Feeding a baby with cleft palate
Cleft Palate: Feeding Your Baby
The palate, more commonly referred to as the roof of the mouth, separates the mouth from the nose. The palate is important for feeding and speaking. A cleft is an opening or split in the palate. This cleft can make feeding hard for your baby. Most babies with a cleft of the palate are not able to use standard bottles or solely breast feed because they cannot create the suction needed to draw the milk out of the nipple. Special bottles and nipples are available to help infants with cleft palate feed and grow. These bottles may be used with formula or breast milk.
Supplies for Feeding Your Baby
Several types of bottles and nipples are available to help you feed your baby. You may need to try more than one feeding system before finding the best one for you and your baby. Our feeding team will work with you and your family to make sure your baby is feeding well and gaining weight.
Examples of Feeding Systems
Assisted Delivery Systems
- Enfamil® Cleft Lip/Palate Nurser: This bottle is soft and squeezable and comes with a long, stiff nipple.
It can also be used with any standard sized nipple, like an orthodontic nipple. To feed your baby, gently squeeze the bottle using a pulsing rhythm while your baby is sucking to help provide the milk (Picture 1).
- Medela® SpecialNeeds™ Feeder (formerly known as the Haberman Feeder™): The flow rate can be adjusted depending on which line is pointing toward the baby’s nose. This nipple has a one-way flow valve to allow the milk to enter your baby’s mouth when the nipple is squeezed. (Picture 2).
Infant paced systems
- Pigeon™ Nipple/Bottle: This Nipple fits on any standard bottle. It has a one-way flow valve that is inserted into the nipple. The special nipple has a soft side and a hard side (Picture 3). The hard side faces up and the soft side sits on the baby’s tongue. There is a notch (air vent) on the nipple that faces toward the baby’s nose during feeding.
 The baby compresses on the nipple during feeding to draw the formula or breast milk into their mouth.
The baby compresses on the nipple during feeding to draw the formula or breast milk into their mouth. - Dr. Brown’s Specialty Feeding System®: This feeding system also has a one-way flow valve that is placed into the nipple to help your baby feed. This valve is very important for feeding. It cannot be found in the bottles available at stores, so it must be purchased online. Please discuss this with our feeding team. The one-way flow valve allows your baby to self-pace by compressing on the nipple. The valve can be used with any level nipple, but you must watch your baby carefully during feeding to make sure the breast milk or formula is not flowing too fast.
How to Feed Your Baby
Here are some tips for feeding:
- Prepare the formula or breast milk for the bottle. If you are using powered formula, mix it with bottled water. Follow the mixing directions carefully for your baby and use the right measuring scoops or spoons.
- Cuddle your baby for a few minutes before you start to feed. This will help you both relax to make feeding time more pleasant.
- Hold your baby in an upright position on your lap and tilt him or her back slightly (Picture 5). This helps the baby to swallow while preventing milk or formula from flowing into the nose or middle ear.
- Rub the nipple of the bottle on the lower lip to help place the nipple into the mouth. This starts the sucking reflex.
- You should hold the bottle during the whole feeding time. The bottle should not be propped by a pillow or other item during feeding. This is not safe for your baby and can cause choking.
- Burp your baby often (after every 1/2 to 1 ounce). Babies may swallow air during feeding.
- Watch your baby closely during feeding to make sure the baby is eagerly and actively engaged in feeding.
- Feeds should be completed in 30 minutes so that your baby does not get too tired.
 This does not include time spent burping or changing the diaper.
This does not include time spent burping or changing the diaper.
If you put your baby to bed after the feeding, place the baby on their back.
As babies get older, they will need more than just formula or breast milk. Be sure to ask our feeding team about when you can start feeding cereal, fruits and vegetables.
If your baby has coughing, gagging, choking, milk running out of the mouth, or signs of distress, like labored breathing or watery eyes, they may be getting too much milk. If you notice these signs, please contact our team for help. You may see that some milk leaks out of the nose during a feeding. This is normal for a child with cleft palate that has not been fixed. It does not mean your child is choking. To help with this, keep your baby more upright during and after feeding. Most infants with cleft palate can feed successfully.
When to Call the Doctor
Call our feeding team or your child's doctor if your baby has:
- Weight loss or failure to gain weight
- Coughing or choking with feeding
- A sunken soft spot on the head
- Feeding takes longer than 30 minutes
- No wet diaper for 6 hours straight
- A hard time waking up for feeding.
 Some children who have other medical conditions along with a cleft palate may have a harder time with feeding and will need other changes in their feeding plan. If you have any questions, be sure to ask your baby’s doctor or nurse, or call 614-722-6449.
Some children who have other medical conditions along with a cleft palate may have a harder time with feeding and will need other changes in their feeding plan. If you have any questions, be sure to ask your baby’s doctor or nurse, or call 614-722-6449.
You can find more information about feeding on the web site of the Cleft Palate Foundation: www.Cleftline.org.
When Your Baby has Surgery
Children have surgery to repair a cleft palate when they are about 10 to 12 months old. Talk to the cleft palate team about surgery and post-operative feeding.
Cleft Palate: Feeding Your Baby (PDF)
HH-I-21 8/84, Revised 8/19 Copyright 1984, Nationwide Children’s Hospital
Cleft Palate - Starting Foods and Cups
Starting Foods
You can introduce foods to children with an unrepaired cleft palate at around 6 months of age, just as in children without a cleft.
