Effects of bottle feeding to a baby
Effects of breast-feeding duration, bottle-feeding duration and non-nutritive sucking habits on the occlusal characteristics of primary dentition | BMC Pediatrics
- Research article
- Open Access
- Published:
- Xiaoxian Chen1,
- Bin Xia2 &
- Lihong Ge2
BMC Pediatrics volume 15, Article number: 46 (2015) Cite this article
-
13k Accesses
-
35 Citations
-
4 Altmetric
-
Metrics details
Abstract
Background
Early transition from breastfeeding and non-nutritive sucking habits may be related to occlusofacial abnormalities as environmental factors. Previous studies have not taken into account the potential for interactions between feeding practice, non-nutritive sucking habits and occlusal traits. This study assessed the effects of breast-feeding duration, bottle-feeding duration and non-nutritive sucking habits on the occlusal characteristics of primary dentition in 3–6-year-old children in Peking city.
Methods
This cross sectional study was conducted via an examination of the occlusal characteristics of 734 children combined with a questionnaire completed by their parents/guardians. The examination was performed by a single, previously calibrated examiner and the following variables were evaluated: presence or absence of deep overbite, open bite, anterior crossbite, posterior crossbite, deep overjet, terminal plane relationship of the second primary molar, primary canine relationship, crowding and spacing. Univariate analysis and multiple logistic regressions were applied to analyze the associations.
Results
It was found that a short duration of breast-feeding (never or ≤6 months) was directly associated with posterior cross bite (OR = 3.13; 95% CI = 1.11–8.82; P = 0.031) and no maxillary space (OR = 1.63; 95% CI = 1.23–2.98; P = 0.038). In children breast-fed for ≤6 months, the probability of developing pacifier-sucking habits was 4 times that for those breast-fed for >6 months (OR = 4.21; 95% CI = 1.85–9.60; P = 0.0002). Children who were bottle-fed for over 18 months had a 1.45-fold higher risk of nonmesial step occlusion and a 1.43-fold higher risk of a class II canine relationship compared with those who were bottle-fed for up to 18 months. Non-nutritive sucking habits were also found to affect occlusion: A prolonged digit-sucking habit increased the probability of an anterior open bite, while a pacifier-sucking habit associated with excessive overjet and absence of lower arch developmental space.
Conclusion
Breastfeeding duration was shown to be associated with the prevalence of posterior crossbite, no maxillary space in the deciduous dentition and development of a pacifier-sucking habit. Children who had a digit-sucking habit were more likely to develop an open bite.
Children who had a digit-sucking habit were more likely to develop an open bite.
Peer Review reports
Background
Craniofacial growth and development are affected by functional stimuli such as sucking, chewing, swallowing and breathing [1]. Nutritive sucking, which includes breast-feeding and bottle-feeding and non-nutritive sucking (NNS), which includes pacifier and digit sucking, have been associated with growth and development of the maxillomandibular complex. Breast-feeding has been cited as one of the environmental factors responsible for correct development of dentofacial structures [2]. Recently, the biomechanics of milk extraction during breast-feeding have been investigated in detail. One group of researchers used an objective and dynamic analysis of ultrasound (US) videos acquired during breast-feeding to show that this complicated procedure requires coupling between the periodic motions of the infant’s jaws, the undulation of the tongue, and the breast-milk ejection reflex [3]. Another group found that extraction of milk during breast-feeding involved development of time-varying sub-atmospheric pressures within the infant’s oral cavity, and that vacuum pressures as low as −145 mmHg may be generated [4]. Conversely, absence or short duration of breast-feeding results in the child doing fewer oral exercises; this leads to underdevelopment of the muscles, incorrect posture of the lip and tongue, and the acquisition of harmful oral habits, all of which may be associated with dental malocclusions [2].
Another group found that extraction of milk during breast-feeding involved development of time-varying sub-atmospheric pressures within the infant’s oral cavity, and that vacuum pressures as low as −145 mmHg may be generated [4]. Conversely, absence or short duration of breast-feeding results in the child doing fewer oral exercises; this leads to underdevelopment of the muscles, incorrect posture of the lip and tongue, and the acquisition of harmful oral habits, all of which may be associated with dental malocclusions [2].
An absence or short duration of breast-feeding results in a longer duration of bottle-feeding. The sucking mechanism used during bottle-feeding is markedly different from that used during breast-feeding [1,5,6]. Compared with breast-feeding, bottle-feeding requires less forceful muscle action and thus, does not facilitate mandibular development to the same degree. This difference could potentially predispose those children who undergo prolonged bottle-feeding to malocclusion or other distinctive occlusion characteristics [1]. However, more evidence is needed to support this association.
However, more evidence is needed to support this association.
The empirical literature regarding the link between feeding practice and occlusal problems is far from unanimous in its conclusions. Some studies have reported that breast-feeding is a protective factor against malocclusion: Labbok and Hendershot have suggested that increased duration of breast-feeding is associated with a decline in the proportion of children with malocclusion [7], and Adamiak has linked it with a reduced need for orthodontic treatment [8]. In non-breast-fed children, the occurrence of an anterior open bite has been found to be significantly increased, demonstrating the beneficial influence of breast-feeding on dental occlusion [2]. However, other studies have indicated no relationship between the duration of breast-feeding in the first year of life and any dental arch or occlusal parameters [9]. Several reports have suggested that bottle-feeding may be responsible for the development of non-nutritive sucking habits and that these may be responsible for some forms of malocclusion [5,10,11]. Previous studies may not have taken account of confounding factors such as interactions between feeding practice, non-nutritive sucking habits and occlusal traits. Currently, the association between bottle-feeding and the incidence of occlusal alterations in the sagittal plane remains up for debate.
Previous studies may not have taken account of confounding factors such as interactions between feeding practice, non-nutritive sucking habits and occlusal traits. Currently, the association between bottle-feeding and the incidence of occlusal alterations in the sagittal plane remains up for debate.
In Peking, the proportion of children receiving at least four months of exclusive breast-feeding is reported to be as low as 39.2%, with an average weaning time of only 7.66 months [12]. Chinese studies on the feeding practice in childhood and their effects on occlusal characteristics, particularly in Peking city, are lacking. Therefore, the aim of this study was to assess, using multivariate analysis, the possible relationships between breastfeeding duration, bottle-feeding duration, non-nutritive sucking habits and dental arch characteristics in children aged 3–6 years old with primary dentition and attending state preschools in Peking, China.
Methods
Subjects and sample
The data for this cross-sectional study were obtained from annual oral health examinations in two daycare centers, located at Tsinghua University and Peking University, from April to May 2014. The sample size was calculated using the sample size formula and was based on the data from a previous prevalence study. In this study by Takuro, the prevalence of anterior crossbite was 5.7% in the children who were bottle-feeding at 24 months of age [13]. A desired accuracy of 10% and a significance level of 5% were adopted. We determined a minimum sample of 516 children. However, to compensate for possible non-responses, losses and failures to meet inclusion criteria, the study population was increased by 30% to 671 children.
The sample size was calculated using the sample size formula and was based on the data from a previous prevalence study. In this study by Takuro, the prevalence of anterior crossbite was 5.7% in the children who were bottle-feeding at 24 months of age [13]. A desired accuracy of 10% and a significance level of 5% were adopted. We determined a minimum sample of 516 children. However, to compensate for possible non-responses, losses and failures to meet inclusion criteria, the study population was increased by 30% to 671 children.
Questionnaire
This study was approved by the Research Ethics Committee at Peking University School and Hospital of Stomatology (Protocol No. PKUSSIRB-201414045). Written informed consent was obtained from parents or guardians of each subject.
Based on questionnaires designed by Charchut et al. [14] and answered by the parents/guardians, a retrospective investigation was made concerning the age and sex of the children, the parents’ schooling level, the feeding method (breast and/or bottle) used (including duration of use) for each 6-month period making up the first 36 months of the child’s life and finally, the child’s non-nutritive sucking habits during these time periods and at present. Feeding frequency was graded according to the following categories: method frequently used, used moderately, infrequently used, not used. Since a child might have received nutrition via both methods, the child was considered to be bottle-fed when the bottle score was higher than the breast score. A child was considered to exhibit non-nutritive sucking habits if he/she had been sucking an object (usually a digit or a pacifier) not related to feeding for more than the first year of life [5].
Feeding frequency was graded according to the following categories: method frequently used, used moderately, infrequently used, not used. Since a child might have received nutrition via both methods, the child was considered to be bottle-fed when the bottle score was higher than the breast score. A child was considered to exhibit non-nutritive sucking habits if he/she had been sucking an object (usually a digit or a pacifier) not related to feeding for more than the first year of life [5].
Inclusion criteria
The inclusion criteria were as follows: completely filled out questionnaire with no items missed, complete primary dentition without missing teeth, absence of extensive caries affecting the mesio-distal and occluso-gingival dimensions, absence of stainless steel crowns, absence of dental morphological anomalies, number and structure, absence of erupted or erupting permanent teeth, absence of trauma to the craniofacial complex, no history of orthodontic treatment and cooperation during the examination. The aim of all of the above criteria was to exclude factors that would compromise occlusal relationships or interfere with the examination results.
The aim of all of the above criteria was to exclude factors that would compromise occlusal relationships or interfere with the examination results.
Occlusal examination
The occlusal examinations were performed by a single examiner, a calibrated dentist who was blind to the questionnaire data. An intra-examiner reliability test was performed by examining 20 children at two different times, 2 weeks apart, and the Kappa value was calculated to be 85%. The clinical examinations were performed in the daycare center, using a mouth mirror and probe, under a suitably directed portable light source. The children lay down in a comfortable position, while the examiner was seated at 12 o’clock. The occlusal relationships were examined by direct visual inspection of the teeth at maximum mouth opening and then at maximum intercuspation. The primary second molar relationships and primary canine relationships were recorded while the patients’ primary teeth were closed at maximum intercuspation.
The following arch characteristics were recorded by a single examiner throughout the study using published definitions [15,16]:
- 1.
Overbite was graded according to coverage of the mandibular incisor by the most protruded fully erupted maxillary incisor and recorded as <1/2, or ≥1/2.
- 2.
