Bottle feeding tongue tied babies
Does a Lip-Tie or Tongue-Tie Affect Bottle-Feeding? - Alabama Tongue-Tie Center | Dr. Richard Baxter
by Richard Baxter, DMD, MS | Oct 17, 2021
These are excellent questions we hear from parents on a daily basis. Many parents are told by providers to “just give him a bottle” and it will solve the issues they are struggling with from the tongue-tie. The problem is, it’s not true. Switching to a bottle takes away the maternal aspect (pain, plugged ducts, supply issues, etc.), but it does not fix the infant issues of a poor latch, milk leaking out, reflux, excessive gas, colic, and slow feeding with possible weight gain issues.
In the 1920s when formula came out, it was sold to parents as “better than breastmilk” so if a baby was tongue-tied, you might as well feed them formula since it’s “superior.” Fast forward 70 years and with renewed research in the 1990s and an emphasis on breastfeeding, more moms began nursing because, in fact, breastmilk is far superior to infant formula. Also, the act of nursing is superior to bottle-feeding, as it helps to mold the palate, and set the child up for healthy airways and craniofacial growth. That is to say, if you are bottle-feeding, don’t feel that ever-present mom guilt, as babies can still thrive with formula or bottle-feeding, and many moms need to supplement for various reasons (our twins were bottle-fed, and are now thriving 7-year-olds).
With tongue-ties, it’s heartbreaking when moms come to see us months after the baby is born and has been struggling with an undiagnosed tongue or lip-tie, and mom had to give up nursing and has now lost her milk supply. It takes a while for parents to put the puzzling symptoms together, and providers lack education on the impact of tongue- and lip-ties. This happens on an almost daily basis, and to the parents’ surprise, switching to a bottle has not magically solved the problems. They have tried five different bottles and are still struggling. The baby is still leaking milk, fussy, gassy, colicky, struggling to sleep, spitting up all the time, hiccuping after every feed, and seems always hungry. Most of the time, it’s a less obvious posterior tongue-tie, as if it was to-the-tip, many providers would have seen it and informed the parents. (But we see lots of to-the-tip or anterior ties go undiagnosed for months as well, surprisingly! Education in this space is lacking at medical and dental schools and residency programs.)
The baby is still leaking milk, fussy, gassy, colicky, struggling to sleep, spitting up all the time, hiccuping after every feed, and seems always hungry. Most of the time, it’s a less obvious posterior tongue-tie, as if it was to-the-tip, many providers would have seen it and informed the parents. (But we see lots of to-the-tip or anterior ties go undiagnosed for months as well, surprisingly! Education in this space is lacking at medical and dental schools and residency programs.)
Posterior Tongue-Tie in Infant After Lifting Properly
Recently, a new study by Dr. Bobby Ghaheri confirmed what we see daily at our office. In a randomized controlled trial (RCT), he showed with a special bottle with a computerized nipple, that babies feed more efficiently, are better able to adapt to changes in feeding, and had more rhythmic and coordinated sucking after a proper posterior tongue-tie release. Moms also saw less nipple pain, were more confident in feeding their babies, and the babies had less spit-up, fewer hiccups, and were less fussy after having their posterior (less obvious!) tie released with a CO2 laser. This study is important because it shows that not just anterior or obvious ties cause problems, but posterior ties also cause issues. It also shows that switching to a bottle will not solve the issue. If there is a physical restriction of the tongue, and the baby has the symptoms of a tie (see image), then that baby would very likely experience improvement after a proper, full tongue-tie release by an experienced provider.
This study is important because it shows that not just anterior or obvious ties cause problems, but posterior ties also cause issues. It also shows that switching to a bottle will not solve the issue. If there is a physical restriction of the tongue, and the baby has the symptoms of a tie (see image), then that baby would very likely experience improvement after a proper, full tongue-tie release by an experienced provider.
All of the issues at the top of the symptoms sheet can be experienced by bottle-feeding babies. Tongue-ties do not always lead to weight gain issues, so we hear daily that the primary care provider said “he’s gaining weight, so he is fine” and the parents think the tie doesn’t need to be treated. First, mom may have an oversupply, or be constantly feeding him, or any number of other ways to compensate, so the baby is still “fine” but not “thriving.” We want optimal health and growth, not just “fine” or survival. If moms and babies have more than a few symptoms on this form, it means they are on the struggle bus and are not thriving! Plus, a tongue restriction can have lifelong effects including speech, solid feeding, or sleep issues in the future (see below for child to adult symptoms).