The following are some of the signs that your child may be ready for solid food:
- interest in watching others at mealtimes
- holds head up without support
- sits upright with light support
- leans forward to eat food
- keeps tongue in the mouth when offered food
Start by giving your baby slightly thicker foods without lumps, such as Stage 2 baby foods or thicker infant cereals.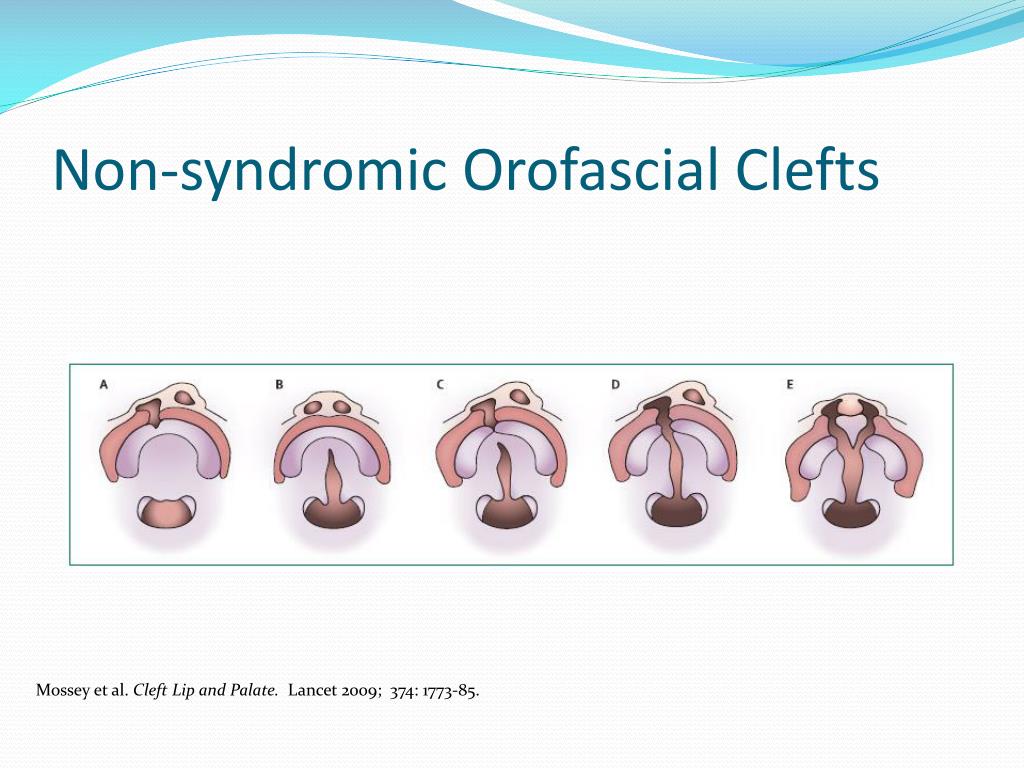 These help your child control the food in their mouth.
These help your child control the food in their mouth.
- Give foods with only one ingredient for a few days before starting any other flavors. This helps you to know if your child has a reaction.
- You do not need to use any special spoons or equipment to feed your baby foods.
- Watch your child carefully to make sure that they swallow each bite before giving them another spoonful. If your child does not seem to swallow a bite, try giving a dry spoon or a spoon with no food on it. This helps your baby swallow any food in the mouth.
Adding More Textures
At around 8 to 9 months of age, fork-mashed table foods (such as avocados and bananas), solids that melt (such as teething crackers) and soft solids (such as a small piece of boiled potato or cooked carrot pieces) can be started. You should watch your child very closely when starting any new food to make sure they are safe while eating.
Once your baby is eating melting solids and soft solids well, you can start giving small pieces of other table foods. This is typically around 10 to 12 months of age.
This is typically around 10 to 12 months of age.
- Some foods should be NOT be given at this age. The following foods can cause choking
in young children:- nuts and seeds
- grapes
- popcorn or chips
- hard pieces of raw fruit or vegetables
- hard or sticky candies
- pieces of hot dog
- tough meats (like, pork chops or steak)
Talk to your child’s health care provider if you have any questions about when you should start certain foods or if a food is safe to give to your baby.
Food in the Nose
Since your child has a cleft of the palate, some foods may enter their nose while eating. Do not worry if this happens. If food enters their nose, it may be a little uncomfortable for your child. It usually gets cleared while eating, drinking or sneezing. Try to avoid wiping your child’s face too often. This may upset your child. Mealtimes may be messy, but it is important for you to stay positive during feedings. If you are happy during the meal, your child will be too!
If you are happy during the meal, your child will be too!
Drinking From a Cup
- You can start giving your child a cup around 6 months of age. Some signs your child is
ready to start drinking from a cup include:- good head control
- eating solid foods
- sitting upright with little support
- holding the cup and tipping it to drink
- Your child should use a free-flowing cup. This is a cup that does not need suction in order to drink the liquid. Free-flowing cups include an open cup or a soft spout sip cup that does not have a spill-proof valve or straw. Some examples of free-flowing cups include:
- Nuby No-Spill™ Super Spout Cup
- Philips Avent My Natural Drinking Cup
- OXO Tot® Transitions Soft Spout Sippy or Training Cup
- NUK® Learner Cup
- Small open cups, such as the Dr. Brown’s™ Bottle lid, a Dixie® cup, or a Nosey cup
There are many other cups that can be used when the spill-proof valve is removed.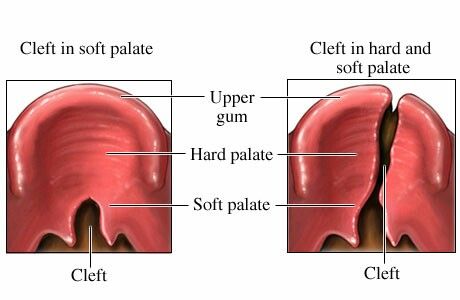 If using another cup, use one with a soft spout since the surgeons allow these cups after palate repair.
If using another cup, use one with a soft spout since the surgeons allow these cups after palate repair.
- When starting to use a cup, put in only a small amount of liquid. Give it to your child one time a day instead of a bottle. It is best to start with the first feeding in the morning since children are often most thirsty at this time. Once your child shows interest in the cup, increase the amount of liquid in the cup. Then, start to offer it more often during the day. The bottle given before bed is often the hardest to change to a cup, but your child may be different.
Getting Ready for Surgery
Since your child will have feeding restrictions after a palate repair, continue to give baby foods or foods without lumps, such as applesauce and yogurt, even while advancing food
textures. You should also continue to offer all drinking options, such as the bottle, free-flowing soft spout sip cups and open cups. These practices will help your child eat and drink
soon after their palate is repaired and get discharged from the hospital quickly.
Problems With Feeding or Drinking
Although most children with a cleft palate do well with starting solid foods, adding textures, and drinking from cups, some may have problems. If you have concerns with your child’s
eating or drinking, please contact the Cleft Lip and Palate Center. We can help make mealtimes more successful.
If you notice problems with feeding or you are concerned with your child’s growth, please call the Cleft Lip and Palate Center’s nurse line during regular business hours from 8 a.m. to
4:30 p.m., Monday through Friday at (614) 722-6299.
After hours, on weekends or holidays, call (614) 722-2000. Ask to speak to the plastic surgeon on call.
Cleft Palate - Starting Foods and Cups (PDF), Spanish (PDF)
HH-IV-212 ©2020 Nationwide Children’s Hospital
How to feed a baby before surgery to close a cleft
nutrients.
