most babies begin turning their head toward sounds. They continue gaining head control and can easily lift and move their head by 4 months. Some parents and caregivers also notice that head shaking begins around this time.
Developmental reasons why a baby might shake their head include:
Experimentation
Babies master new skills by practicing them. For an infant with little control over the world, increasing head control is a major change.
A baby who has recently learned to control their head may turn it from side to side and experiment with moving it into different positions.
Listening to sounds
A baby will commonly move their head toward familiar or interesting sounds, such as a loud crash or a parent’s or caregiver’s voice.
If two or more people are talking, or there are several competing noises in a room, a baby may move their head back and forth, trying to follow the sounds.
In a quieter room, the head movements may stop.
Communication
Babies can understand words well before they can talk. As a result, they may start understanding some of what parents or caregivers say to them at about 6 months. A baby may shake their head to communicate with them.
By a year, many babies shake their head to signal “no” or frustration.
Self-soothing
Some babies find it soothing to shake their head from side to side. They may do this when they are overstimulated, anxious, or trying to fall asleep.
Self-soothing is harmless and may help a baby feel less anxious in new situations.
When a baby shakes their head because something is wrong, they often have other symptoms simultaneously.
Parents and caregivers should monitor head shaking that accompanies other signs and symptoms, such as crying or not meeting developmental milestones.
Some things to watch for include:
Pain or ear infection
Some babies may shake their head to soothe themselves if they are in pain.
Sudden head shaking may be a sign of an ear infection, especially if the baby has a fever or grabs at their ear. Doctors may prescribe antibiotics to treat ear infections.
Epilepsy
Some people with epilepsy, including babies, have myoclonic jerks. These are very short seizures that cause sudden contractions in the muscles.
While myoclonic jerks can affect any part of the body, they may cause some babies to turn their head or neck. The jerks are very short, and parents or caregivers may not initially recognize them as seizures.
Myoclonic jerks happen suddenly and can be forceful. If a baby has these, it will not look as though they are voluntarily shaking their head.
Autism and other developmental issues
Some people with autism move their body to self-soothe or stimulate themselves. They may nod or shake their head, usually in rhythmic motions.
It is possible that an infant may be autistic if they:
- do not meet developmental milestones
- gain and then lose skills
- do not make eye contact with or respond to parents or caregivers
Neurological disorders
Head shaking may signal a neurological problem, especially if a baby seems unable to control it or has other unusual movements or behaviors.
For example, a condition called rhombencephalosynapsis causes differences in the formation of the brain’s cerebellum. A 2013 study found that 50 of 59 children with this condition had persistent head shaking for years before a doctor formally diagnosed them.
Babies with neurological disorders may not meet developmental milestones and may have trouble with speech, movement, and other age-typical behaviors.
Shuddering attacks
Very rarely, babies and young children experience so-called shuddering attacks, which seem to occur spontaneously. A baby’s body may shake or shiver, and these movements might extend to their head.
Doctors do not know what causes these attacks, but they are usually harmless. However, a doctor may first rule out other causes, such as neurological conditions or head injuries.
It is never too early to see a doctor for worrisome or unusual behavior in a baby.
Early interventions can help for a severe developmental or neurological problem, and early treatment for ear infections and other common conditions may prevent these conditions from worsening.
A person should take a baby to the doctor’s office if they:
- do not meet their developmental milestones — for example, if a baby does not move their head toward sounds by 4 months
- have other symptoms along with the head shaking, such as fever
- seem distressed
- are unable to control their head or their movements
Parents or caregivers should also discuss any new behaviors at the baby’s next well-child visit.
As babies discover the world, they continually develop new skills. Sometimes, unusual behaviors appear along with these skills.
Sometimes, unusual behaviors appear along with these skills.
In most cases, head shaking is a normal, developmentally appropriate behavior that shows that a baby is exploring and interacting with their world.
If a baby has any accompanying symptoms or seems distressed, it is important to take them to see a doctor.
Baby won't take a bottle | Philips Avent
search support iconSearch Keywords
Home ›› What to do when your baby refuses a bottle
↑ top
any problems. If your breastfed baby refuses a bottle, don't worry. This is a common occurrence in many babies who are used to breastfeeding. Obviously, this can create certain difficulties for moms, especially if you need to return to work in the near future.
3 Philips Avent products to help you bottle feed:
So why is your baby refusing to bottle and crying? There are many ways to quickly and easily teach a breastfed baby to a bottle. Here are important tips on what to do when your baby refuses a bottle.