If moms and babies have more than a few symptoms on this form, it means they are on the struggle bus and are not thriving! Plus, a tongue restriction can have lifelong effects including speech, solid feeding, or sleep issues in the future (see below for child to adult symptoms).
Probably 75% of the babies that come see us have a lip-tie that is fairly obvious (that’s what brings them to our office), but also have a less obvious tight, thick, restrictive tongue-tie that is causing feeding difficulty. In fact, for moms that are nursing, the posterior tongue-tie very often is to blame for the 7+, toe-curling pain they are experiencing. This is highly unfortunate because those are the babies that are told to switch to a bottle because of the terrible pain, and moms are told the baby has “no tongue-tie” because it is not easily seen with a tongue depressor or on a quick inspection of the mouth.
If your baby is struggling with these symptoms, whether nursing or bottle-feeding, and you are concerned there might be a tongue-tie, please contact our office and we would love to get you in for a consultation to check for a restricted lip- or tongue-tie. The more checkmarks on that list of symptoms, the higher the chances of having a tongue- or lip-tie. Call 205-419-4333 to set up a consult, or send us a message. It would be an honor to help you and your family. – Dr. Baxter
The more checkmarks on that list of symptoms, the higher the chances of having a tongue- or lip-tie. Call 205-419-4333 to set up a consult, or send us a message. It would be an honor to help you and your family. – Dr. Baxter
Bottle Feeding a Baby with Tongue Tie | Helping Babies with Tongue Tie
When we think of tongue tie, we often think of a nervous speaker stumbling over their words, or mixing up our words during a conversation. However, many people don’t realise that tongue tie is a medical condition found in some babies, also known in medical terminology as ankyloglossia. From how common it is, to the implications for your child, here’s everything you need to know about tongue tie in babies.
Tongue tie occurs when a baby’s frenulum (the strip of tissue connecting the tongue to the floor of the mouth) is shorter than usual. This is a relatively common condition, affecting between 4%-11% of babies, but studies have shown it’s actually slightly more common in baby boys. Tongue tie is present at birth, and some studies have shown that it can be hereditary (passed from parent to baby), so if you know that you suffered from this then make sure to tell your doctor or midwife.
Tongue tie is present at birth, and some studies have shown that it can be hereditary (passed from parent to baby), so if you know that you suffered from this then make sure to tell your doctor or midwife.
What Is Tongue Tie?
Tongue tie is where the little strip of skin which connects your baby’s tongue to the bottom of their mouth is shorter than that of most other babies. This is sometimes diagnosed during a newborn’s physical examination after birth. However, tongue tie can be hard to spot and it may not become obvious until your baby has problems feeding. Babies who are born with this condition have a restricted range of motion in their tongue and as they age, the way that they eat, speak and swallow can be affected. For some babies with tongue tie, they are unbothered by the condition but for those who incur problems they may need a simple surgical procedure for correction.
How To Tell If Your Baby Has Tongue Tie
Caregivers may notice that their baby with tongue tie or lip tie does not meet appropriate feeding milestones or has atypical feeding behaviours. Possible symptoms for this condition include:
Possible symptoms for this condition include:
- Difficulty latching and feeding when babies breastfeed or bottle feed; they lift their lower jaw during suckling, and use their top gum and the tip of the tongue (which lies on the lower gum) to keep the nipple / bottle in place. Tongue tie and lip tie can prevent the baby from taking enough breast tissue into the mouth to latch properly for feeding and the latch is often very shallow. Many babies may be able to latch but are unable to get the correct movements for sucking. Tongue tie may also result in a poor suck, breathing pattern or swallow.
- Mother experiences pain while nursing due to restricted and atypical tongue movements or improper latching. While the infant nurses, the mother may experience additional friction. This can lead to pain, bruising and bleeding.
- Frequent feeding patterns occur because during each feed, the infant consumes less milk than typical infants. Shortly after feeding, the infant may also show signs of hunger.

- Fatigue during or directly after feeding; the stressful experience of feeding means that the child expends more time and effort when feeding. During feedings, she might become irritated or fall asleep within one to two minutes.
- Dimpling of cheeks or clicking sounds when feeding; this is tongue tie-specific and is caused by atypical latching and sucking movements. There may also be jaw tremor here. Children with tongue tie are sometimes fussy and / or often pull away from the breast or bottle.