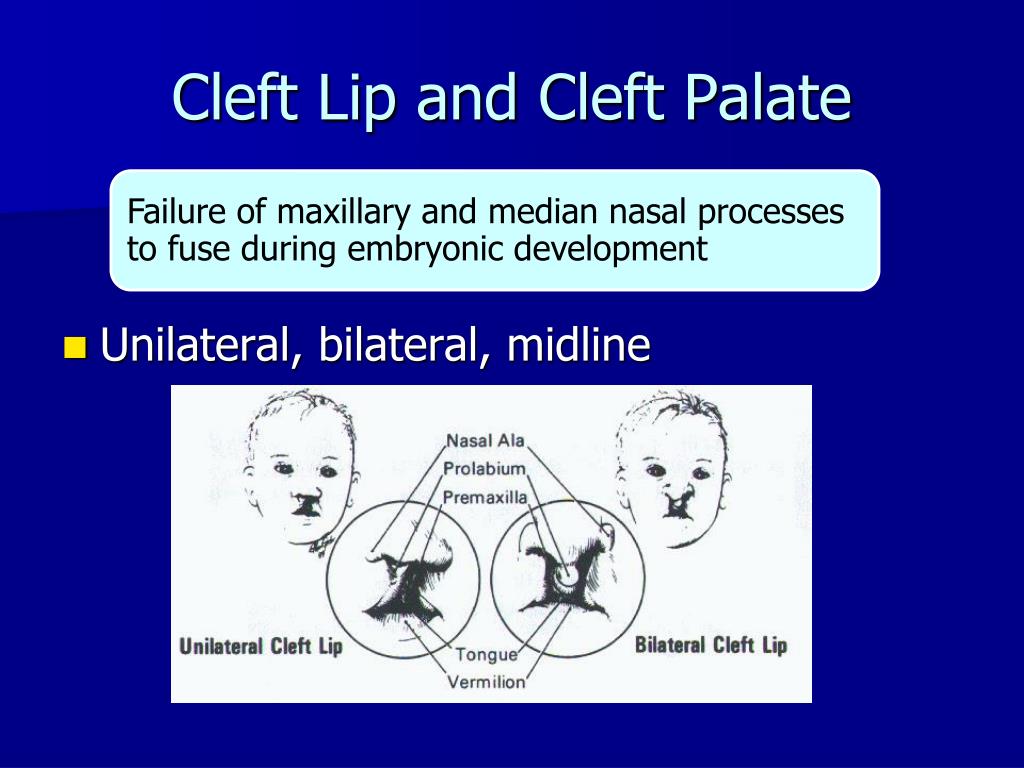
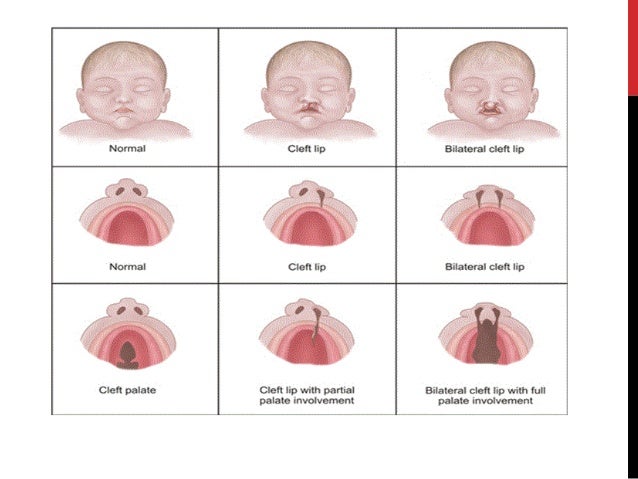
Babies with only cleft lip without palatal integrity usually have no problems with nipple latch and sucking. Children with cleft lip and palate or one cleft palate require some modification of the feeding method, as they have an abnormal communication between the nasal and oral cavity, which prevents the creation of negative pressure necessary for full sucking. Newborns with a cleft palate must squeeze milk out of the nipple by pinching it between the tongue and the rest of the hard palate and alveolar process of the upper jaw.
Children with cleft lip and palate or one cleft palate require some modification of the feeding method, as they have an abnormal communication between the nasal and oral cavity, which prevents the creation of negative pressure necessary for full sucking. Newborns with a cleft palate must squeeze milk out of the nipple by pinching it between the tongue and the rest of the hard palate and alveolar process of the upper jaw.
When milk is squeezed into the mouth of a child with cleft palate, some of it will go into the nose. In addition, during feeding, more air can enter the stomach than in healthy children. This requires frequent changes in the position of the baby when feeding to ensure regurgitation of air. In the first weeks of life, this swallowing of air can lead to disorders such as colic, regurgitation of food, or even slight vomiting. Usually, the child outgrows all these problems within a few months, as the tone of the stomach muscles increases and the activity of the muscles of the digestive tract is coordinated. If some of these symptoms persist for a long time, contact your pediatrician.
If some of these symptoms persist for a long time, contact your pediatrician.
Feeding babies with cleft lip and/or palate
For babies with clefts, as with all newborns, there are two best ways to feed: breastfeeding and bottlefeeding. Cup feeding is not the method of choice, and in the case of normal breastfeeding or bottle feeding, there is no need to resort to this method.
Breastfeeding
There are different opinions about breastfeeding children with clefts. Although it is undeniable that breast milk is the best food for a baby. When a child with a cleft lip or palate is first placed on the breast, there may be some difficulties that are automatically associated with the existence of the cleft. Meanwhile, feeding a baby requires a certain period of trial and error before normal feeding is established.
A baby born with only a cleft lip often has no more difficulty feeding than a baby without a cleft lip, as the breast tends to fill the empty space, adapting and sealing the baby's mouth as much as possible.
Feeding children with perforated cleft lip and palate is also possible if there are no other problems. However, additional patience and modification of feeding technique will be needed to provide the baby with an adequate supply of nutrients, reduce maternal stress, and optimize the baby's responses.
The following tips may be helpful to you.
- Massaging the breast before feeding promotes reflex milk release, which in turn facilitates the flow of milk into the baby's mouth.
Warm compresses applied to the breasts for 20 minutes prior to feeding ensure good blood flow to them.
Frequent breastfeeding (every 2-3 hours) in the first 2 weeks of life is often recommended to establish normal lactation.
Mothers are sometimes advised to increase their fluid intake. - Uses the areola (dark area around the nipple) digital pressure technique to help increase the protrusion of the nipple, making it easier to grab and hold in the baby's mouth. The nipple will enlarge during breastfeeding.