Anterior open bite was recorded when one or more of the maxillary incisors occluded lingual to the mandibular incisors.
- 3.
Overjet or horizontal overlap was measured from the palatal surface of the mesial corner of the most protruded fully erupted maxillary incisor to the labial surface of the corresponding mandibular incisor. The degree of overjet was recorded in millimeters.
 In this study, an overjet of greater than 4 mm was considered an increased overjet.
In this study, an overjet of greater than 4 mm was considered an increased overjet. - 4.
Posterior crossbite was recorded when one or more of the maxillary primary canines or molars occluded lingual to the buccal cusps of the opposing mandibular teeth.
- 5.
The terminal relationship of the deciduous second molar were classified into three categories: flush terminal, where the distal surfaces of the upper and lower second primary molars are in the same vertical plane in a centric occlusion; distal step, where the distal surfaces of the lower primary second molar are in a posterior relationship to the distal surface of the upper second molars in centric occlusion; mesial step, the distal surfaces of the lower primary second molar are in an anterior relationship to the distal surface of the upper second molars in centric occlusion.
 Flush terminal and distal step relationships were combined as nonmesial step relationships.
Flush terminal and distal step relationships were combined as nonmesial step relationships. - 6.
Canine relationship was classified into three categories: class I, the tip of the maxillary primary canine tooth is in the same vertical plane as the distal surface of the mandibular primary canine; class II, the tip of the maxillary primary canine tooth is mesial to the distal surface of the mandibular primary canine; class III, the tip of the maxillary primary canine is distal to the distal surface of the mandibular primary canine.
- 7.
Spacing: If primate space or developmental space was present, spacing was noted.
- 8.
Crowding: When there are one or more teeth with disturbance of position or rotation, crowding was noted.

In determining the occlusal relationships of the primary second molar and primary canine, the occurrence of a similar occlusion on both sides was taken as a criterion. In the determination of the primary second molar relationship, if one side had a flush terminal plane while the other side had a distal or mesial step, which was noted as a distal or mesial terminal plane. In determining the canine relationship, if there was a class II or class III relationship on one side and class I on the other side, that was considered a class II or class III relationship. Children with a mesial step on one side and a distal step on the other were excluded from the study.
Data analysis
A descriptive analysis was carried out, in which the differences in the distribution of the study covariates in the dependent variable categories were assessed. The chi-square test was used to analyze the associations between breast-feeding duration, bottle-feeding duration, non-nutritive sucking and occlusal characteristics, at significance levels of P < 0. 05.
To measure the strength of the association and the relative chances of developing a particular occlusion characteristic, the odds ratio (OR) was calculated in a multivariate logistic regression analysis. Arch characteristics were the dependent variables, including anterior open bite, anterior crossbite, posterior crossbite, no maxillary space, mesial step, class II canine relationship, excessive overjet and space. Duration of breast-feeding was the main independent variable and was classified as either ‘never breast-fed/breast-fed until the age of six months’ or ‘breast-fed for more than six months’. The covariates were duration of bottle-feeding (≦18 months or >18 months), age (3–4, 4–5 or 5–6 years), sex, digit sucking (‘never had this habit/had this habit but stopped before the age of one’ or ‘had this habit for longer than one year’) and pacifier sucking (classification as for digit-sucking). A confidence interval of 95% was used as the criterion for statistical inference.
Results
Originally, we recruited 847 Chinese children from 3–6 years of age with complete primary dentition. Of these, 113 were excluded because their questionnaires were not completely/correctly filled in. Most questionnaires (93.2%) were completed by the parents. The remaining (6.8%) questionnaires were completed by the grandfather or grandmother.
The demographic and descriptive results for the subjects are presented in Table 1. Our sample included 734 children: 398 males and 336 females with a mean age of 4.48 ± 0.84. In most cases (73.4%), at least one of the parents had postgraduate qualifications. The incidence of NNS was 23.2%. The proportion of children who were breast-fed for 1–6 months was 27.1%, never breastfed was 13.8%. The proportion of children who were bottle-fed for over 18 months was 58.4%, bottle-fed for 6–18 months was 41.6%. None of children in the present study was bottle-fed for 0–6 months. In the first 6 months, 14.2% of infants were exclusively bottle-fed, 22. 9% were exclusively breast-fed while 62.9% were mixed-fed.
9% were exclusively breast-fed while 62.9% were mixed-fed.
Full size table
An increased percentage of posterior crossbite and no maxillary space (no upper arch space) were found in children who were breast-fed for less than 6 months (Table 2). No association was found between the duration of breast-feeding and the other examined occlusal characteristics. Analysis of the multivariate regression revealed that breast-feeding for no longer than 6 months seems to be the most important factor influencing posterior crossbite (OR = 3.13; 95% CI = 1.11–8.82; P = 0.031) and no maxillary space (OR = 1.63; 95% CI = 1.23–2.98; P = 0.038).
Table 2 Logistic regression analysis of the association between feeding duration and occlusal characteristicsFull size table
Bottle-feeding for longer than 18 months was associated with an increased prevalence of a nonmesial terminal plane (OR = 1. 45; 95% CI = 1.06–2.0; P = 0.018) and of a class II canine relationship (OR = 1.43; 95% CI = 1.03–2.0; P = 0.034), compared with children who were bottle-fed for between 6 and 18 months (Table 2). No association was found between duration of bottle-feeding and any other occlusal characteristics.
45; 95% CI = 1.06–2.0; P = 0.018) and of a class II canine relationship (OR = 1.43; 95% CI = 1.03–2.0; P = 0.034), compared with children who were bottle-fed for between 6 and 18 months (Table 2). No association was found between duration of bottle-feeding and any other occlusal characteristics.
The effects of the feeding method on non-nutritive sucking habits were quite different (Table 3). Our data indicated that children who were breast-fed for less than 6 months showed a higher probability of pacifier sucking (OR = 4.21; 95% CI = 1.85–9.60; P < 0.001). However, breast-feeding did not increase the probability of having a digit sucking habit (OR = 0.89; 95% CI = 0.61–1.30; P = 0.54). Bottle-feeding for longer than 18 months did not increase the prevalence of pacifier-sucking habit or digit-sucking habit.
Table 3 Feeding practice and non-nutritive sucking habitsFull size table
The prevalence of posterior crossbite and no maxillary space did not increase significantly in children with pacifier sucking or digit-sucking habits, when compared to children without these habits (Table 4). Similarly, there was no significant effect on the prevalence of a nonmesial terminal plane and a class II canine relationship. This suggests that NNS does not act in synergy with feeding practice to promote the development of the positive occlusal/arch characteristics mentioned above. A pacifier-sucking habit that lasted beyond one year of age was associated with excessive overjet (P = 0.01), absence of lower arch developmental space (P = 0.03). While a digit sucking habit that lasted beyond one year of age was associated with anterior open bite (P < 0.001).
Similarly, there was no significant effect on the prevalence of a nonmesial terminal plane and a class II canine relationship. This suggests that NNS does not act in synergy with feeding practice to promote the development of the positive occlusal/arch characteristics mentioned above. A pacifier-sucking habit that lasted beyond one year of age was associated with excessive overjet (P = 0.01), absence of lower arch developmental space (P = 0.03). While a digit sucking habit that lasted beyond one year of age was associated with anterior open bite (P < 0.001).
Full size table
Discussion
The literature provides no single criterion for malocclusion of primary dentition; therefore most occlusal characteristics were assessed in determining the relationship between malocclusion and feeding patterns. Our findings indicated that failure to breast-feed or breast-feeding for only a short period was associated with a higher prevalence of posterior crossbite and no maxillary space in the primary dentition. Sucking the breast places great demands on the perioral musculature. The constant repetitive effort promotes the correct development of these muscles, increasing their tone and ensuring that correct oral function is established. As a result, the duration of natural breast-feeding has a positive effect on the mobility of orofacial structures [17]. Early weaning may lead to an insufficient perioral muscular activity, which may cause negative consequences to swallowing, breathing and speaking, as well as malocclusion [18]. Warren et al. found that breast-feeding facilitates normal palate development and attenuates the formation of a deep, high-arched palate [10]. Viggiano et al. and Karjalainen et al. have reported that breast-feeding was a protective factor against development of posterior crossbite in the deciduous dentition [5,19]. Similarly, Kobayashi et al. reported that prolonged exclusive breast-feeding can strongly reduce the prevalence of posterior crossbite, and children who were breast-fed for more than 12 months had a 20-fold lower risk of posterior crossbite compared with children who were never breast-fed.
Sucking the breast places great demands on the perioral musculature. The constant repetitive effort promotes the correct development of these muscles, increasing their tone and ensuring that correct oral function is established. As a result, the duration of natural breast-feeding has a positive effect on the mobility of orofacial structures [17]. Early weaning may lead to an insufficient perioral muscular activity, which may cause negative consequences to swallowing, breathing and speaking, as well as malocclusion [18]. Warren et al. found that breast-feeding facilitates normal palate development and attenuates the formation of a deep, high-arched palate [10]. Viggiano et al. and Karjalainen et al. have reported that breast-feeding was a protective factor against development of posterior crossbite in the deciduous dentition [5,19]. Similarly, Kobayashi et al. reported that prolonged exclusive breast-feeding can strongly reduce the prevalence of posterior crossbite, and children who were breast-fed for more than 12 months had a 20-fold lower risk of posterior crossbite compared with children who were never breast-fed. Additionally, their risk was 5-fold lower than those who were breast-fed for between 6 and 12 months [20]. This evidence corroborates the findings of the present study. Although the absolute incidence of posterior crossbite was extremely low, its harmful effects on masticatory chewing cycle pattern and normal growth and development of the orofacial system were noticeable [21]. We suggest that early weaning may interfere with the normal development of alveolar ridges and the hard palate, and hence result in posterior crossbite, a lack of space or crowding in the upper arch.
Additionally, their risk was 5-fold lower than those who were breast-fed for between 6 and 12 months [20]. This evidence corroborates the findings of the present study. Although the absolute incidence of posterior crossbite was extremely low, its harmful effects on masticatory chewing cycle pattern and normal growth and development of the orofacial system were noticeable [21]. We suggest that early weaning may interfere with the normal development of alveolar ridges and the hard palate, and hence result in posterior crossbite, a lack of space or crowding in the upper arch.