Some babies with tongue tie have no problems stemming from the condition at all; bottle fed babies are usually fine, as the teat from the bottle doesn’t require the same tongue action as breastfeeding. However, tongue tie can cause difficulty when breastfeeding, as the baby’s tongue is essential for proper suction to the breast.
A baby with tongue tie may end up compressing the breast tissue during feeding, which can lead to nipple soreness and damage. This inability to feed correctly can lead to low weight gain and fussiness. A tell-tale sign of a baby with tongue tie is a clicking sound when feeding, but this can also be a sign that you need support with the positioning and attachment of the baby at your breast, so check to make sure.
A tell-tale sign of a baby with tongue tie is a clicking sound when feeding, but this can also be a sign that you need support with the positioning and attachment of the baby at your breast, so check to make sure.
I was contacted by a very upset mum a couple of weeks ago who’s baby was extremely unhappy. Cheryl was at her wits’ end after several visits to her GP, Health Visitor and A & E with her daughter resulted in no clarity whatsoever as to what was going on with poor Jessica. Cheryl was desperate and wanted to try the babocush as soon as possible but I knew, after seeing photos of Jessica’s swollen tummy that it would take more than the babocush to sort out whatever was going on.
Want to find out more about tongue tie? Read Baby Jessica's Tongue Tie Story
How might an upper lip-tie impact feeding?
The impact of the upper lip-tie can vary - as the fullness of the upper lip can come into play. According to Melanie Potock, MA, CCC-SLP, you should consider these key points:
Breastfeeding and Bottle Feeding with Tongue Tie
- Breast – Inadequate latch: An infant has to flange his lips to establish ample suction and a proper seal of the nipple and surrounding tissue.
 It is important for babies to take in sufficient breast tissue to activate the suckling reflex, stimulating both the touch receptors in the lips and in the posterior oral cavity in order to obtain enough milk without fatigue. One (not always present) sign is a callus on the upper lip of the infant, immediately at midline.
It is important for babies to take in sufficient breast tissue to activate the suckling reflex, stimulating both the touch receptors in the lips and in the posterior oral cavity in order to obtain enough milk without fatigue. One (not always present) sign is a callus on the upper lip of the infant, immediately at midline.
- Bottle – Inadequate Seal: Since bottles and nipple shapes are interchangeable, and modifications can be made, a weak lip seal can be compensated. These compensatory measures are often adopted, however, because all attempts at breastfeeding have become too difficult, too exhausting, or result in poor weight gain ... and the culprit has been the upper lip-tie all along.
It can be difficult to tell if a baby has tongue tie, but if your baby struggles to extend his tongue out beyond his lips or if his tongue has a heart shaped appearance at the tip, it might be worthwhile getting him evaluated by a doctor.
Can Tongue Tie Go Away By Itself?
In most cases, the frenulum will recede by itself over the baby's first year, but in some cases a small surgical procedure may be required.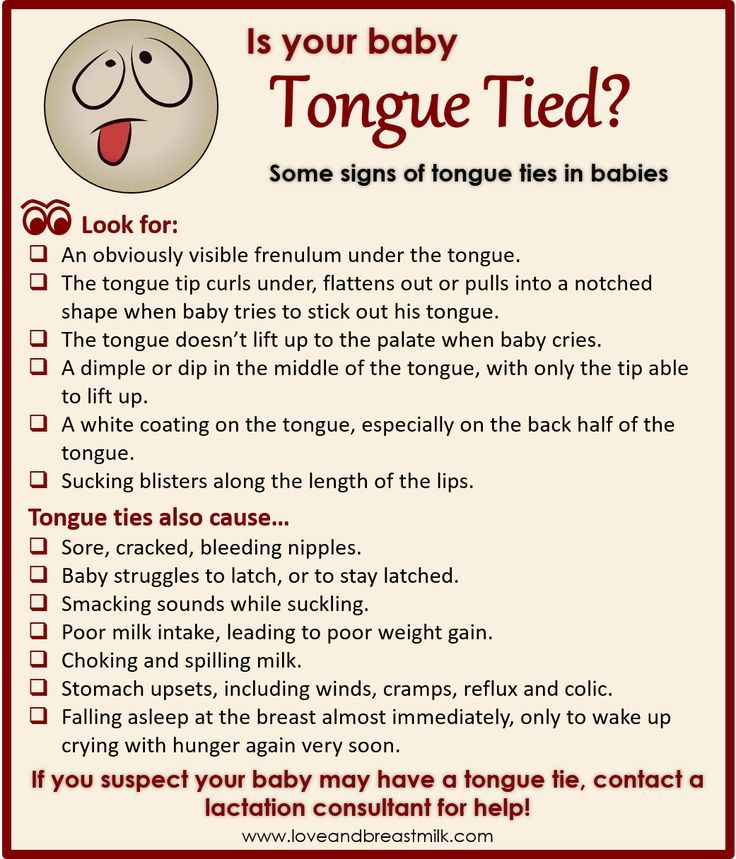 This is a very simple operation known as a frenotomy, which is a safe and uncomplicated procedure, usually performed in office at the GP’s surgery. No anaesthesia or stitches are needed; it’s a very easy and painless procedure.