Sometimes the process of feeding is complicated by the appearance of cracks in the nipple. Such cracking may be due to infection or drug therapy. In such cases, to facilitate the feeding of the child, special pads are used to ensure the normal shape of the nipple and alleviate the mother's condition. Subsequently, when the cracks disappear, the nipple will bulge normally. - If, after several attempts, the baby is unable to hold on to the nipple, or if you feel that the baby is not fully satiated, collect the remaining milk with a breast pump and finish feeding this milk from the bottle. In any case, when you are supplementing a baby from a bottle, you should always give the baby the breast first and then the bottle. With gradual adaptation, increasing strength and patience of your baby, the process of breastfeeding can become longer.
Bottle-feeding
It happens that it is not possible to establish normal sucking strength during attachment to the breast, especially in children with bilateral cleft lip and palate, in which the child cannot compensate for the pathological communication between the mouth and nose . In such cases, the only way to obtain breast milk is to bottle feed expressed breast milk. It is advisable to feed the baby with milk expressed using a breast pump for several weeks or, if possible, longer. Even when your baby has been breastfed but breastfeeding has been delayed due to surgery or other reasons, you can bottle feed your baby with expressed milk until you can return to normal breastfeeding. In addition, there are currently ways to harvest breast milk for a certain period. Questions about how and when to store milk should be discussed with your pediatrician. In addition, there are currently a large number of breast pumps that significantly reduce the pumping time and ensure the maintenance of lactation for a long time.
In such cases, the only way to obtain breast milk is to bottle feed expressed breast milk. It is advisable to feed the baby with milk expressed using a breast pump for several weeks or, if possible, longer. Even when your baby has been breastfed but breastfeeding has been delayed due to surgery or other reasons, you can bottle feed your baby with expressed milk until you can return to normal breastfeeding. In addition, there are currently ways to harvest breast milk for a certain period. Questions about how and when to store milk should be discussed with your pediatrician. In addition, there are currently a large number of breast pumps that significantly reduce the pumping time and ensure the maintenance of lactation for a long time.
Formula feeding
Formula feeding is a simple and reliable substitute for breast milk. For this type of feeding, the same principles are acceptable as for breastfeeding, with the exception of small additions to the technique if necessary.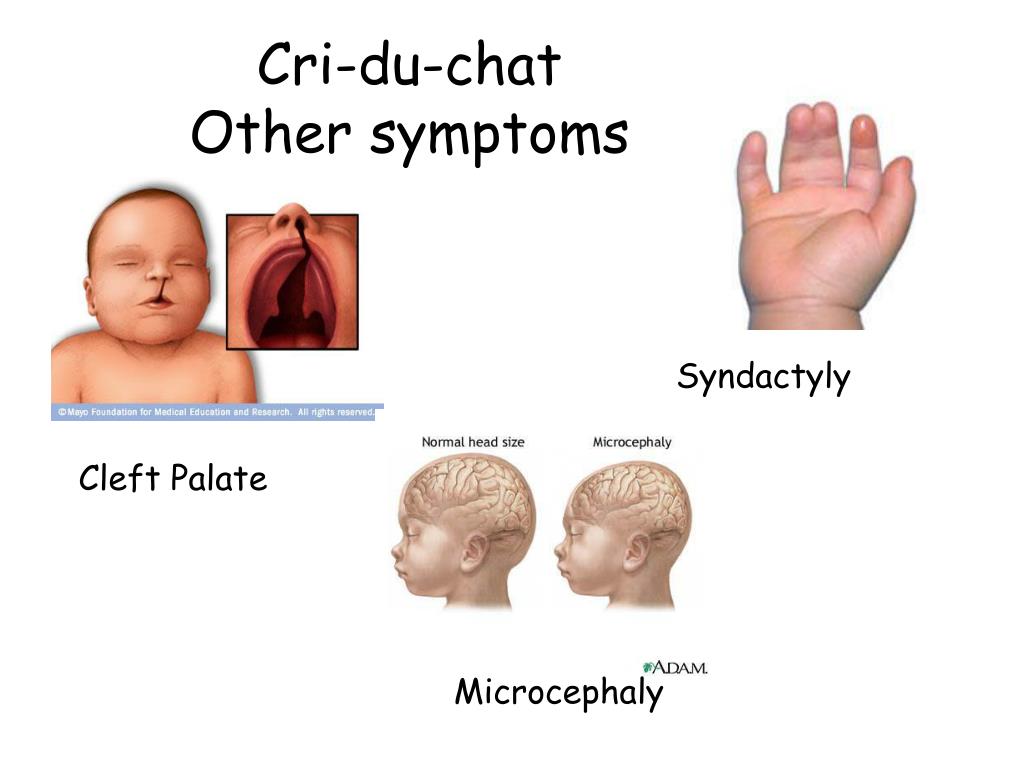 In addition, the easier intake of food with wide cleft lip and palate will help your child more easily compensate for the difficulties that arise from pathological communication of the oral cavity and nose. The selection of the necessary mixture for your baby can be adequately carried out by your pediatrician, who is guided by the peculiarities of the metabolism and digestive system of each child. Remember that you need to carefully study the instructions for preparing the mixture, which is usually located on the label of each package. Sometimes the pediatrician may recommend increasing the concentration of the mixture to speed up the weight gain of the child. This is a temporary measure, since the intake of water into the child's body is no less important than the amount of food consumed. For children with a cleft, a pacifier and bottle may need to be matched. Usually, parents start with simple types of nipples and bottles, and often, especially for children with small cleft lips, they are suitable.
In addition, the easier intake of food with wide cleft lip and palate will help your child more easily compensate for the difficulties that arise from pathological communication of the oral cavity and nose. The selection of the necessary mixture for your baby can be adequately carried out by your pediatrician, who is guided by the peculiarities of the metabolism and digestive system of each child. Remember that you need to carefully study the instructions for preparing the mixture, which is usually located on the label of each package. Sometimes the pediatrician may recommend increasing the concentration of the mixture to speed up the weight gain of the child. This is a temporary measure, since the intake of water into the child's body is no less important than the amount of food consumed. For children with a cleft, a pacifier and bottle may need to be matched. Usually, parents start with simple types of nipples and bottles, and often, especially for children with small cleft lips, they are suitable. If the baby is not satisfied with the proposed devices, you can try using special orthodontic nipples and soft bottles. Your main task is to select the nipple and bottle that will make feeding the baby easy and complete.
If the baby is not satisfied with the proposed devices, you can try using special orthodontic nipples and soft bottles. Your main task is to select the nipple and bottle that will make feeding the baby easy and complete.