The parents were very highly educated in our study and the rate of exclusive breast-feeding of children at 6 months of age was 22.9%. The corresponding rate in rural western China was 11.6 % [22], which was lower than our study. Scott et al. reviewed literature identifying factors associated with the initiation and duration of breastfeeding among Western women and found there was a strong and consistent association with demographic factors such as maternal age and level of education, there was a less consistent association with factors such as marital and socioeconomic status. [23]. However, Agboado et al. found there were no significant associations between breastfeeding cessation and marital status, mode of delivery, timing of breastfeeding initiation and socio-economic deprivation in Lancashire, UK [24]. These different finding highlights the fact that breastfeeding is multifactorial in nature and future programs aimed at promoting breastfeeding must take this into consideration.
[23]. However, Agboado et al. found there were no significant associations between breastfeeding cessation and marital status, mode of delivery, timing of breastfeeding initiation and socio-economic deprivation in Lancashire, UK [24]. These different finding highlights the fact that breastfeeding is multifactorial in nature and future programs aimed at promoting breastfeeding must take this into consideration.
Our study found a significant association between non-mesial step and bottle-feeding for over 18 months, compared to children who were bottle-fed for less than 18 months. A similar association was also found between the class II canine relationships and bottle-feeding. It is known that the terminal relationship of primary second molars seems to be the most important factor that could determine or influence the future relationship between the permanent molars and the subsequent development of occlusion. As Moyers and Waiuright reported, non-mesial step combined with a class II canine relationship increases the probability of developing Angle class II malocclusion in mixed dentition and permanent dentition [25]. Therefore, in many cases, early orthodontic intervention will be needed. Similarly, Nahás-Scocate et al. found that the older the child when bottle-feeding ceased (3–4 years old) and the shorter the breastfeeding duration (<3 months), the greater the chances of the child presenting distal step [26]. There are several theoretical mechanisms by which bottle-feeding might contribute to the development of malocclusion: (1) less muscle activity is necessary to extract milk from a bottle, resulting in decreased development of muscles involved in sucking, which may act as a functional matrix for inadequate mandibular growth; (2) The tongue acts only to control the milk outlet during bottle-feeding and bottle-fed children have an increased prevalence of abnormal swallowing patterns or tongue thrusting habits [27]; (3) over 60% of the children who were predominantly bottle-fed presented mouth breathing or mixed breathing, which may compromise occlusion [28]. Although Narbutyte et al. [29] found that the literature contains insufficient evidence to connect bottle-feeding with the development of skeletal malocclusions, the results of our study clearly showed that bottle-feeding may be related to abnormal maxillomandibular relationship via its inadequate provision of muscular stimulation.
Therefore, in many cases, early orthodontic intervention will be needed. Similarly, Nahás-Scocate et al. found that the older the child when bottle-feeding ceased (3–4 years old) and the shorter the breastfeeding duration (<3 months), the greater the chances of the child presenting distal step [26]. There are several theoretical mechanisms by which bottle-feeding might contribute to the development of malocclusion: (1) less muscle activity is necessary to extract milk from a bottle, resulting in decreased development of muscles involved in sucking, which may act as a functional matrix for inadequate mandibular growth; (2) The tongue acts only to control the milk outlet during bottle-feeding and bottle-fed children have an increased prevalence of abnormal swallowing patterns or tongue thrusting habits [27]; (3) over 60% of the children who were predominantly bottle-fed presented mouth breathing or mixed breathing, which may compromise occlusion [28]. Although Narbutyte et al. [29] found that the literature contains insufficient evidence to connect bottle-feeding with the development of skeletal malocclusions, the results of our study clearly showed that bottle-feeding may be related to abnormal maxillomandibular relationship via its inadequate provision of muscular stimulation. Nevertheless, the absolute OR value was low. The reason may be that the effects of bottle-feeding on occlusion were difficult to assess when bottle-feeding was concurrent with breast-feeding. In this study, 14.2% of infants were exclusively bottle-fed in the first 6 months while 62.9% were mixed-fed. This would weaken the effect of bottle-feeding on any specific type of malocclusion. Nevertheless, there was a weak trend associating bottle-feeding for over 18 months with inadequate mandibular growth.
Nevertheless, the absolute OR value was low. The reason may be that the effects of bottle-feeding on occlusion were difficult to assess when bottle-feeding was concurrent with breast-feeding. In this study, 14.2% of infants were exclusively bottle-fed in the first 6 months while 62.9% were mixed-fed. This would weaken the effect of bottle-feeding on any specific type of malocclusion. Nevertheless, there was a weak trend associating bottle-feeding for over 18 months with inadequate mandibular growth.
The incidences of pacifier sucking and digit sucking in the present study were 4.1% and 19.1%, respectively. Previous studies on non-nutritive sucking habits have shown a variation in prevalence between 20% and 87% at age 36 months [20,25,30]. Pacifier and digit sucking incidences have been reported to be 18.2% and 61.5% in Australia [31], 70.3% and 10% in Sweden, and 50% and 19% in Norway [32]. Most previous studies have reported much higher incidences of NNS compared with our study. This difference suggests that the incidence of NNS varies from one population to another and may be related to local culture and customs. The present study showed that 40.9% children were weaned early and this increased the prevalence of pacifier sucking by up to 4.1 fold, but it did not increase the prevalence of digit sucking. Theories that endeavor to explain this effect suggest that children who are naturally breast-fed satisfy their sucking needs along with their psychological and affective requirements through close, intimate contact with the mother during breast-feeding and thus have less need to suck a pacifier, digit or other object [33]. Conversely, non-nutritive sucking habits are developed when children satisfy their instinctive sucking urge by sucking their thumbs or by prolonged use of pacifiers. Nobuya et al. also reported that pacifier sucking was more prevalent in children with a short breast-feeding duration than in those with a normal feeding duration [34]. Luz et al.
This difference suggests that the incidence of NNS varies from one population to another and may be related to local culture and customs. The present study showed that 40.9% children were weaned early and this increased the prevalence of pacifier sucking by up to 4.1 fold, but it did not increase the prevalence of digit sucking. Theories that endeavor to explain this effect suggest that children who are naturally breast-fed satisfy their sucking needs along with their psychological and affective requirements through close, intimate contact with the mother during breast-feeding and thus have less need to suck a pacifier, digit or other object [33]. Conversely, non-nutritive sucking habits are developed when children satisfy their instinctive sucking urge by sucking their thumbs or by prolonged use of pacifiers. Nobuya et al. also reported that pacifier sucking was more prevalent in children with a short breast-feeding duration than in those with a normal feeding duration [34]. Luz et al. examined 249 children with mixed dentition and found statistically significant associations between short breast-feeding duration (<6 months) and non-nutritive sucking habits, and between non-nutritive sucking habits and class II malocclusions [35]. Montaldo et al. reported that children who underwent bottle- or complementary feeding showed a higher risk of acquiring non-nutritive sucking habits after the first year of life, and that this was associated with a greater risk of crossbite, open bite and class II molar relationships [36]. Surprisingly no correlation was found between bottle-feeding duration and pacifier sucking or between bottle-feeding duration and digit sucking. This can be explained by the fact that Chinese parents will usually select a milk bottle or other way to calm their infants rather than a pacifier.
examined 249 children with mixed dentition and found statistically significant associations between short breast-feeding duration (<6 months) and non-nutritive sucking habits, and between non-nutritive sucking habits and class II malocclusions [35]. Montaldo et al. reported that children who underwent bottle- or complementary feeding showed a higher risk of acquiring non-nutritive sucking habits after the first year of life, and that this was associated with a greater risk of crossbite, open bite and class II molar relationships [36]. Surprisingly no correlation was found between bottle-feeding duration and pacifier sucking or between bottle-feeding duration and digit sucking. This can be explained by the fact that Chinese parents will usually select a milk bottle or other way to calm their infants rather than a pacifier.
Different sucking habits are known to affect occlusion in different ways, and the disturbances found in the present study bear similarities to other findings elsewhere. In this study, a significant correlation was seen between pacifier sucking and excessive overjet as well as absence of lower arch developmental space. Pacifier sucking appeared to have an effect on the lower labial segment. Similar trends were reported by Warren et al., who found an association between prolonged pacifier sucking and a shorter intercanine width in the mandibular arch [10]. Aznar et al. found that a pacifier-sucking habit led to a significant reduction in the intercanine and intermolar mean width in the maxillary arch [37]. Melink et al. compared 30 children with a unilateral posterior crossbite and 30 children without a crossbite and found that the duration of pacifier habits were associated with posterior crossbites at the age of 4 or 5 years because of low tongue posture in the mouth [38]. These inconsistent findings can be explained by the force and frequency of muscle action involved in different pacifier sucking pattern or duration, which result in different effect on the development of the dental arches.
In this study, a significant correlation was seen between pacifier sucking and excessive overjet as well as absence of lower arch developmental space. Pacifier sucking appeared to have an effect on the lower labial segment. Similar trends were reported by Warren et al., who found an association between prolonged pacifier sucking and a shorter intercanine width in the mandibular arch [10]. Aznar et al. found that a pacifier-sucking habit led to a significant reduction in the intercanine and intermolar mean width in the maxillary arch [37]. Melink et al. compared 30 children with a unilateral posterior crossbite and 30 children without a crossbite and found that the duration of pacifier habits were associated with posterior crossbites at the age of 4 or 5 years because of low tongue posture in the mouth [38]. These inconsistent findings can be explained by the force and frequency of muscle action involved in different pacifier sucking pattern or duration, which result in different effect on the development of the dental arches. About half of the children in the present study were 3–4-years old and sucking a pacifier was rare in those beyond 3 years of age, so they may be too young to present an anterior open bite. Moreover, as was mentioned above, Chinese parents seldom use a pacifier to placate their infants, so the number with the habit was not large enough to show the most serious and representative effects.
About half of the children in the present study were 3–4-years old and sucking a pacifier was rare in those beyond 3 years of age, so they may be too young to present an anterior open bite. Moreover, as was mentioned above, Chinese parents seldom use a pacifier to placate their infants, so the number with the habit was not large enough to show the most serious and representative effects.