This is a very simple operation known as a frenotomy, which is a safe and uncomplicated procedure, usually performed in office at the GP’s surgery. No anaesthesia or stitches are needed; it’s a very easy and painless procedure.
Tongue Tie In Babies: What You Need To Know
However, needing this procedure is rare, and only required in cases where the baby is struggling to feed or when mum is very uncomfortable. The baby can feed with ease straight after the procedure, and many mums note that comfort during breastfeeding improves almost instantly!
If your newborn is having problems feeding and showing symptoms of tongue tie then you should flag this up with your pediatrician. If you are nursing and experiencing pain, bruising or bleeding then you should definitely notify your doctor ASAP to get your baby evaluated to see if tongue tie is the cause. We hope you have found our tips helpful and please remember that if your baby is diagnosed with tongue tie there is nothing to be afraid of. Your baby’s tongue will either grow to a normal capacity during their first year or a simple painless surgical procedure may be required. The most important thing is that feeding time runs smoothly for both mom and baby, so don’t hesitate to contact a medical professional if you are experiencing difficulties.
Your baby’s tongue will either grow to a normal capacity during their first year or a simple painless surgical procedure may be required. The most important thing is that feeding time runs smoothly for both mom and baby, so don’t hesitate to contact a medical professional if you are experiencing difficulties.
Bottle feeding
When breastfeeding is not possible, or there is not enough breast milk and supplementary feeding is required, the use of infant milk formulas allows you to establish good nutrition for the baby.
The mixtures contain all the necessary nutrients, vitamins and trace elements. As a rule, they are well tolerated and digested, especially if the feeding process is properly established.
If you plan to bottle feed or supplement your baby with formula, our article will help you navigate the basic rules and intricacies of artificial feeding.
How to choose a teat (nozzle) for a bottle
Teats differ in composition (silicone, latex), shape and flow rate. While the shape of the nipple and the material are often chosen according to the preferences and needs of a particular baby, the flow rate is strictly determined by the age category.
While the shape of the nipple and the material are often chosen according to the preferences and needs of a particular baby, the flow rate is strictly determined by the age category.
Babies are fed from birth using the slowest flow nipple (these are usually labeled from 0 and one drop). Next, the teat flow rate in most bottle manufacturers increases at 3 months, 6 months, 12 months.
In order not to be mistaken, pay attention to the labeling and the age group for which the nipple to the bottle of the selected manufacturer is intended.
Whether such a nipple is right for you, you will also probably be able to understand during feeding.
- The baby should be able to comfortably grip the nipple and drink formula confidently (without too much effort).
- He should not choke/choke frequently.
- The mixture should flow well. If the mixture does not flow until you shake the bottle, the hole may be clogged with powder.
- If the mixture flows too much, check if the nipple is not torn.

How to treat the bottle
For newborn babies in the first months of life, it is recommended to sterilize the bottles before each feeding. Sterilization is the immersion of all feeding accessories (bottles, nipples, other parts) in boiling water for about 5 minutes to destroy pathogenic microflora.
You can choose any convenient method of sterilization: using a special device (sterilizer), in a microwave oven, dishwasher, ordinary boiling. Read more about how to properly sterilize bottles in our other article.
It is important to ensure that the baby bottle you use is made of safe plastic that can be heated. Some types of plastic release harmful chemicals when heated. As a rule, information about the possibility of sterilization and heating is indicated on the packaging. If there is no such information, it is not worth the risk. Use special baby bottles from well-known manufacturers. For example, a Dino Reno feeding bottle with nipple can be sterilized completely by any of the listed methods.