Soft nipples are usually better than hard nipples. You can soften the nipple by boiling. Subsequently, with the strengthening of your baby's chewing muscles, soft nipples can be replaced with soft orthodontic or harder nipples.
Some children with clefts may have difficulty with both very long and very short nipples. Short nipples cannot provide good contact with the tongue and palate, while long nipples can provoke a gag reflex.
One of the ways to regulate the flow of milk into the baby's mouth is the cross hole on the tip of the nipple. Such cuts facilitate the flow of liquid from the bottle. Cross-shaped incisions are very convenient, as they allow the child to regulate the strength and speed of milk flow with a constant sucking rhythm, preventing choking. A simple enlargement of the opening in the nipple causes a steady increase in the flow of milk into the baby's mouth, which leads to difficulty in sucking control and disruption of the interaction between swallowing and breathing. On the contrary, the cruciform incision ensures the flow of milk only at the moment of squeezing the nipple. Any nipple can be made into a cross-cut nipple with a regular razor blade. If it is required to make an incision on the orthodontic nipple, then it is better to perform it not at the very top, but a little closer to the lingual surface, as this will contribute to a dosed flow of fluid.
A simple enlargement of the opening in the nipple causes a steady increase in the flow of milk into the baby's mouth, which leads to difficulty in sucking control and disruption of the interaction between swallowing and breathing. On the contrary, the cruciform incision ensures the flow of milk only at the moment of squeezing the nipple. Any nipple can be made into a cross-cut nipple with a regular razor blade. If it is required to make an incision on the orthodontic nipple, then it is better to perform it not at the very top, but a little closer to the lingual surface, as this will contribute to a dosed flow of fluid.
Another way to make milk flow easier while conserving baby's energy is to use soft bottles. The compression of such a bottle should be carried out rhythmically and correspond to the frequency of sucking and swallowing food by the child (approximately every 2-3 sips). Following the rhythm of the child, you can be sure that there will be no excessive intake of milk into the oral cavity and its reflux into the respiratory tract. The bottle must be squeezed and then released without continued compression. Feeding is usually easier if the bottle is angled to the opposite side of the mouth from the cleft, so that the nipple can be compressed between the tongue and the remaining normal part of the alveolar process of the maxilla and hard palate. Your baby will make the necessary adjustments on his own, adjusting to the position of the nipple, making it easier for him to get milk from the bottle. To do this, you only need to hold the bottle in one position and give the child the opportunity to shift the nipple from one corner of the mouth to another.
The bottle must be squeezed and then released without continued compression. Feeding is usually easier if the bottle is angled to the opposite side of the mouth from the cleft, so that the nipple can be compressed between the tongue and the remaining normal part of the alveolar process of the maxilla and hard palate. Your baby will make the necessary adjustments on his own, adjusting to the position of the nipple, making it easier for him to get milk from the bottle. To do this, you only need to hold the bottle in one position and give the child the opportunity to shift the nipple from one corner of the mouth to another.
When choosing a method of feeding, parents should understand for themselves some of the main advantages of bottle feeding:
- the most adequate supply of milk to the baby's body;
- saving physical energy spent on feeding, both by the child and the parent;
- the method allows to normalize suckling;
- is the most affordable, inexpensive and easiest way to feed.

Other feeding recommendations
Feeding position
It is very important that the breastfeeding parent finds the most comfortable position for himself. Sometimes, for comfort, it is useful to use a pillow to support the child. It also makes it easier to support the child with a footrest, on which the parent can lean with both one and two legs. Since feeding a baby can take up to 30 minutes. several times a day, the adult feeding the child should choose the most comfortable and relaxed position for himself.
The baby should be well supported during feeding, usually in a slightly elevated position or sitting. This position helps prevent milk from entering the nose and choking the baby.
While breastfeeding, the mother can use several positions that can make the process much easier. The first position, when the child sits on a mattress or pillow, his back is supported by the mother's forearm, and her head by her hand. In this position, gravity helps the nipple to be placed in the baby's mouth.
In this position, gravity helps the nipple to be placed in the baby's mouth.
It is very important to push the chest away from the baby's nose so as not to interfere with adequate breathing.
Another position where the child sits on the mother's lap, facing her, with the child's legs wide apart, embracing the mother's stomach. Sometimes it is necessary to use a pillow in order to lift the child higher.
In order to suckle effectively, the baby's lower jaw must be in a stable position. If the mother supports the child by the lower jaw or chin, then the baby will not get tired so quickly. It is also useful for the baby's head to be turned first to one side and then to the other during feeding. Such a change allows the muscles of the oral region to work evenly. When bottle feeding, it is important that the baby is supported in an elevated position. The nipple should be placed in the area where all tissues are most preserved.
How to choose the right time to feed
When a baby starts crying loudly and seems agitated, there is a good chance that he is very hungry and this can make feeding very difficult. It is necessary to feed the child before he becomes too hungry. The child eats better when he is slightly hungry and does not feel much discomfort.
It is necessary to feed the child before he becomes too hungry. The child eats better when he is slightly hungry and does not feel much discomfort.
Many parents find that they can learn their baby's feeding schedule by watching for certain "signals" of the baby during awakening (moving the eyes under closed eyelids, moving the mouth, or moving the hands to the mouth). However, it must be remembered that the child does not eat the same amount of liquid during each feeding. It depends on the time elapsed between feedings.
Help with food in the nose
Even when a fed baby is in a semi-elevated position, there is a risk of milk entering the nose (nasal regurgitation). Sometimes such regurgitation can be associated with a sudden change in body position. Parents should not be overly concerned about this, as food getting into the nose is quite common at first. It does not harm the child and gradually decrease with the growth of the baby. When regurgitation occurs, it is necessary to temporarily stop feeding and give the baby some time to cough or sneeze. This will allow the baby to clear the nasal passages and you can continue feeding. However, if the child has persistent regurgitation, cough is frequent and severe, you should consult your doctor.
This will allow the baby to clear the nasal passages and you can continue feeding. However, if the child has persistent regurgitation, cough is frequent and severe, you should consult your doctor.
Use of palatal obturators
Some specialists involved in the treatment of children with cleft lip and palate believe that obturators (special palatal plates that follow the curvature of the palate) should be used when feeding children with cleft palate, as they separate the oral and nasal cavity, which can greatly facilitate feeding. Such obturators tend to damage the mucosa. A more reliable result is obtained when the fitting of the obturator is carried out in the first few days of life. If you agree to use such a device, then you must be in close contact with a specialist who will manufacture, try on and adjust the device, periodically replacing it with a new one.