The finding that pacifier- and digit-sucking habits have different effects on occlusal traits has also been reported previously [10,39,40]. The present study found that digit sucking resulted in an increased prevalence of anterior crossbite and that it had a significant effect on the upper labial segment. Franco also found that for the first 3–4 years of life, the detrimental effect on occlusion is largely confined to the anterior segment [41]. The effect on development of dentofacial structures depends on the duration and frequency of the habit, the intensity of the sucking, the relationship of the dental arches and the direction and nature of the force exerted by the digit [42]. Generally, it is agreed that prolonged digit sucking is associated with increased overjet, greater maxillary arch depth, and greater prevalence of anterior open bite [37,40,41]. The present study pointed to the association between digit sucking and anterior open bite. This might be because a digit-sucking habit is difficult to give up and 62% of the children with the digit-sucking habit maintained it up to 3 years of age; this makes it more likely to impact occlusion and lead to vertical disturbances. Our study also showed that non-nutritive sucking habits were not associated with the prevalence of posterior crossbite and no maxillary space, nor did we find any effects on mesial step and class II canine relationship. We suggest that feeding practice may play a primary role in the development of posterior crossbite and no maxillary space. The evidence presented in this study suggests that children should be predominant breast-fed or exclusive breast-fed for no less than 6 months where possible and that parent should be more aware of the potentially deleterious effects of non-nutritive sucking habits on oral development.
Generally, it is agreed that prolonged digit sucking is associated with increased overjet, greater maxillary arch depth, and greater prevalence of anterior open bite [37,40,41]. The present study pointed to the association between digit sucking and anterior open bite. This might be because a digit-sucking habit is difficult to give up and 62% of the children with the digit-sucking habit maintained it up to 3 years of age; this makes it more likely to impact occlusion and lead to vertical disturbances. Our study also showed that non-nutritive sucking habits were not associated with the prevalence of posterior crossbite and no maxillary space, nor did we find any effects on mesial step and class II canine relationship. We suggest that feeding practice may play a primary role in the development of posterior crossbite and no maxillary space. The evidence presented in this study suggests that children should be predominant breast-fed or exclusive breast-fed for no less than 6 months where possible and that parent should be more aware of the potentially deleterious effects of non-nutritive sucking habits on oral development. From another direction, our finding fitted in with the WHO recommendation of breastfeeding exclusively for 6 months.
From another direction, our finding fitted in with the WHO recommendation of breastfeeding exclusively for 6 months.
However, there are some intrinsic limitations of cross section study and it was hard to take into consideration of the effect of heredity and other oral detrimental habits on malocclusion. The recall bias of the people who filled the questionnaire still existed, which might affect the accuracy of the duration of feeding practice. A future study with a larger sample size and isolating single variables is needed for a thorough understanding of the relationship between sucking and malocclusions.
Conclusions
The present study highlights the importance of taking into account multiple interactions between feeding practice, non-nutritive sucking habits and occlusal characteristics. The results suggest that even in the absence of non-nutritive sucking habits, failure to breast-feed for a sufficient length of time may negatively affect maxillary arch growth and may lead to malocclusion in the form of a posterior crossbite. Another negative consequence may be a prolonged pacifier-sucking habit, as we found that the probability of this increased 4-fold in children who were breast-fed for less than 6 months. In addition, we have found that increased bottle-feeding duration may contribute to inadequate mandibular development, and that non-nutritive sucking habits can be a dominant and deleterious factor in the development of occlusofacial problems.
Another negative consequence may be a prolonged pacifier-sucking habit, as we found that the probability of this increased 4-fold in children who were breast-fed for less than 6 months. In addition, we have found that increased bottle-feeding duration may contribute to inadequate mandibular development, and that non-nutritive sucking habits can be a dominant and deleterious factor in the development of occlusofacial problems.
References
Inoue N, Sakashita R, Kamegai T. Reduction of masseter muscle activity in bottle-fed babies. Early Hum Dev. 1995;42(3):185–93.
Article CAS PubMed Google Scholar
Romero CC, Scavone-Junior H, Garib DG, Cotrim-Ferreira FA, Ferreira RI. Breastfeeding and non-nutritive sucking patterns related to the prevalence of anterior open bite in primary dentition. J Appl Oral Sci. 2011;19(2):161–8.

Article PubMed PubMed Central Google Scholar
Elad D, Kozlovsky P, Blum O, Laine AF, Po MJ, Botzer E, et al. Biomechanics of milk extraction during breast-feeding. Proc Natl Acad Sci USA. 2014;111(14):5230–5.
Article CAS PubMed PubMed Central Google Scholar
Geddes DT, Kent JC, Mitoulas LR, Hartmann PE. Tongue movement and intra-oral vacuum in breastfeeding infants. Early Hum Dev. 2008;84(7):471–7.
Article PubMed Google Scholar
Viggiano D, Fasano D, Monaco G, Strohmenger L. Breast feeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child. 2004;89(12):1121–3.
Article CAS PubMed PubMed Central Google Scholar
Gomes CF, Trezza EM, Murade EC, Padovani CR. Surface electromyography of facial muscles during natural and artificial feeding of infants. J Pediatr (Rio J). 2006;82(2):103–9.
Article Google Scholar
Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227–32.
CAS PubMed Google Scholar
Adamiak E. [Prevalence of occlusal disorders in preschool children in rural areas in relation to various individual factors]. Czas Stomatol. 1981;34(5):551–5.
CAS PubMed Google Scholar
Warren JJ, Bishara SE. Duration of nutritive and nonnutritive sucking behaviors and their effects on the dental arches in the primary dentition.
 Am J Orthod Dentofacial Orthop. 2002;121(4):347–56.
Am J Orthod Dentofacial Orthop. 2002;121(4):347–56.Article PubMed Google Scholar
Warren JJ, Bishara SE, Steinbock KL, Yonezu T, Nowak AJ. Effects of oral habits’ duration on dental characteristics in the primary dentition. J Am Dent Assoc. 2001;132(12):1685–93. 1726.
Article CAS PubMed Google Scholar
Farsi NM, Salama FS. Sucking habits in Saudi children: prevalence, contributing factors and effects on the primary dentition. Pediatr Dent. 1997;19(1):28–33.
CAS PubMed Google Scholar
Zhang WK, Hao B, Wang LH. Situation of breastfeeding in ten cities in five provinces in China. Chin J Health Educ. 2004;20(1):14–6.
Google Scholar
Takuro Y, Kadoya M, Yakushiji M.
 Effects of prolonged breast- and bottle-feeding on occlusal characteristics in the primary dentition. Pediatr Dent J. 2005;2(15):176–9.
Effects of prolonged breast- and bottle-feeding on occlusal characteristics in the primary dentition. Pediatr Dent J. 2005;2(15):176–9.Google Scholar
Charchut SW, Allred EN, Needleman HL. The effects of infant feeding patterns on the occlusion of the primary dentition. J Dent Child (Chic). 2003;70(3):197–203.
Google Scholar
Farsi NM, Salama FS. Characteristics of primary dentition occlusion in a group of Saudi children. Int J Paediatr Dent. 1996;6(4):253–9.
Article CAS PubMed Google Scholar
Bhat SS, Rao HA, Hegde KS, Kumar BK. Characteristics of primary dentition occlusion in preschool children: an epidemiological study. Int J Clin Pediatr Dent. 2012;5(2):93–7.
PubMed PubMed Central Google Scholar
Medeiros AP, Ferreira JT, Felicio CM. Correlation between feeding methods, non-nutritive sucking and orofacial behaviors. Pro Fono. 2009;21(4):315–9.
Article PubMed Google Scholar
Neiva FC, Cattoni DM, Ramos JL, Issler H. Early weaning: implications to oral motor development. J Pediatr (Rio J). 2003;79(1):7–12.
Article Google Scholar
Karjalainen S, Ronning O, Lapinleimu H, Simell O. Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year-old Finnish children. Int J Paediatr Dent. 1999;9(3):169–73.
Article CAS PubMed Google Scholar
Kobayashi HM, Scavone HJ, Ferreira RI, Garib DG. Relationship between breastfeeding duration and prevalence of posterior crossbite in the deciduous dentition.
 Am J Orthod Dentofacial Orthop. 2010;137(1):54–8.
Am J Orthod Dentofacial Orthop. 2010;137(1):54–8.Article PubMed Google Scholar
Sever E, Marion L, Ovsenik M. Relationship between masticatory cycle morphology and unilateral crossbite in the primary dentition. Eur J Orthod. 2011;33(6):620–7.
Article PubMed Google Scholar
Qu P, Wang T, Liu F, Dang S, Zeng L, Yan H. Breast-feeding patterns of ethnic groups in rural western China. Public Health Nutr. 2015;16:1–8.
Google Scholar
Scott JA, Binns CW. Factors associated with the initiation and duration of breastfeeding: a review of the literature. Breastfeed Rev. 1999;7(1):5–16.
CAS PubMed Google Scholar
Agboado G, Michel E, Jackson E, Verma A. Factors associated with breastfeeding cessation in nursing mothers in a peer support programme in Eastern Lancashire.
 BMC Pediatr. 2010;10:3.
BMC Pediatr. 2010;10:3.Article PubMed PubMed Central Google Scholar
Moyers RE, Waiuright R. Skeletal contributions to occlusal development. In: McNamara Jr JA, editor. The Biology of Occlusal Development, monograph 7, Craniofacial Growth Series. Ann Arbor, MI: Univ of Michigan Press; 1977.
Google Scholar
Nahás-Scocate ACR, de Moura PX, Marinho RB, Alves AP, Ferreira RI, Guimarães FM. Association between infant feeding duration and the terminal relationships of the primary second molars. Bras J Oral Sci. 2011;10(2):140–5.
Google Scholar
Stanley EO, Lundeen DJ. Tongue thrust in breast fed and bottle-fed school children: a cross-cultural investigation. Int J Oral Myol. 1980;6(1):6–17.
CAS PubMed Google Scholar
Carrascoza KC, Possobon RF, Tomita LM, Moraes AB. Consequences of bottle-feeding to the oral facial development of initially breastfed children. J Pediatr (Rio J). 2006;82(5):395–7.