How to prepare formula and feed your baby
- Wash your hands with soap and water and dry with a dry towel.
- Remove the bottle and nipple from the sterilizer using the special holder (tweezers), assemble the bottle with the nipple, being careful not to touch the part that will go into the baby's mouth with your hands.
- Take boiled or special baby water heated to body temperature, dilute the mixture in the proportion indicated on the package.
- Use the special measuring spoon for preparation (it is included in each box with the mixture).
- Dilute the mixture strictly in the proportion indicated by the manufacturer. A thicker or thinner formula can harm your baby and cause stomach problems.
- Shake the bottle thoroughly to mix the contents evenly. Make sure that there are no lumps and clots left in the liquid and on the walls of the bottle.
- Check the temperature of the prepared mixture by dropping a little liquid on your wrist, it should not burn.

- Hold the bottle at the right angle. So that the tip of the nipple is always filled with milk and not with air.
- After feeding, hold the baby upright, let him burp the excess air.
- Feed your baby only fresh formula. According to the recommendations of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) of 2004, the reconstituted dry formula can be stored in a sealed bottle at a cool temperature for no more than 4 hours.
- If the mixture has cooled down, it can be warmed up with a special heater or in a water bath.
- If you are going on a long trip or outing, do not prepare the formula ahead of time. Better just pour the required amount of water into the bottle, and pour the right amount of the mixture into a separate container. Mix before feeding.
You will also find recommendations on the amount of formula to eat at a time, taking into account the age of the child, on the package. But some features of the baby's behavior can tell you whether he is full or not.
- If the baby pushes the nipple out of the bottle with his tongue and spit out the formula, he is probably already full and the feeding should be stopped.
- If the baby drank the contents of the bottle quickly and is crying, he may not have eaten enough and it is time to increase the portion.
- When your baby grows up, a feeding bottle with handles will come to your rescue. The child will be able to hold it himself and regulate the amount eaten.
Baby won't take bottle | Philips Avent
search support iconSearch Keywords
Home ›› What to do when your baby refuses a bottle
↑ Top
In most cases, switching a baby from breastfeeding to bottle feeding does not cause any problems. If your breastfed baby refuses a bottle, don't worry. This is a common occurrence in many babies who are used to breastfeeding. Obviously, this can create certain difficulties for moms, especially if you need to return to work in the near future.
3 Philips Avent products to help you bottle feed:
So why is your baby refusing the bottle and crying? There are many ways to quickly and easily teach a breastfed baby to a bottle. Here are important tips on what to do when your baby refuses a bottle.
Is the baby refusing the bottle? Take a step back
If your baby cries while bottle feeding, the first thing to do is to start over and rethink your feeding approach and technique. Try the following steps when bottle feeding your baby: [1]
- Lift and tilt your baby's head forward. Before inserting the pacifier into the baby's mouth, make sure that the baby's head is raised and tilted over his body to avoid choking: so that the baby does not choke and have the opportunity to burp during bottle feeding.
- Insert the pacifier. Bring the pacifier to the baby's lips and gently guide it into the baby's mouth. In no case do not try to press the nipple on the baby's lips and try to push it into his mouth.
 After touching the pacifier to the baby's lips, wait for the baby to open his mouth and take the pacifier.
After touching the pacifier to the baby's lips, wait for the baby to open his mouth and take the pacifier. - Hold the bottle at an angle. Tilt the bottle at an angle so that the nipple is only half full. So the child can eat at his own pace.
- Let the baby burp during and after feeding. It can be useful for a child to burp not only after feeding, but also approximately in the middle of the process. This will help reduce gas or tummy discomfort that your baby may experience from swallowing too much air.
- Stop in time, do not overfeed the baby. If the baby begins to turn his head away from the bottle or closes his mouth, then he is full and you need to stop feeding.
- Perhaps the flow of milk from the nipple is weak or too fast for the baby, so he is naughty and refuses the bottle. Try changing the nipple to a nipple with a different flow.
Other tips if your baby refuses a bottle
If you've followed the steps above and your baby still refuses a bottle, don't worry. There are other ways to help bottle feed your baby. Here are some simple tricks you can add to your bottle feeding process. [2]
There are other ways to help bottle feed your baby. Here are some simple tricks you can add to your bottle feeding process. [2]
1. Remind your child about mom.
Sometimes a child can be fed by someone other than his mother - dad, grandmother or, for example, a nanny. If your baby fusses while bottle feeding, try wrapping the bottle in something that smells like mommy, like a piece of clothing or some fabric. This will make it easier to feed the baby when the mother is not around.