Most babies born with cleft palate and lip can be adequately fed without the use of such a machine when parents use combinations of feeding positions, appropriate feeding pattern (bottle or while breastfeeding), and appropriate technique.
Solid food introduction
Your child should be ready for pureed food at the same age as other children. Pureed food should be introduced at 4–6 months of age. Feeding should be done with a spoon, not a bottle. This is the time when the child begins to be interested in the difference in tastes and states. Again, moving from an elevated position to a sitting position reduces the number of episodes of regurgitation. Initially, the child should receive a small amount of liquid (no lumps) cereal porridge mixed with artificial formula until he learns to feel the pieces of food in his mouth. Pureed food should be given to the child until he is very hungry, otherwise the child will refuse to eat. The child must be gradually accustomed to more adult food, which takes time and patience. At first, the baby will try to suck in new food, which can again lead to episodes of food entering the nose. If this happens, give the child some water to drink. As soon as the child learns to swallow food, the density of porridge can be increased by mixing it with less milk.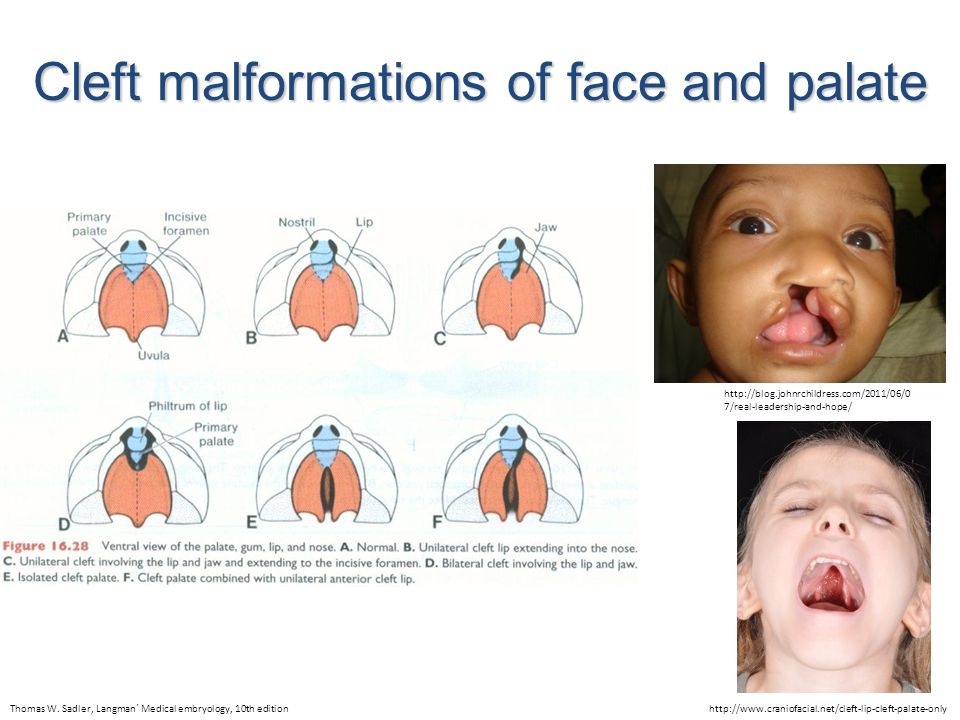 After that, you can add other complementary foods. If a child continues to have difficulty learning to eat solid foods for a long time, it is necessary to seek advice from specialists involved in the treatment of children with cleft lip and palate.
After that, you can add other complementary foods. If a child continues to have difficulty learning to eat solid foods for a long time, it is necessary to seek advice from specialists involved in the treatment of children with cleft lip and palate.
Recommended feeding steps
| 4-6 months | introduction of porridge and puree soups |
| 8 months | give liquid, pureed food, introduce more hard or crushed food |
| 12 m. | give liquid, coarser chopped food, include chewy meat food |
| 18 mo. | give liquid, coarser chopped food, increase the amount of meat food, and increase the amount of raw vegetables |
General questions
1. How often does the baby need to burp?
Frequent regurgitation usually occurs in children who swallow large amounts of air during feeding. The baby usually signals impending regurgitation by slowing down or stopping suckling. This is the time when the baby can burp, and not at the moment of active sucking.
This is the time when the baby can burp, and not at the moment of active sucking.
2. Does the cleft area need cleaning?
A child's mouth, whether it has a cleft or not, tends to clean itself. Some newborns with cleft lip do not need additional cleaning, but you should come to such a decision with your pediatrician. Removal of small amounts of curdled milk in the area of the cleft can be successfully carried out by giving the child a few sips of water. In any case, it may be necessary to gently wipe the baby's face and mouth area with a damp cloth. The use of cotton swabs or rinsing with a syringe is not recommended, as this can damage the baby's delicate mucous membrane.
3. How to feed during the early postoperative period?
The surgeon who will operate on your child will definitely tell you about the features of feeding the baby after the restoration of the lip or palate. Mostly, parents should change the way of feeding immediately after surgery, and then the usual way of feeding will be restored. You will undoubtedly receive advice on restrictions and the introduction of a new way of feeding a few weeks before the operation so that you can gradually get used to this way.
You will undoubtedly receive advice on restrictions and the introduction of a new way of feeding a few weeks before the operation so that you can gradually get used to this way.
4. When can cup feeding be introduced?
A cleft baby can be cup fed in the same way as other babies. Most babies are ready for this way of eating at 8-9 months of age. There are many types of cups for babies, which can greatly reduce the adjustment period, as some cups may make a baby drink better than others. This helps to establish this way of feeding before palate plasty, especially if your child is already ready for the operation. Drinking from a cup does not adversely affect the newly operated lip and will allow you to return to your usual way of feeding after the operation. Since bottle-feeding is not allowed after palate plasty, gradually weaning the child from it will allow you to avoid unnecessary whims after the operation.
The experience of feeding a baby is extremely important for both parents and their baby. Newborn children adapt more easily, and infants learn faster if the parents have the necessary support, patience and love. Remember that there are many experienced professionals ready to provide you with the support you need.