Article Google Scholar
Narbutyte I, Narbutyte A, Linkeviciene L. Relationship between breastfeeding, bottle-feeding and development of malocclusion. Stomatologija. 2013;15(3):67–72.
PubMed Google Scholar
Duncan K, McNamara C, Ireland AJ, Sandy JR. Sucking habits in childhood and the effects on the primary dentition: findings of the Avon Longitudinal Study of Pregnancy and Childhood. Int J Paediatr Dent. 2008;18(3):178–88.
Article PubMed Google Scholar
Cerny R. Thumb and finger sucking. Aust Dent J. 1981;26(3):167–71.
Article CAS PubMed Google Scholar
Larsson E, Ogaard B, Lindsten R. Dummy- and finger-sucking habits in young Swedish and Norwegian children. Scand J Dent Res. 1992;100(5):292–5.
CAS PubMed Google Scholar
Benkert KK. The effectiveness of orofacial myofunctional therapy in improving dental occlusion. Int J Orofacial Myology. 1997;23:35–46.
CAS PubMed Google Scholar
Ozawa N, Hamada S, Takekoshi F, Shinji H. A study on non-nutritive sucking habits in young Japanese children—Relationships among incidence, duration, malocclusion and nursing behavior. Pediatr Dent J. 2005;15(1):64–71.
Article Google Scholar
Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop.
 2006;130(4):531–4.
2006;130(4):531–4.Article PubMed Google Scholar
Montaldo L, Montaldo P, Cuccaro P, Caramico N, Minervini G. Effects of feeding on non-nutritive sucking habits and implications on occlusion in mixed dentition. Int J Paediatr Dent. 2011;21(1):68–73.
Article PubMed Google Scholar
Aznar T, Galan AF, Marin I, Dominguez A. Dental arch diameters and relationships to oral habits. Angle Orthod. 2006;76(3):441–5.
CAS PubMed Google Scholar
Melink S, Vagner MV, Hocevar-Boltezar I, Ovsenik M. Posterior crossbite in the deciduous dentition period, its relation with sucking habits, irregular orofacial functions, and otolaryngological findings. Am J Orthod Dentofacial Orthop. 2010;138(1):32–40.
Article PubMed Google Scholar
Ogaard B, Larsson E, Lindsten R. The effect of sucking habits, cohort, sex, intercanine arch widths, and breast or bottle feeding on posterior crossbite in Norwegian and Swedish 3-year-old children. Am J Orthod Dentofacial Orthop. 1994;106(2):161–6.
Article CAS PubMed Google Scholar
Kohler L, Holst K. Malocclusion and sucking habits of four-year-old children. Acta Paediatr Scand. 1973;62(4):373–9.
Article CAS PubMed Google Scholar
Franco VV, Gorritxo GB. Pacifier sucking habit and associated dental changes. Importance of early diagnosis. An Pediatr (Barc). 2012;77(6):374–80.
Article Google Scholar
Jyoti S, Pavanalakshmi GP. Nutritive and non-nutritive sucking habits – effect on the developing oro-facial complex; a review.
 Dent. 2014;4(3):1–4.
Dent. 2014;4(3):1–4.Google Scholar
Download references
Acknowledgements
We thank all the children and their families who participated in this study. The authors are very grateful for the valuable statistical assistance provided by Dr. Wang Shengfeng in School of Public Health, Peking University. We are grateful to the study participants, daycare centers of Tsinghua University and Peking University, whose participation made this study possible.
Author information
Author notes
Authors and Affiliations
Department of Pediatric Dentistry, First Dental Center, Peking University School and Hospital of Stomatology, Postal address: Jia No.37 Xishiku Street, Xicheng District, Beijing, 100034, China
Xiaoxian Chen
Department of Pediatric Dentistry, Peking University School and Hospital of Stomatology, Beijing, 100081, China
Bin Xia & Lihong Ge
Authors
- Xiaoxian Chen
View author publications
You can also search for this author in PubMed Google Scholar
- Bin Xia
View author publications
You can also search for this author in PubMed Google Scholar
- Lihong Ge
View author publications
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Lihong Ge.
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
XC contributed to the implementation of the study, analysis and writing of this manuscript. BX supervised the development of the manuscript and contributed to the analysis and writing. LG contributed to the study design, initiated the study, and provided comments on the manuscript. All authors read and approved the final manuscript.
Xiaoxian Chen and Bin Xia contributed equally to this work.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made.
The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit https://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and Permissions
About this article
The Risks of Not Breastfeeding for Mothers and Infants
1. Ip S, Chung M, Raman G, et al. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep) 2007;153:1–186. [PMC free article] [PubMed] [Google Scholar]
2. American College of Obstetrics and Gynecology, authors. Special Report from ACOG. Breastfeeding: maternal and infant aspects. ACOG Clinical Review. 2007;12(suppl):1S–16S. [Google Scholar]
ACOG Clinical Review. 2007;12(suppl):1S–16S. [Google Scholar]
3. Gartner LM, Morton J, Lawrence RA, et al. Breastfeeding and the use of human milk. Pediatrics. 2005;115:496–506. [PubMed] [Google Scholar]
4. American Academy of Family Physicians, authors. Breastfeeding, family physicians supporting (Position Paper) [Accessed June 10, 2009]. http://www.aafp.org/online/en/home/policy/policies/b/breastfeedingpositionpaper.html.
5. Centers for Disease Control and Prevention, authors. Breastfeeding among U.S. children born 1999–2006, CDC National Immunization Survey. [Accessed June 10, 2009]. http://www.cdc.gov/breastfeeding/data/NIS_data/index.htm.
6. Centers for Disease Control and Prevention, authors. Breastfeeding-related maternity practices at hospitals and birth centers-United States, 2007. MMWR Morb Mortal Wkly Rep. 2008;57:621–625. [PubMed] [Google Scholar]
7. Wiessinger D. Watch your language! J Hum Lact. 1996;12:1–4. [PubMed] [Google Scholar]
8. Berry NJ, Gribble KD. Breast is no longer best: promoting normal infant feeding. Matern Child Nutr. 2008;4:74–79. [PMC free article] [PubMed] [Google Scholar]
Berry NJ, Gribble KD. Breast is no longer best: promoting normal infant feeding. Matern Child Nutr. 2008;4:74–79. [PMC free article] [PubMed] [Google Scholar]
9. Cattaneo A. The benefits of breastfeeding or the harm of formula feeding? J Paediatr Child Health. 2008;44:1–2. [PubMed] [Google Scholar]
10. Li R, Rock VJ, Grummer-Strawn L. Changes in public attitudes toward breastfeeding in the United States, 1999–2003. J Am Diet Assoc. 2007;107:122–127. [PubMed] [Google Scholar]
11. Hamosh M. Bioactive factors in human milk. Pediatr Clin North Am. 2001;48:69–86. [PubMed] [Google Scholar]
12. Nathavitharana KA, Catty D, McNeish AS. IgA antibodies in human milk: epidemiological markers of previous infections? Arch Dis Child Fetal Neonatal Ed. 1994;71:F192–F197. [PMC free article] [PubMed] [Google Scholar]
13. Peterson JA, Patton S, Hamosh M. Glycoproteins of the human milk fat globule in the protection of the breast-fed infant against infections. Biol Neonate. 1998;74:143–162. [PubMed] [Google Scholar]
[PubMed] [Google Scholar]
14. Hamosh M. Protective function of proteins and lipids in human milk. Biol Neonate. 1998;74:163–176. [PubMed] [Google Scholar]
15. Bachrach VR, Schwarz E, Bachrach LR. Breastfeeding and the risk of hospitalization for respiratory disease in infancy: a meta-analysis. Arch Pediatr Adolesc Med. 2003;157:237–243. [PubMed] [Google Scholar]
16. Chien PF, Howie PW. Breast milk and the risk of opportunistic infection in infancy in industrialized and non-industrialized settings. Adv Nutr Res. 2001;10:69–104. [PubMed] [Google Scholar]
17. Kramer MS, Chalmers B, Hodnett ED, et al. Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA. 2001;285:413–420. [PubMed] [Google Scholar]
18. Holman RC, Stoll BJ, Curns AT, et al. Necrotising enterocolitis hospitalisations among neonates in the United States. Paediatr Perinat Epidemiol. 2006;20:498–506. [PubMed] [Google Scholar]
19. Horta BL, Bahl R, Martinés JC, et al. Evidence on the long-term effects of breastfeeding: systematic review and meta-analyses. Geneva: World Health Organization; 2007. pp. 1–57. [Google Scholar]
Evidence on the long-term effects of breastfeeding: systematic review and meta-analyses. Geneva: World Health Organization; 2007. pp. 1–57. [Google Scholar]
20. Harder T, Bergmann R, Kallischnigg G, et al. Duration of breastfeeding and risk of overweight: a meta-analysis. Am J Epidemiol. 2005;162:397–403. [PubMed] [Google Scholar]
21. Owen CG, Martin RM, Whincup PH, et al. Effect of infant feeding on the risk of obesity across the life course: a quantitative review of published evidence. Pediatrics. 2005;115:1367–1377. [PubMed] [Google Scholar]
22. Arenz S, Rückerl R, Koletzko B, et al. Breastfeeding and childhood obesity-a systematic review. Int J Obes Relat Metab Disord. 2004;28:1247–1256. [PubMed] [Google Scholar]
23. Owen CG, Martin RM, Whincup PH, et al. Does breastfeeding influence risk of type 2 diabetes in later life? A quantitative analysis of published evidence. Am J Clin Nutr. 2006;84:1043–1054. [PubMed] [Google Scholar]
24. Owen CG, Whincup PH, Gilg JA, et al. Effect of breast feeding in infancy on blood pressure in later life: systematic review and meta-analysis. BMJ. 2003;327:1189–1195. [PMC free article] [PubMed] [Google Scholar]
Effect of breast feeding in infancy on blood pressure in later life: systematic review and meta-analysis. BMJ. 2003;327:1189–1195. [PMC free article] [PubMed] [Google Scholar]
25. Martin RM, Gunnell D, Smith GD. Breastfeeding in infancy and blood pressure in later life: systematic review and meta-analysis. Am J Epidemiol. 2005;161:15–26. [PubMed] [Google Scholar]
26. Owen CG, Whincup PH, Odoki K, et al. Infant feeding and blood cholesterol: a study in adolescents and a systematic review. Pediatrics. 2002;110:597–608. [PubMed] [Google Scholar]
27. Agostoni C. Ghrelin, leptin and the neurometabolic axis of breastfed and formula-fed infants. Acta Paediatr. 2005;94:523–525. [PubMed] [Google Scholar]