2. Try to maintain body contact while bottle feeding.
Some babies need contact with their mother, so try bottle feeding while leaning against you. However, some babies are better at bottle feeding when they are in the exact opposite position than when they are breastfed. For example, there is a position with bent legs. Lay the child on your bent knees, facing you, pointing the child's legs towards your stomach. During feeding, the baby will be able to look at you and contact you in this way. If your baby refuses a bottle, experiment to see which works best.
During feeding, the baby will be able to look at you and contact you in this way. If your baby refuses a bottle, experiment to see which works best.
3. Move while feeding.
Sometimes all it takes to get your baby to take the bottle is a little wiggle or walk. The next time your baby starts crying while bottle feeding, try moving around a little rhythmically to calm him down.
4. Try changing the milk temperature.
If the baby still does not want to take the bottle, check if the milk in the bottle is too hot or too cold. Before feeding, put some warm breast milk on the inside of your wrist to check the temperature. Milk should be warm, but if it seemed hot to you, just place the bottle for a short while under a stream of cold water.
Choosing the right bottle for your baby If you plan to combine bottle feeding with breastfeeding, it is advisable to choose bottles with a nipple that will have a wide base as the bottle will grip closer to the breast.
 Also pay attention to the fact that the nipple is firm and flexible, the child must make an effort to drink from the bottle, as well as from the breast. Give preference to nipples with an anti-colic valve that vents air out of the bottle.
Also pay attention to the fact that the nipple is firm and flexible, the child must make an effort to drink from the bottle, as well as from the breast. Give preference to nipples with an anti-colic valve that vents air out of the bottle. Natural bottle allows you to combine breast and bottle feeding. 83.3% of babies switch from a natural bottle to breastfeeding and back.*
If you choose a bottle for artificial feeding, traditional bottles are fine, but it is desirable that the nipple is made of a hypoallergenic material, such as silicone, has an anti-colic valve and did not stick together when bottle fed. In case your baby spit up often, then use special bottles with anti-colic and anti-reflux valve, which reduces the risk of spitting up and colic.
Bottle with unique AirFree valve reduces the risk of colic, gas and spitting up. With this bottle, you can feed your baby in an upright or semi-upright position to reduce spitting up. Due to the fact that the nipple is filled with milk and not air during feeding, the baby does not swallow air, which means that feeding will be more comfortable.
Both bottles are indispensable if you want to breastfeed, bottle feed or just bottle feed your baby.
“My baby refuses to breastfeed but bottle feeds – help!”
Sometimes a baby gets used to bottle feeding and refuses to breastfeed. Therefore, it is important to use bottles that are suitable for combining breastfeeding with bottle feeding. If, nevertheless, you are faced with the fact that the child refuses to take the breast, try using silicone nipple covers to make the transition from the bottle to the breast and back more imperceptible.
Remember that if you want to combine breastfeeding and bottle feeding, it is worth waiting at least a month before offering a bottle, so that you are lactating and have time to get used to each other and develop a breastfeeding regimen.
Breastfeed and bottle feed your baby with pleasure
Remember that it takes a while for your baby to get used to bottle feeding. This is completely normal. If you have to go to work, be sure to set aside enough time to bottle train your baby beforehand.
This is completely normal. If you have to go to work, be sure to set aside enough time to bottle train your baby beforehand.
Remember that every child is different, so what works for one may not work for another. With a little time and patience, you will find out what works best for your baby when he refuses a bottle.
You will identify your child's unique needs. However, if your baby still refuses the bottle after all the steps above, check with your pediatrician.
Articles and tips from Philips Avent
Refs:
*O.L. Lukoyanova, T.E. Borovik, I.A. Belyaeva, G.V. Yatsyk; NTsZD RAMS; 1st Moscow State Medical University THEM. Sechenova, "The use of modern technological methods to maintain successful breastfeeding", Russian Federation, 02.10.2012
1 . 3 llli.org - The Baby Who Doesn't Nurse
llli.org - Introducing a Bottle to a Breastfed Baby
Baby+ app
Download the app and track your child's development and growth with trackers and save those special moments forever.