Newborn children adapt more easily, and infants learn faster if the parents have the necessary support, patience and love. Remember that there are many experienced professionals ready to provide you with the support you need.
| Feeding a child with cleft lip and palate
Feeding a child with CLP
Babies with only cleft lip and palate do not usually have problems with nipple latch and suction. Whereas children with cleft lip and palate (CLPA) or only cleft palate require a different approach to feeding. The pathological communication between the nasal and oral cavities makes it impossible to create a vacuum in the oral cavity and thus prevents full sucking. As a rule, children with CCLP are transferred to artificial feeding quite early, but even at the same time, during feeding, part of the milk spills out, and swallowed large amounts of air causes frequent, profuse regurgitation. This requires frequent changes in the position of the baby when feeding to facilitate spitting up. The impossibility of proper feeding and mixed breathing in children with CCLP create favorable conditions for the development of inflammatory processes in the ENT organs, lungs and gastrointestinal tract. To avoid these complications, it is necessary to follow a number of simple recommendations.
The impossibility of proper feeding and mixed breathing in children with CCLP create favorable conditions for the development of inflammatory processes in the ENT organs, lungs and gastrointestinal tract. To avoid these complications, it is necessary to follow a number of simple recommendations.
Breastfeeding
There is no doubt that breast milk is the best food for a baby. Therefore, if a mother wants to breastfeed a child with CCLP, there are special recommendations that will facilitate this process.
• Massaging the breast before feeding promotes reflex milk ejection, which in turn makes it easier for milk to flow into the baby's mouth.
• Warm compresses applied to the breasts for 20 minutes before a feed will ensure good blood flow to them.
• Frequent breastfeeding (every 2-3 hours) in the first 2 weeks of life, which contributes to the establishment of normal lactation.
• Finger pressure on the areola (the dark area around the nipple) helps increase nipple prominence, making it easier to grab and hold in your baby's mouth. The nipple will enlarge during breastfeeding.
The nipple will enlarge during breastfeeding.
• To facilitate the feeding of the baby, special pads are used to ensure the normal shape of the nipple.
If, after several attempts, the baby is unable to hold on to the nipple, or if you feel that the baby is not fully satiated, collect the remaining milk with a breast pump and finish feeding this milk from the bottle. In any case, when you are supplementing your baby with a bottle, you should always give the baby the breast first, and only then the bottle. With gradual adaptation, increasing strength and patience of your baby, the process of breastfeeding can become longer.
When feeding children with cleft palate, obturators (special palatal plates that repeat the curvature of the palate) can be used, as they separate the oral and nasal cavities, providing greater feeding efficiency. However, it should be borne in mind that such devices can damage the oral mucosa. To prevent this complication, fitting the obturator is carried out in the first few days of life. In the process of using the device, it should be tried on and adjusted, periodically replacing it with a new one.
In the process of using the device, it should be tried on and adjusted, periodically replacing it with a new one.
Bottle feeding
In cases where it is not possible to establish a normal sucking force during attachment to the breast, especially in children with bilateral cleft lip and palate, a bottle with a nipple must be used for breast milk feeding. It is advisable to feed the baby with milk expressed using a breast pump for several weeks, and if possible, longer. Modern breast pumps significantly reduce the pumping time and ensure the maintenance of lactation for a long time. Currently, there are ways to harvest breast milk for a certain period. Questions about how and when to store milk should be discussed with your pediatrician.
Artificial feeding
If it is impossible to breastfeed, artificial feeding is used. This uses the same principles as for breastfeeding, with the exception of small additions to the technique. Easier food intake will compensate for the efforts that occur during pathological communication of the oral cavity and nose, especially with wide cleft lip and palate. When choosing a pacifier and a bottle, first of all, feeding efficiency should be taken into account, and it depends on several factors:
When choosing a pacifier and a bottle, first of all, feeding efficiency should be taken into account, and it depends on several factors:
• nipple pressure on underlying tissues;
• nipple shapes;
• elasticity of the material from which it is made;
• Diameter of the hole in the nipple - it should not be very large, as the child will choke, and, in addition, under such conditions, he does not need to exert great effort when sucking, and therefore the lower jaw will be underdeveloped.
Orthodontic nipples and soft bottles are usually used. To begin with, a soft nipple is suitable for a child, but over time it needs to be changed to a more rigid one, for the optimal development of the baby's chewing muscles.
Recently NUK latex nipples have become popular. They allow you to feed the baby artificially, despite the presence of a cleft. There is no hole in the nipple - it is made individually for each baby in accordance with the doctor's recommendations and depending on the direction of the cleft, but not in the upper part of the nipple that closes the cleft. There should be several holes in the nipple, and their sizes are standard, so that when the bottle is turned upside down, the milk only drips, and does not flow out in a trickle. The nipples have a wide mouthpiece that promotes the natural sucking reflex.
There should be several holes in the nipple, and their sizes are standard, so that when the bottle is turned upside down, the milk only drips, and does not flow out in a trickle. The nipples have a wide mouthpiece that promotes the natural sucking reflex.
In the process of feeding, it is necessary to control the swallowing of formula or milk. You should not allow the presence of a large volume of the nutrient mixture in the oral cavity. In all children, when using a pacifier, the nutrient mixture enters the oral cavity in drops, while the circular split muscle remains passive, the back of the tongue rises, separating the mouth and nose. At the same time, the most physiological sucking is noted in children, even with a cleft lip and palate.
Some children with clefts may have difficulty with both very long and very short nipples. Short nipples cannot provide good contact with the tongue and palate, and long nipples can provoke a gag reflex.
One of the ways to regulate the flow of milk into the baby's mouth is the cross hole at the tip of the nipple. Such cuts facilitate the flow of liquid from the bottle. Cross-shaped incisions are very convenient, as they allow the child to regulate the strength and speed of milk flow with a constant sucking rhythm. Simply enlarging the opening in the nipple causes a steady increase in the flow of milk into the baby's mouth, resulting in difficulty in suckling control and disruption of the interaction between swallowing and breathing. On the contrary, a cruciform incision ensures the flow of milk only at the moment of squeezing the nipple. Any nipple can be made into a cross-cut nipple with a regular razor blade. If it is required to make an incision on the orthodontic nipple, then it is better to perform it not at the very top, but a little closer to the lingual surface, as this will contribute to the metered flow of fluid.
Such cuts facilitate the flow of liquid from the bottle. Cross-shaped incisions are very convenient, as they allow the child to regulate the strength and speed of milk flow with a constant sucking rhythm. Simply enlarging the opening in the nipple causes a steady increase in the flow of milk into the baby's mouth, resulting in difficulty in suckling control and disruption of the interaction between swallowing and breathing. On the contrary, a cruciform incision ensures the flow of milk only at the moment of squeezing the nipple. Any nipple can be made into a cross-cut nipple with a regular razor blade. If it is required to make an incision on the orthodontic nipple, then it is better to perform it not at the very top, but a little closer to the lingual surface, as this will contribute to the metered flow of fluid.