28. Aydin S, Ozkan Y, Erman F, et al. Presence of obestatin in breast milk: relationship among obestatin, ghrelin, and leptin in lactating women. Nutrition. 2008;24:689–693. [PubMed] [Google Scholar]
29. Anderson JW, Johnstone BM, Remley DT. Breast-feeding and cognitive development: a meta-analysis. Am J Clin Nutr. 1999;70:525–535. [PubMed] [Google Scholar]
Am J Clin Nutr. 1999;70:525–535. [PubMed] [Google Scholar]
30. Drane DL, Logemann JA. A critical evaluation of the evidence on the association between type of infant feeding and cognitive development. Paediatr Perinat Epidemiol. 2000;14:349–356. [PubMed] [Google Scholar]
31. Jain A, Concato J, Leventhal JM. How good is the evidence linking breastfeeding and intelligence? Pediatrics. 2002;109:1044–1053. [PubMed] [Google Scholar]
32. Dewey KG, Cohen RJ, Brown KH, et al. Effects of exclusive breastfeeding for four versus six months on maternal nutritional status and infant motor development: results of two randomized trials in Honduras. J Nutr. 2001;131:262–267. [PubMed] [Google Scholar]
33. Kramer MS, Aboud F, Mironova E, et al. Breast-feeding and child cognitive development: new evidence from a large randomized trial. Arch Gen Psychiatry. 2008;65:578–584. [PubMed] [Google Scholar]
34. Simmer K, Patole S, Rao SC. Longchain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database Syst Rev. 2008;1 CD00037. [PubMed] [Google Scholar]
Cochrane Database Syst Rev. 2008;1 CD00037. [PubMed] [Google Scholar]
35. McVea KL, Turner PD, Peppler DK. The role of breastfeeding in sudden infant death syndrome. J Hum Lact. 2000;16:13–20. [PubMed] [Google Scholar]
36. American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome, authors. The changing concept of sudden infant death syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics. 2005;116:1245–1255. [PubMed] [Google Scholar]
37. Chen A, Rogan WJ. Breastfeeding and the risk of postneonatal death in the United States. Pediatrics. 2004;113:e435–e439. [PubMed] [Google Scholar]
38. Penders J, Thijs C, Vink C, et al. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics. 2006;118:511–521. [PubMed] [Google Scholar]
39. Forchielli ML, Walker WA. The role of gut-associated lymphoid tissues and mucosal defence. Br J Nutr. 2005;93(suppl 1):S41–S48. [PubMed] [Google Scholar]
2005;93(suppl 1):S41–S48. [PubMed] [Google Scholar]
40. Indrio F, Ladisa G, Mautone A, et al. Effect of a fermented formula on thymus size and stool pH in healthy term infants. Pediatr Res. 2007;62:98–100. [PubMed] [Google Scholar]
41. Gdalevich M, Mimouni D, Mimouni M. Breast-feeding and the risk of bronchial asthma in childhood: a systematic review with meta-analysis of prospective studies. J Pediatr. 2001;139:261–266. [PubMed] [Google Scholar]
42. Gdalevich M, Mimouni D, David M, et al. Breast-feeding and the onset of atopic dermatitis in childhood: a systematic review and meta-analysis of prospective studies. J Am Acad Dermatol. 2001;45:520–527. [PubMed] [Google Scholar]
43. Kostraba JN, Cruickshanks KJ, Lawler-Heavner J, et al. Early exposure to cow’s milk and solid foods in infancy, genetic predisposition, and risk of IDDM. Diabetes. 1993;42:288–295. [PubMed] [Google Scholar]
44. Norris JM, Scott FW. A meta-analysis of infant diet and insulin-dependent diabetes mellitus: do biases play a role? Epidemiology. 1996;7:87–92. [PubMed] [Google Scholar]
1996;7:87–92. [PubMed] [Google Scholar]
45. Gerstein HC. Cow’s milk exposure and type I diabetes mellitus. A critical overview of the clinical literature. Diabetes Care. 1994;17:13–19. [PubMed] [Google Scholar]
46. Akerblom HK, Virtanen SM, Ilonen J, et al. Dietary manipulation of beta cell autoimmunity in infants at increased risk of type 1 diabetes: a pilot study. Diabetologia. 2005;48:829–837. [PubMed] [Google Scholar]
47. Greaves MF. Speculations on the cause of childhood acute lymphoblastic leukemia. Leukemia. 1988;2:120–125. [PubMed] [Google Scholar]
48. Kwan ML, Buffler PA, Abrams B, et al. Breast-feeding and the risk of childhood leukemia: a meta-analysis. Public Health Rep. 2004;119:521–535. [PMC free article] [PubMed] [Google Scholar]
49. Kvale G, Heuch I. Lactation and cancer risk: is there a relation specific to breast cancer? J Epidemiol Community Health. 1988;42:30–37. [PMC free article] [PubMed] [Google Scholar]
50. Michels KB, Willet WC, Rosner BA, et al. Prospective assessment of breastfeeding and breast cancer incidence among 89,887 women. Lancet. 1996;347:431–436. [PubMed] [Google Scholar]
Prospective assessment of breastfeeding and breast cancer incidence among 89,887 women. Lancet. 1996;347:431–436. [PubMed] [Google Scholar]
51. Bernier MO, Plu-Bureau G, Bossard N, et al. Breastfeeding and risk of breast cancer: a meta-analysis of published studies. Hum Reprod Update. 2000;6:374–386. [PubMed] [Google Scholar]
52. Lipworth L, Bailey LR, Trichopoulos D. History of breast-feeding in relation to breast cancer risk: a review of the epidemiologic literature. J Natl Cancer Inst. 2000;92:302–312. [PubMed] [Google Scholar]
53. London SJ, Colditz GA, Stampfer MJ, et al. Lactation and risk of breast cancer in a cohort of US women. Am J Epidemiol. 1990;132:17–26. [PubMed] [Google Scholar]
54. Tryggvadóttir L, Tulinius H, Eyfjord JE, et al. Breastfeeding and reduced risk of breast cancer in an Icelandic cohort study. Am J Epidemiol. 2001;154:37–42. [PubMed] [Google Scholar]
55. Lee SY, Kim MT, Kim SW, et al. Effect of lifetime lactation on breast cancer risk: a Korean women’s cohort study. Int J Cancer. 2003;105:390–393. [PubMed] [Google Scholar]
Int J Cancer. 2003;105:390–393. [PubMed] [Google Scholar]
56. Collaborative Group on Hormonal Factors in Breast Cancer, authors. Breast cancer and breastfeeding: collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including50302 women with breast cancer and 96973 women without the disease. Lancet. 2002;360:187–195. [PubMed] [Google Scholar]
57. Stuebe AM, Willet WC, Xue F, et al. Lactation and incidence of premenopausal breast cancer: a longitudinal study. Arch Intern Med. 2009;169:1364–1371. [PMC free article] [PubMed] [Google Scholar]
58. Danforth KN, Tworoger SS, Hecht JL, et al. Breastfeeding and risk of ovarian cancer in two prospective cohorts. Cancer Causes Control. 2007;18:517–523. [PubMed] [Google Scholar]
59. Cramer DW, Titus-Ernstoff L, McKolanis JR, et al. Conditions associated with antibodies against the tumor-associated antigen MUC1 and their relationship to risk for ovarian cancer. Cancer Epidemiol Biomarkers Prev. 2005;14:1125–1131. [PubMed] [Google Scholar]
2005;14:1125–1131. [PubMed] [Google Scholar]
60. Stuebe AM, Rich-Edwards JW. The reset hypothesis: lactation and maternal metabolism. Am J Perinatol. 2009;26:81–88. [PMC free article] [PubMed] [Google Scholar]
61. Dewey KG, Heinig MJ, Nommsen LA. Maternal weight-loss patterns during prolonged lactation. Am J Clin Nutr. 1993;58:162–166. [PubMed] [Google Scholar]
62. Stuebe AM, Rich-Edwards JW, Willett WC, et al. Duration of lactation and incidence of type 2 diabetes. JAMA. 2005;294:2601–2610. [PubMed] [Google Scholar]
63. Stuebe AM, Michels KB, Willett WC, et al. Duration of lactation and incidence of myocardial infarction in middle to late adulthood. Am J Obstet Gynecol. 2009;200:138.e1–138.e8. [PMC free article] [PubMed] [Google Scholar]
64. Ram KT, Bobby P, Hailpern SM, et al. Duration of lactation is associated with lower prevalence of the metabolic syndrome in midlife-SWAN, the study of women’s health across the nation. Am J Obstet Gynecol. 2008;198:268. e1–268.e6. [PMC free article] [PubMed] [Google Scholar]
e1–268.e6. [PMC free article] [PubMed] [Google Scholar]
65. Schwarz EB, Ray RM, Stuebe AM, et al. Duration of lactation and risk factors for maternal cardiovascular disease. Obstet Gynecol. 2009;113:974–982. [PMC free article] [PubMed] [Google Scholar]
66. Taveras EM, Li R, Grummer-Strawn L, et al. Mothers’ and clinicians’ perspectives on breastfeeding counseling during routine preventive visits. Pediatrics. 2004;113:e405–e411. [PubMed] [Google Scholar]
67. DiGirolamo AM, Grummer-Strawn LM, Fein SB. Do perceived attitudes of physicians and hospital staff affect breastfeeding decisions? Birth. 2003;30:94–100. [PubMed] [Google Scholar]
68. Hartley BM, O’Connor ME. Evaluation of the ‘Best Start’ breast-feeding education program. Arch Pediatr Adolesc Med. 1996;150:868–871. [PubMed] [Google Scholar]
69. Howard C, Howard F, Lawrence R, et al. Office prenatal formula advertising and its effect on breast-feeding patterns. Obstet Gynecol. 2000;95:296–303. [PubMed] [Google Scholar]
70.![]() Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia. 2007;12:211–221. [PubMed] [Google Scholar]
Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia. 2007;12:211–221. [PubMed] [Google Scholar]
71. Newton M, Newton NR. The let-down reflex in human lactation. J Pediatr. 1948;33:698–704. [PubMed] [Google Scholar]
72. Cregan MD, Mitoulas LR, Hartmann PE. Milk prolactin, feed volume and duration between feeds in women breastfeeding their full-term infants over a 24 h period. Exp Physiol. 2002;87:207–214. [PubMed] [Google Scholar]
73. Keefe MR. The impact of infant rooming-in on maternal sleep at night. J Obstet Gynecol Neonatal Nurs. 1988;17:122–126. [PubMed] [Google Scholar]
74. Philipp BL, Merewood A. The Baby-Friendly way: the best breastfeeding start. Pediatr Clin North Am. 2004;51:761–783. [PubMed] [Google Scholar]
75. Moore ER, Anderson GC, Bergman N. Early skinto-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2007;4 CD003519. [PubMed] [Google Scholar]
Artificial feeding of babies | Bebbo
Submitted by Ilya Danshyn on Wed, 12/08/2021 - 18:40
Sometimes the baby cannot breastfeed, so you have to express milk and bottle feed the baby. Some babies are formula fed because for some reason breastfeeding is not possible, or lactation has stopped prematurely, or you have chosen to formula feed your baby.