Here are important tips on what to do when your baby refuses a bottle.
Is the baby refusing the bottle? Take a step back
If your baby cries while bottle feeding, the first thing to do is to start over and rethink your feeding approach and technique. Try the following steps when bottle feeding your baby: [1]
- Lift and tilt your baby's head forward. Before inserting the pacifier into the baby's mouth, make sure that the baby's head is raised and tilted over his body to avoid choking: so that the baby does not choke and have the opportunity to burp during bottle feeding.
- Insert the pacifier. Bring the pacifier to the baby's lips and gently guide it into the baby's mouth. In no case do not try to press the nipple on the baby's lips and try to push it into his mouth. After touching the pacifier to the baby's lips, wait for the baby to open his mouth and take the pacifier.
- Hold the bottle at an angle. Tilt the bottle at an angle so that the nipple is only half full.
 So the child can eat at his own pace.
So the child can eat at his own pace. - Let the baby burp during and after feeding. It can be useful for a child to burp not only after feeding, but also approximately in the middle of the process. This will help reduce gas or tummy discomfort that your baby may experience from swallowing too much air.
- Stop in time, do not overfeed the baby. If the baby begins to turn his head away from the bottle or closes his mouth, then he is full and you need to stop feeding.
- Perhaps the flow of milk from the nipple to the baby is weak or, on the contrary, too fast, so he is naughty and refuses the bottle. Try changing the nipple to a nipple with a different flow.
Other tips if your baby refuses the bottle
If you've followed the steps above and your baby still refuses the bottle, don't worry. There are other ways to help bottle feed your baby. Here are some simple tricks you can add to your bottle feeding process. [2]
1. Remind your child about mom.
Remind your child about mom.
Sometimes a child can be fed by someone other than his mother - dad, grandmother or, for example, a nanny. If your baby fusses while bottle feeding, try wrapping the bottle in something that smells like mommy, like a piece of clothing or some fabric. This will make it easier to feed the baby when the mother is not around.
2. Try to maintain skin contact while bottle feeding.
Some babies need contact with their mother, so try bottle feeding while leaning against you. However, some babies are better at bottle feeding when they are in the exact opposite position than when they are breastfed. For example, there is a position with bent legs. Lay the child on your bent knees, facing you, pointing the child's legs towards your stomach. During feeding, the baby will be able to look at you and contact you in this way. If your baby refuses a bottle, experiment to see which works best.
3. Move while feeding.
Move while feeding.
Sometimes all it takes to get your baby to take the bottle is a little wiggle or walk. The next time your baby starts crying while bottle feeding, try moving around a little rhythmically to calm him down.
4. Try changing the milk temperature.
If the baby still does not want to take the bottle, check if the milk in the bottle is too hot or too cold. Before feeding, put some warm breast milk on the inside of your wrist to check the temperature. Milk should be warm, but if it seemed hot to you, just place the bottle for a short while under a stream of cold water.
Choosing the right bottle for your baby If you plan to combine bottle feeding with breastfeeding, it is advisable to choose bottles with a nipple that will have a wide base as the bottle will grip closer to the breast. Also pay attention to the fact that the nipple is firm and flexible, the child must make an effort to drink from the bottle, as well as from the breast.
 Give preference to nipples with an anti-colic valve that vents air out of the bottle.
Give preference to nipples with an anti-colic valve that vents air out of the bottle. Natural bottle allows you to combine breast and bottle feeding. 83.3% of babies switch from a Natural bottle to breastfeeding and back.*
If you choose a bottle for artificial feeding, traditional bottles are fine, but it is desirable that the nipple is made of a hypoallergenic material, such as silicone, has an anti-colic valve and did not stick together when bottle fed. In case your baby spit up often, then use special bottles with anti-colic and anti-reflux valve, which reduces the risk of spitting up and colic.
Bottle with unique AirFree valve reduces the risk of colic, gas and spitting up. With this bottle, you can feed your baby in an upright or semi-upright position to reduce spitting up. Due to the fact that the nipple is filled with milk and not air during feeding, the baby does not swallow air, which means that feeding will be more comfortable.
Both bottles are indispensable if you want to breastfeed, bottle feed or just bottle feed your baby.
“My baby refuses to breastfeed but bottle feeds – help!”