Another way to make milk flow easier while conserving baby's energy is to use soft bottles. The compression of such a bottle should be carried out rhythmically and correspond to the frequency of sucking and swallowing food by the child (approximately every 2-3 sips). By following the rhythm of the baby, you can be sure that there will be no excessive intake of milk into the oral cavity and its reflux into the respiratory tract. The bottle must be squeezed and then released without continued compression. Feeding is usually easier if the bottle is angled away from the cleft side of the mouth so that the nipple can be squeezed between the tongue and the remaining normal maxillary alveolar bone and hard palate. Your baby will make the necessary adjustments by adjusting to the position of the nipple, making it easier for him to get milk from the bottle. To do this, it is only necessary to hold the bottle in one position and allow the child to shift the nipple from one corner of the mouth to another.
By following the rhythm of the baby, you can be sure that there will be no excessive intake of milk into the oral cavity and its reflux into the respiratory tract. The bottle must be squeezed and then released without continued compression. Feeding is usually easier if the bottle is angled away from the cleft side of the mouth so that the nipple can be squeezed between the tongue and the remaining normal maxillary alveolar bone and hard palate. Your baby will make the necessary adjustments by adjusting to the position of the nipple, making it easier for him to get milk from the bottle. To do this, it is only necessary to hold the bottle in one position and allow the child to shift the nipple from one corner of the mouth to another.
Feeding position
It is very important that the breastfeeding parent finds the most comfortable position for himself. Sometimes, for comfort, it is useful to use a pillow to support the child. It also makes it easier to support the child with a footrest, on which the parent can lean with one or both feet. Since feeding a baby can take up to 30 minutes. several times a day, the adult feeding the baby should find the most comfortable and relaxed position for himself.
Since feeding a baby can take up to 30 minutes. several times a day, the adult feeding the baby should find the most comfortable and relaxed position for himself.
The baby should be well supported during feeding, usually in a slightly elevated position, or sitting. This position helps prevent milk from entering the baby's respiratory tract.
While breastfeeding, the mother can use several positions that make the process much easier. The first position is when the child sits on a mattress or pillow, his back is supported by the mother's forearm, and her head is supported by her hand. In this position, gravity helps the nipple to be placed in the baby's mouth.
It is very important to push the chest away from the baby's nose so as not to interfere with adequate breathing.
Another position is when the child sits on the mother's lap, facing her, with the child's legs wide apart, embracing the mother's stomach. Sometimes it is necessary to use a pillow in order to lift the child higher.
In order to suckle effectively, the baby's lower jaw must be in a stable position. If the mother supports the child by the lower jaw or chin, then the baby will not get tired so quickly. It is also helpful to have the baby's head turned first to one side and then to the other during feeding. This change allows you to evenly work the circular muscles. When bottle-feeding, it is important that the baby is supported in an elevated position. The nipple should be placed in the area where all the tissues are most preserved.
Help with food entering the nose
Even when a fed baby is in a semi-elevated position, there is a risk of milk entering the nose (nasal regurgitation). Sometimes such regurgitation can be associated with a sudden change in body position. Parents should not worry too much about this, as food entering the nose is quite common at first. It does not harm the baby and will gradually decrease as the baby grows. When regurgitation occurs, it is necessary to temporarily stop feeding and give the baby some time to cough or sneeze.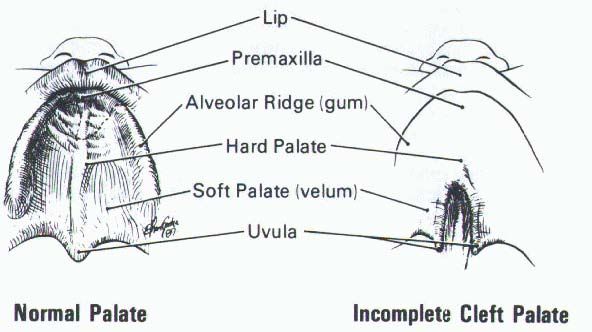 This will allow the baby to clear the nasal passages and you can continue feeding. However, if the child has persistent regurgitation and the cough is frequent and severe, you should consult your doctor.
This will allow the baby to clear the nasal passages and you can continue feeding. However, if the child has persistent regurgitation and the cough is frequent and severe, you should consult your doctor.
Solid food introduction
Your child should be ready for pureed food at the same age as other children. Pureed food should be introduced at 4-6 months. Feeding should be done with a spoon, not a bottle. At the same time, the transition from an elevated position to a sitting position reduces the number of episodes of regurgitation. Initially, the child should receive a small amount of liquid (no lumps) cereal porridge mixed with artificial formula until he can feel the pieces of food in his mouth. The child must be gradually accustomed to more adult food, which takes time and patience. At first, the baby will try to absorb new food, which can again lead to episodes of food entering the nose. In these cases, give the child some water to drink. As soon as the child learns to swallow food, the density of the porridge can be increased by mixing it with less milk.
Frequently Asked Questions
1. How often does a child need to burp air?
Frequent regurgitation usually occurs in children who swallow large amounts of air during feeding. The baby usually signals the impending regurgitation by slowing down or stopping suckling. It is at this time that the child should be given the opportunity to burp, and not at the moment of active sucking.
2. Does the cleft area need to be cleaned?
A child's mouth, whether or not it has a cleft, tends to clean itself. Some newborns with cleft lip do not need additional cleaning, but this decision should be made with your pediatrician. A small amount of curdled milk in the area of the cleft can be successfully removed by giving the child a few sips of water. In any case, a small, gentle wipe over the child's face and mouth with a damp cloth may be required. The use of cotton swabs or rinsing with a syringe is not recommended, as this can damage the delicate lining of the child's mouth.
3. How to feed during the early postoperative period?
The surgeon who will operate on your child will definitely tell you about the peculiarities of feeding the baby after the restoration of the lip or palate. Mostly, parents should change the way of feeding immediately after surgery, and then the usual way of feeding will be restored. You will no doubt receive advice on restrictions and the introduction of a new way of feeding a few weeks before the operation in order to gradually get used to this method.
4. When can cup feeding be introduced?
A cleft baby can be cup fed at the same time as other babies. Most children are ready for this way of eating at the age of 8-9 months. Drinking from a cup does not adversely affect the newly operated lip and will allow you to return to your usual way of feeding after surgery. Since bottle-feeding is not allowed after a palatoplasty, gradually weaning your baby from bottle-feeding will allow you to avoid unnecessary whims after the operation.