Some babies are formula fed because for some reason breastfeeding is not possible, or lactation has stopped prematurely, or you have chosen to formula feed your baby.
- Make sure that the rate of milk flow from the bottle through the nipple is appropriate for the baby.
- To check this, turn the filled bottle upside down.
- Milk should drip quickly, not squirt. If you have to shake the bottle hard to make the milk drip, it means that the nipple is not providing the normal intensity of feeding.
- The baby can fall asleep even before he has eaten everything from the bottle.
- It is normal for a small amount of milk to leak from the corners of the mouth; it will stop when the child gets older.
- If you can't find the perfect nipple, choose the one that produces the most milk; it's okay if you have to go through how many nipples before you find one that's right for you and your baby.
How to bottle feed your baby
- Sit back and hold your baby in your arms, gently but firmly.
 It is better for the baby to be in a more upright position, similar to the position when breastfeeding.
It is better for the baby to be in a more upright position, similar to the position when breastfeeding. - Place the pacifier between the baby's lips; he will open his mouth and start sucking.
- Hold the bottle at an angle so that the nipple and mouth of the bottle are constantly filled with milk; this will prevent the child from swallowing air.
- When the baby stops actively sucking or has eaten half the milk from the bottle, carefully remove the bottle and check if he wants to burp; after that, you can continue feeding.
- Change the position of the baby during feeding or at least at each feeding; this allows even stimulation of the baby's sensations on both sides of the body and prevents positional deformation of the head.
How much milk does a baby need?
- The number of meals and the amount of milk is determined by the baby! Different babies require different amounts of breast milk or formula. Feeding time is not always evenly distributed over the time of day, sometimes children eat more during the day, followed by a long night break.

- If you are formula feeding, check the chart on the box. Of course, the recommended serving size for your age will only serve as a guideline and may not necessarily be appropriate for your child.
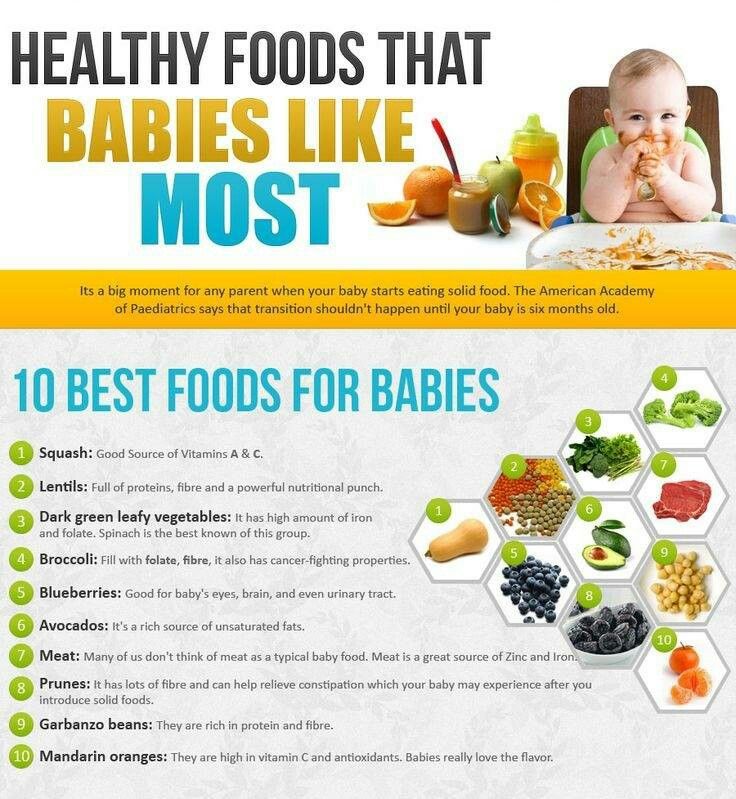
- When a baby begins to receive complementary foods, as the amount of solid food increases, the baby's need for milk decreases.
- The amount of formula your baby eats will decrease when he switches from bottle to cup.
- By the age of 12 months, when a baby can switch to cow's milk, he usually receives 500-600 ml of breast milk or formula per day.
Some babies never eat the recommended amount of milk for their age and height. For some, this "recommended" volume is not enough. At least six wet diapers during the day, constant but not excessive weight gain, a healthy and active child - all this indicates that everything is in order. If you are concerned that your baby is not getting enough milk or formula, contact your doctor.
Responsive feeding from the bottle in accordance with the needs of the child
- Feed the baby when he shows that he is hungry and not on the schedule, follow his signals.

- Do not feed the baby if he is not hungry, just because the formula is already prepared - this can lead to overfeeding the baby.
- When a baby is bottle fed, there is no difference between foremilk and hindmilk that affects the feeling of fullness in a breastfed baby.
- The child is often held so that the milk simply flows into the mouth rather than actively suckling; in this case, he eats too much milk too quickly.
- During feeding, watch the baby for signs of satiety - he turns away from the bottle, sucks lazily - and stop feeding in time.
- Hold the baby close to you during feeding, hug and talk to him; it stimulates growth and development and also strengthens the bond between you and your child.
- The baby did not eat everything from the bottle and fell asleep while eating.
- Don't worry if the child hasn't eaten everything; he knows how much formula or breast milk he needs.
- If the child falls asleep while eating, put him on your shoulder, stroke or pat him on the back and legs; Changing diapers is also an effective way to wake up a baby.

- Wait until the baby is awake before giving him any leftover milk.
Always empty the remaining milk from the bottle if more than an hour has passed!
Night feeding
- Every baby is different. Some wean from night feeding at four months, and some at two years. From the 6th month of life, healthy children no longer need night feeding. Now it's just a habit that gets harder to change the older the child gets.
- If a baby is bottle fed, this is the last age to stop eating at night! Do not replace milk with juices or other sweetened drinks to protect your child's teeth from cavities.
- If your baby drinks 60 ml or less of milk during the night, you can simply stop feeding at night and calm the baby as you usually do, and then put him back in the crib to fall asleep on his own.
- If your baby eats more than 60 ml every night, gradually reduce the amount of milk over 5-7 nights and lull the baby as you normally do.

Risks of bottle feeding in bed
- If your child gets used to falling asleep with a bottle in bed, it will be more difficult for him to learn to calm down or fall asleep on his own.
- If a child falls asleep with a bottle in his mouth, there is a risk of choking on milk and suffocation. Babies are not as light sleepers as older children and adults, and do not wake up if something prevents them from breathing.
- A mixture left in the mouth during sleep leads to dental caries.
- When a child drinks from a bottle lying down, the risk of ear inflammation increases.
Australian Article
On
Cover Image
Image
© UNICEF/UN0158032/Voronin
KeyWords
Breast Feed
Category
Power
Child Age
1st month
2nd month
3-4 months
003
There is a wide variety of infant formula available. Most of them are based on cow's milk. However, never use regular cow's milk for artificial feeding. Although cow's milk is taken as the basis, it is significantly modified to be suitable for an infant. It undergoes heat treatment so that its proteins are better digested. Milk sugar (lactose) is added so that its concentration is the same as in breast milk, milk fat is eliminated and replaced with vegetable oils and animal fats that are easier for the baby to digest.
Most of them are based on cow's milk. However, never use regular cow's milk for artificial feeding. Although cow's milk is taken as the basis, it is significantly modified to be suitable for an infant. It undergoes heat treatment so that its proteins are better digested. Milk sugar (lactose) is added so that its concentration is the same as in breast milk, milk fat is eliminated and replaced with vegetable oils and animal fats that are easier for the baby to digest.
BREAST OR BOTTLE: HOW TO FEED CORRECTLY
At first it may seem that you are only engaged in feeding the baby. How often you feed him depends on how often he is hungry, and one feeding kind of flows into another. Breastfed babies usually want to eat 8-12 times a day - about every 2-3 hours. Formula-fed babies usually want to eat 6-9 times a day - about every 3-4 hours in the first months of life.
Your child will not always be hungry as often. Gradually, he will need fewer daily feedings, and at each feeding he will eat more. The rhythm of life and feeding will begin to emerge in a month or two. Be prepared for the fact that the newborn will usually wake up 1-2 times a night to feed, and will require more milk during periods of increased growth.
The rhythm of life and feeding will begin to emerge in a month or two. Be prepared for the fact that the newborn will usually wake up 1-2 times a night to feed, and will require more milk during periods of increased growth.