Sometimes a baby gets used to bottle feeding and refuses to breastfeed. Therefore, it is important to use bottles that are suitable for combining breastfeeding with bottle feeding. If, nevertheless, you are faced with the fact that the child refuses to take the breast, try using silicone nipple covers to make the transition from the bottle to the breast and back more imperceptible.
Remember that if you want to combine breastfeeding and bottle feeding, it is worth waiting at least a month before offering a bottle, so that you are lactating and have time to get used to each other and develop a breastfeeding regimen.
Breastfeed and bottle feed your baby with pleasure
Remember that it takes a while for your baby to get used to bottle feeding. This is completely normal. If you have to go to work, be sure to set aside enough time to bottle train your baby beforehand.
Remember that every child is different, so what works for one may not work for another. With a little time and patience, you will find out what works best for your baby when he refuses a bottle.
You will identify your child's unique needs. However, if your baby still refuses the bottle after all the steps above, check with your pediatrician.
Articles and tips from Philips Avent
References:
*O.L. Lukoyanova, T.E. Borovik, I.A. Belyaeva, G.V. Yatsyk; NTsZD RAMS; 1st Moscow State Medical University THEM. Sechenova, "The use of modern technological methods to maintain successful breastfeeding", RF, 10/02/2012 3 llli.org - The Baby Who Doesn't Nurse
llli.org - Introducing a Bottle to a Breastfed Baby
Baby+ app
Download the app and track your child's development and growth with trackers and save those special moments forever.
Download app:
You are leaving the Philips Healthcare (“Philips”) official website.![]() Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
I understand
You are about to visit a Philips global content page
Continue
You are about to visit the Philips USA website.
I understand
90,000 Memo for parents - GBUZ JSC City Clinic No. 10m Era of the prevention of accidents
Rules for feeding and sleep of the child 9000 . Get into a comfortable sitting or lying position. Bring the baby to your chest so that his head and body are in the same plane. The baby should be facing the breast: its nose is located opposite the nipple.
1.2. If desired, you can support the chest from below with your whole hand or put four fingers under the chest, and the fifth (large) on top.
1.3. Touch the nipple to the baby's lips, and when the baby opens his mouth wide, press his body tightly to you. If the baby is properly attached to the breast, he captures with his mouth not only the nipple, but also most of the halo with the tissue located under it.
In this case: the child's chin touches the chest; his mouth is wide open; his lower lip is turned outward; you can see most of the halos above the upper lip and not under the lower. You do not experience any discomfort in the chest.
1.4. As a rule, the child himself releases the chest satisfied and sleepy.
1.5. The baby's nasal passages should not be blocked by the mother's breast during feeding.
1.6. Hold the baby at the sternum for more than 20 minutes. The baby sucks out most of the required volume of feeding in 5-10 minutes, the rest of the time it mainly satisfies the sucking reflex.
- Artificial feeding
2.1. In bottle feeding, adequate selection of the opening in the nipple is of great importance.
2.2. The hole should be such that when the milk bottle is tipped over, the milk will flow out only in drops through the hole in the nipple.
2.3. When feeding from a bottle, make sure that the neck of the bottle and the nipple are constantly filled with formula and do not contain air during feeding. Air entering the neck causes air to be sucked in by the baby. In this case, the child does not eat up, and he easily has regurgitation and vomiting.
2.4. The nutrient mixture should be warm. A cold or hot mixture can cause a reflex spasm of the muscles of the esophagus and stomach.
2.5. After feeding, it is necessary to hold the child in an upright position for 2-3 minutes, which will facilitate the discharge of air that has entered the stomach during feeding.
2.6. As a rule, the child himself releases the breast (or bottle) satisfied and sleepy.
- Sleep rules
3.1. The best place for sleeping a child of the first year of life is a crib in the parents' bedroom, for children over 1 year old - a crib in the nursery. Sleeping in the same bed with parents is prohibited.
Sleeping in the same bed with parents is prohibited.
- Prevention of aspiration in children
Aspiration in children is the ingestion of a foreign body (milk, milk formula, pieces of food, stomach contents) into the respiratory tract.
4.1. In newborns, aspiration may be caused by regurgitation of breast milk or formula. Follow the rules for feeding children. After feeding, the newborn baby should be laid on the barrel, turning the head to the side.
4.2. During feeding, the nasal passages of the child should not be closed by the mother's breast.
4.3. During breastfeeding, it is necessary to refrain from alcohol - alcohol dulls the vigilance of the mother. A woman who has drunk can take the child with her to bed so that she can feed him at night without waking up. The child may choke, suffocate, or get other injuries.