Feed on demand . A baby's stomach is very small, about the size of his fist, and it takes 2-3 hours for it to become completely empty. To feed on demand, you need to watch for signs that the baby is hungry: he makes sucking movements with his mouth and tongue, sucks on his fist, makes sounds and, of course, cries. The sensations of hunger cause babies to cry. You will soon learn to distinguish between hungry crying and crying for other reasons: from pain, fatigue, illness. When the baby signals that he is hungry, you need to quickly feed him. This will help the child to understand what discomforts are caused by hunger, and to understand that hunger is satisfied by sucking, bringing food. If you don't react quickly enough, the baby may become so upset that trying to feed will be more frustrating than satisfying.
Obey the child . Try not to rush your baby while feeding. He will decide how much to eat and how quickly. Many children, like adults, prefer to eat slowly. It's perfectly normal for a baby to suckle, take a break, rest, have a little chat, and then go back to eating. Some newborns are fast eaters, eat a lot and fidget all the time. Others are slow, prefer small portions and long breaks. Some, especially newborns, are dormouse. They will suck briefly and vigorously, then fall asleep blissfully, then wake up, eat again and sleep again during the entire feeding time.
The child will also let you know when he has eaten enough. When the baby is satisfied, he will stop suckling, close his mouth or turn away from the nipple. He may push the nipple out of his mouth with his tongue or arch if you try to continue feeding. However, if the baby needs to burp or has begun to defecate, feeding should be interrupted at this time. Wait a little, then offer the breast or bottle again.
Infant formula contains the correct amount of carbohydrates and the correct percentage of fats and proteins. It is the responsibility of each manufacturer to test each batch to ensure that it contains all the necessary substances and nothing harmful.
Infant formula is a high energy food. More than half of its calories come from fat. These fats are made up of many different types of fatty acids. For infant formulas, those whose formula is close to the formula contained in breast milk are selected. These fatty acids help the development of the baby's brain and nervous system, as well as meet energy needs.
For and against. Bottle feeders say the main benefit of this is:
• Greater freedom . Using a bottle of infant formula allows you to feed your baby to different people. Therefore, some mothers feel freer if they are bottle fed. Partners may enjoy bottle feeding because it makes it easier for them to share parenting responsibilities.
However, bottle feeding also presents some challenges:
• Time-consuming preparation . Bottles should be prepared and warmed before each feeding. A constant supply of mixtures is required. Bottles and nipples should be washed. If you are going somewhere, you will have to take everything with you.
• Cost . Formulas are expensive, which is significant for many parents.
• Intolerance to mixture . For some babies, it takes a long time to find the right mixture.
Basic information about artificial feeding. When you first go shopping for baby food, you will be amazed at how many different types there are. Talk to your pediatrician about the right choice. For most children, formulas based on cow's milk with a high iron content are best.
Special blends are also available, such as those containing soy proteins and protein hydrolysates. These mixtures are intended for use in certain digestive disorders and should be used under medical supervision.
Increased iron content is important to prevent anemia and iron deficiency that retard development. Iron deficiency usually does not occur in the first few months of a child's life. However, later, in children 6–10 months old, it was common until iron-fortified formulas were available.
Infant formula is available in three forms: powder, liquid concentrate and ready-to-use. A certain amount of water must be added to powders and concentrates. Dry mixes are usually the cheapest. The most convenient ready-to-use.
If you decide to feed your baby formula, you should have everything you need by the time you return from the hospital. Let the medical staff know that you want to bottle feed. You will be provided with everything you need and mixtures and will be shown how to bottle feed your newborn. But you will need to stock up on your own with everything you need for the future.
For bottle feeding you usually need:
• Four 100g bottles (preferably as it is very convenient in the beginning).
• Eight 250g bottles.
• 8-10 teats with clip rings and caps.
• Measuring cup.
• Bottle brush.
• Infant formula.
Once you've bought everything you need, complete the tutorial if you haven't already. Often, information about feeding newborns is given in childbirth preparation courses. If you haven't bottle fed your baby before, training will help you feel more confident when you get home with your baby.
Where to start. Baby feeding bottles are available in glass, plastic and soft plastic. Usually they come in two sizes: 100 and 250 g. The amount that fits in a bottle does not indicate how much a child should eat in one feeding. At each feeding, he may require more or less.
There are many types of nipples with holes of different sizes according to the child's age. Most babies don't care which pacifier you use. But for babies born at term, very soft nipples intended for premature babies are not suitable.
Use the same teat type for all bottles.
It is important that the food flows out of the nipple at the correct rate. If it flows too fast or too slow, the baby swallows too much air, which causes stomach discomfort and frequent spitting up. Check the speed by turning the bottle upside down and counting the drops. It is normal for about one drop per second to flow out.
Teats are available in sizes for newborns, three months old, six months old, and so on, providing age-appropriate flow rates.
Preparation of mixtures. There are three main types of formulas:
• Based on cow's milk . Most infant formula is made from cow's milk, the composition of which has been adjusted to be closer to breast milk. This ensures the right balance of nutrients and makes the mixture easier to digest. For most babies, cow's milk formulas are fine. But for some who are allergic to cow's milk proteins, other types of baby food are required.
• Soy based . Soy-based formulas are for babies with allergies or intolerances to cow's milk or lactose, a sugar naturally found in cow's milk. Soy formulas are also helpful if you want to eliminate animal proteins from your baby's diet. However, children who are allergic to cow's milk may also be allergic to soy.
• Based on protein hydrolyzate . These formulas are intended for children with family allergies to milk and soy. They are easy to digest and less likely to cause allergic reactions than other types of baby food. They are also called hypoallergenic mixtures.
There are also specialized baby foods for premature babies and babies with certain diseases.
Whatever type and form of baby food you choose, it is important that it is properly prepared and stored so that it is nutritious enough and safe for your baby's health.
Wash your hands before handling utensils and baby formula. Everything you use to measure, mix and store food should be washed with hot soapy water, rinsed and dried before each use. If you are good at cleaning bottles and nipples, it is not necessary to sterilize them. Use a bottle brush to clean the bottles.
If you are good at cleaning bottles and nipples, it is not necessary to sterilize them. Use a bottle brush to clean the bottles.
Wash bottles thoroughly to ensure that no traces of formula remain in them. Rinse well. You can also wash them in the dishwasher.
When using a powder or concentrate mix, add the exact amount of water as directed on the label. Bottle markings may not be accurate, so measure water before adding to formula. Too much or too little water can harm the baby. If diluted too thin, the child will not receive enough nutrients to grow and satisfy hunger. Too concentrated food strains the child's digestive system and kidneys and can lead to dehydration. Cooked meals or liquid concentrate can be stored in the refrigerator for up to 48 hours. Then everything unused must be thrown away.
Warming food is not necessary, but the child may prefer warm food. To warm up for a few minutes, place the bottle in a pot of warm water. Shake the bottle and check the temperature by placing a few drops on your hand. Do not reheat in the microwave as hot spots may form and burn the baby's mouth. If you heated the mixture, do not refrigerate the leftovers, but pour it out.
Do not reheat in the microwave as hot spots may form and burn the baby's mouth. If you heated the mixture, do not refrigerate the leftovers, but pour it out.
In general, it is better to prepare the mixture not in advance, but immediately before use. However, it is worth preparing 1-2 bottles in the evening and placing them in the refrigerator for night feeding. This will make feeding at night easier.
Correct position. The first thing to do when starting bottle feeding is to make yourself comfortable. Find a secluded place where you won't be distracted. Hold the baby with one hand, the bottle with the other, and sit in a comfortable chair, preferably with wide, low armrests. You can put a pillow on your knees to support the child. Hold the baby firmly against you, but not too tightly, so that the head is raised and rests on the crook of your elbow. This elevated position will make it easier to swallow.
Now that you are ready to feed, help your baby get ready. Gently stroke your baby's cheek with a pacifier or finger. This touch will cause the baby to turn towards you, often with their mouth open. Touch the nipple to the baby's lips or the corner of the mouth. He will open his mouth and gradually begin to suck.
Gently stroke your baby's cheek with a pacifier or finger. This touch will cause the baby to turn towards you, often with their mouth open. Touch the nipple to the baby's lips or the corner of the mouth. He will open his mouth and gradually begin to suck.
When feeding, hold the bottle at an angle of approximately 45 degrees. This will keep the nipple full of milk. While the baby is eating, hold the bottle firmly. If the baby fell asleep, it means that he swallowed enough milk, or gases filled the stomach. Remove the bottle, let the baby burp, and try to continue feeding.
Always hold the baby while feeding. Do not leave the bottle leaning against the baby. This can cause either vomiting or overeating. Do not give a bottle if the child is lying on his back. This may increase the risk of getting an ear infection.
Although the baby does not yet have teeth, they are forming under the gums. Do not teach your child to go to bed with a bottle. If he falls asleep with a pacifier in his mouth, the unswallowed mixture stagnates. Prolonged contact with milk sugar contributes to the development of caries.
Prolonged contact with milk sugar contributes to the development of caries.
This text is an introductory fragment.
Chapter 3 Breastfeeding
Chapter 3 Natural (breast) feeding is the most adequate nutrition for a child from birth to one year of age. Feeding is a natural process that is aimed at normal physical and
Diseases and breastfeeding
Diseases and breastfeeding Most known diseases are quite compatible with breastfeeding. Only a very serious condition of the mother requires the cessation of feeding, and most often for a while. If you get sick, tell the doctor that you are a nursing mother and want
How to start breastfeeding
How to start breastfeeding Mom sets a certain rhythm of breastfeeding. Feeding before and after sleep is considered obligatory: it is better for the baby to fall asleep with the breast, and upon awakening, they also offer him a breast. The scheme is as follows: give breasts - shouted -
Feeding before and after sleep is considered obligatory: it is better for the baby to fall asleep with the breast, and upon awakening, they also offer him a breast. The scheme is as follows: give breasts - shouted -
Formula feeding
Artificial feeding When breastfeeding or artificial feeding, one rule should be followed: feeding is a holy time for the child and mother, and nothing should interfere with them. Even if the child is breastfed, sometimes it takes
Chapter 22 Breastfeeding
Chapter 22 Breast-feeding Are you going to breastfeed or bottle feed your baby? Some women already know the answer to this question in advance; others doubt. Of course, breast milk is the best, and all the benefits of breastfeeding are well known. breast milk
Breastfeeding
Breast-feeding Breastfeeding is highly encouraged as it has many health benefits.