4.4. During a meal, the act of swallowing can be affected by various psycho-emotional states. Sudden laughter, screaming, fright, or crying can cause a food bolus to back up from the pharynx into the upper respiratory tract.
Sudden laughter, screaming, fright, or crying can cause a food bolus to back up from the pharynx into the upper respiratory tract.
4.5. Be careful with a small child. Don't leave him alone! Do not allow small objects (coins, balls, buttons and other small objects) to be played with. Pay attention to small fragments of toys, even if the child is in front of your eyes, because inhaling them is a matter of a few seconds!
4.6. You do not need to feed your baby nuts, seeds, peas, dense whole berries, small sweets, because babies often inhale these foods. Don't risk your own children's lives!!
- Burn prevention
5.1. Children should not be left unattended.
5.2. Make sure that there are no hot objects ( hot food or liquids, sockets, running iron, etc. ) in the reach of children.
5.3. Items that can cause burns ( matches, hot objects, chemicals and other ) should be kept out of the reach of children.
5.4. Don't let a small child turn on the taps in the bathroom and kitchen until he or she knows how to mix hot and cold water. Even water at 60 degrees can cause a serious burn in just half a minute of contact with it. You should carefully check the water before bathing and in the process of bathing the child.
5.5. Do not carry hot liquids and food over areas where the child plays.
5.6. Do not open the oven if there is a small child in the kitchen.
5.7. Avoid using open coil heaters (boilers).
5.8. When cooking on the stove, turn on the back burners and turn the pots and pans with their handles inward. This will prevent children and you yourself from accidentally turning over a hot pot or pan.
5.9. Do not delay repairing faulty electrical outlets and plugs. Do not use appliances with faulty wiring.
5.10. A high danger is fraught with an electric kettle, especially one that has just boiled. Therefore, even if you are sure that the device itself is located out of the reach of the child, still check the location of its cord as well - whether the child can pull it and tip the kettle over.
5.11. Cover accessible sockets with special devices so that your baby cannot put anything into them. Electrical cords from appliances should be out of reach of the child - the baby can take the cord in his roti and try to bite it.
Burn Prevention
Prevention of burns in young children is primarily the care and responsibility of the adults who are nearby.
Dear parents, be careful!
Every fifth injury in children is a burn. Sometimes a few seconds are enough for the irreparable to happen, so the child must be under the PERMANENT supervision of adults.
- Prevention of children falling out of windows
To avoid an accident involving a child falling out of a window, the following rules must be followed:
6.1. When opening windows in the apartment and ventilating the room, make sure that the child is under supervision.
6.2. During ventilation, open transoms and vents. If you do open a window, then do not open it more than 10 cm, set limiters for this purpose.
If you do open a window, then do not open it more than 10 cm, set limiters for this purpose.
6.3. Do not allow a child to go to the balcony without adult supervision.
6.4. Never leave a sleeping child alone in the apartment. The baby can wake up and climb to the open window.
6.5. Move all furniture, including beds, away from windows. This will help prevent your baby from accidentally getting on the windowsill.
6.6. Do not show your child how the window opens. The later he learns to open the window on his own, the safer his stay in the apartment will be.
6.7. Do not teach your child to place a chair or other device under their feet in order to look out the window or look into the street from the balcony. Subsequently, acting in this way, he may lean out too much and fall out of the window (from the balcony).
6.8. Mosquito nets pose a great danger: the child sees some obstacle in front, confidently leans on it, and as a result, the child can fall out along with the net, which is not designed for the weight of even the smallest one-year-old baby.
6.9. If a child of 5-7 years old is afraid to be alone in the apartment, do not leave him even for a short time. Often, feeling fear, children look out the window or from the balcony, hoping to see their parents, which may cause them to fall from the balcony.
Today we will talk about some aspects of the prevention of respiratory infections in children.
Acute respiratory infections in children are the most common reason for seeking medical help from a pediatrician, pulmonologist, ENT doctor.
As a rule, the incidence increases sharply from the moment the child visits preschool institutions.
Respiratory pathogens (viruses, bacteria) are characterized by damage to the mucous membranes of the respiratory tract and weakening of local protective factors.
Most infectious agents enter through the nasal mucosa.
In order to strengthen this natural barrier, various agents are often used that are injected directly into the nasal passages, i. e. intranasally.
e. intranasally.
The first thing we usually start with is saline solutions.
In outpatient and inpatient practice, we most often use isotonic saline or 0.9% sodium chloride solution, as well as various preparations based on sterile sea water, which can be isotonic and hypertonic.
These products can be used both for the purpose of daily hygiene of the nasal cavity, and for the prevention and treatment of ARI.
Salt solutions, being quite safe, help to remove mucus and normalize the protective function of the ciliated epithelium of the nasal mucosa. Hypertonic solutions help reduce mucosal edema.
Recombinant interferons are currently popular in the form of drops, spray, ointment, gel, and oxolinic ointment.
However, these drugs do not have very high activity.
Apricot oil, lanolin, vaseline, which are part of the ointments, also prevent the penetration of viruses into the cells of the nasal mucosa.
Also have barrier properties agents that are powdered cellulose of vegetable origin.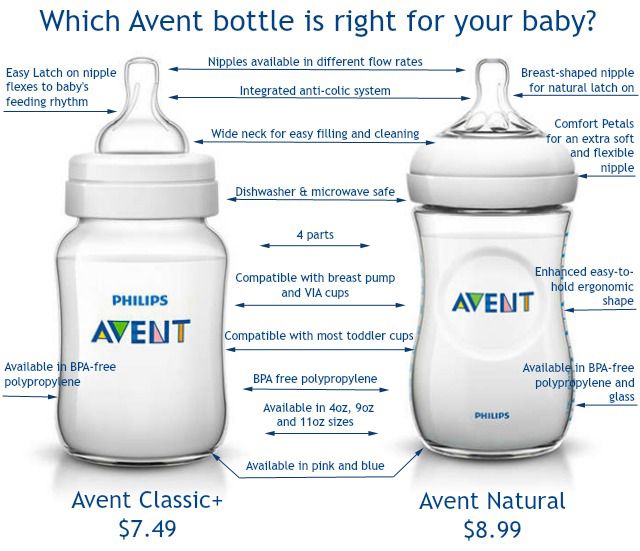
These preparations contribute to the protection of the nasal mucosa from contact with viruses (also with allergens), thanks to the formation of a special film.
The next group of drugs is bacterial lysates in the form of an intranasal spray, which include antigens from almost all major pathogens of upper respiratory tract infections.
Bacterial lysates stimulate local defense factors, which leads to both preventive and curative effects.
And in conclusion, I would like to say that
- All of the listed drugs should be used as prescribed by a doctor in accordance with the instructions.
- Comply with storage conditions.
- When choosing an intranasal preparation, individual tolerance must be taken into account.
- Vaccination is the most effective way to prevent respiratory infections.
First aid procedure
Subfebrile temperature (up to 38°C)
- Undress the child.
- Wipe with a damp cloth (slightly above room temperature).

- Do not use antipyretics.
Febrile temperature (above 38°C)
- Keep calm, put to bed.
- Drink plenty of sweet tea, fruit drink.
- Keep the child warm in case of chills (warm blanket, hot tea).
- Give antipyretics.
- At a temperature of 39.5-40°C, the child should not be wrapped.
- If the temperature is above 40.4°C, call for emergency help and give an antipyretic.
Specialist comment (pediatrician, candidate of medical sciences Gavrilova T. A.)
The normal temperature is not 36.6°C, as is often believed, but 36.0–37.0°C, in the evening it is slightly higher, than in the morning. Body temperature rises with many diseases. The benefits of elevated temperature are a signal of illness, a way to fight pathogens (many bacteria and viruses stop multiplying at temperatures above 37-38 ° C), this is a stimulus for the immune response, since a number of protective factors (including interferon) are released only at temperatures above 38°C.
By lowering the fever, we do not affect the cause of the disease, but we can improve the child's well-being. Subfebrile temperature (up to 38 ° C) may appear when overheating, with a viral or bacterial infection. Taking antipyretics in such cases is not worth it if the child's well-being does not suffer.
At a "febrile" temperature (above 38°C), there is vasoconstriction, increased muscle contractions (hence - chills, trembling), in young children - convulsions (the so-called "febrile" convulsions).
When the temperature rises to 39.5–40.0°C, the skin vessels dilate (the skin turns red), such a child should not be wrapped up.
Fever is dangerous in spasm of skin vessels - this is malignant hyperthermia.
Symptoms:
- temperature above 40.4°C;
- mottled, marbled skin;
- limbs cold to the touch;
It is necessary to call an emergency and be sure to give an antipyretic, preferably in a solution inside.
Antipyretics Children should be given antipyretics at temperatures above 38.