How long should i leave my premature baby between feeds
Caring for Your Premature Baby
The birth of a baby is usually a happy time but can also be stressful. There are many things that can add stress, including if your baby is born premature. A baby is premature if it is born before the 37th week of a normal pregnancy. Sometimes premature babies are called “preemies.”
Path to improved health
Babies who are born premature will likely need special care during their first 2 years. This is especially true if they weigh less than 3 pounds when they’re born. But you can help your baby be healthy, grow, and develop when you bring them home from the hospital. Here’s some advice:
- Make an appointment to take your baby to the doctor soon after the baby leaves the hospital. Your doctor will check your baby to confirm that they are gaining weight and discuss how your baby is doing at home.
- Talk with your doctor about feeding your baby. Breast milk is the best baby food but breastfeeding may not be an option with premature babies.
Premature babies often have more difficulty with breast feeding because of their delayed development. It’s also difficult because it may take longer for the mother’s milk to come in given the premature birth. If your baby is having trouble nursing, your doctor may be able to help you solve this problem. Or your doctor may refer you to a lactation consultant. Breast milk can be fed from a bottle as well as from the breast. It can be pumped and stored if you prefer to feed breast milk from a bottle. This is helpful if you’re away from your baby due to his or her care needs or your work. If your baby takes formula instead of breast milk, a special formula may be needed. Your doctor may recommend you give your baby vitamins and iron. Vitamins are often given to premature babies to help them grow and stay healthy. Your baby also may need extra iron. That’s because premature babies don’t have as much iron in their bodies as full-term babies. Your doctor may want your baby to take iron drops for a year or longer.
- Watch your baby’s growth. Premature babies may not grow at the same rate as a full-term baby for the first 2 years. Premature babies are usually smaller during this time. Sometimes they grow in spurts. They usually catch up with full-term babies in time. To keep a record of your baby’s growth, your doctor can use special growth charts for premature babies. Your doctor also will want to keep track of your baby’s milestones. This would include things like activity level, sitting up, and crawling.
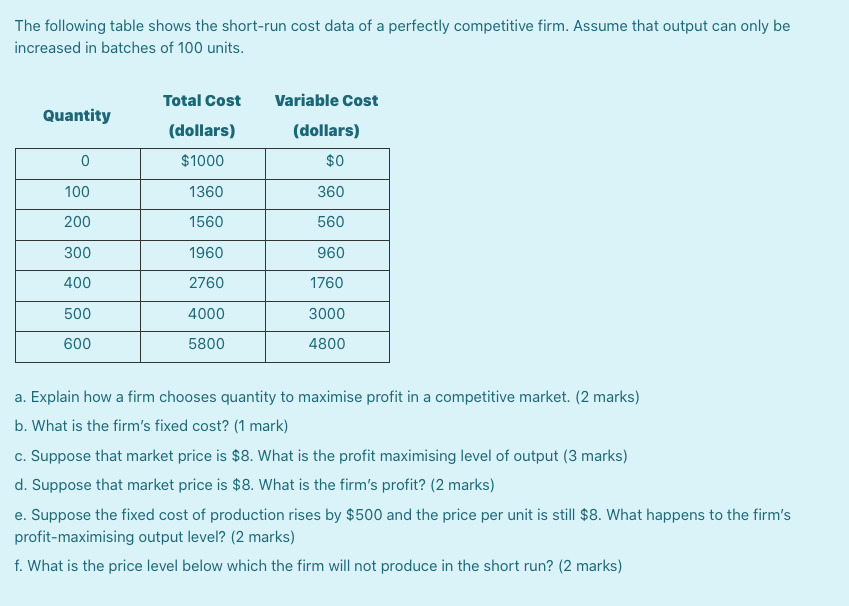
- Be consistent with your baby’s feeding schedule. Most premature babies need 8 to 10 feedings a day. Don’t wait longer than 4 hours between feedings or your baby may get dehydrated (not getting enough fluids). Six to 8 wet diapers a day show that your baby is getting enough breast milk or formula. Premature babies often spit up after a feeding. This is normal. However, you want to make sure your baby is still gaining weight. Talk to your doctor if you think your baby has stopped gaining or is losing weight.
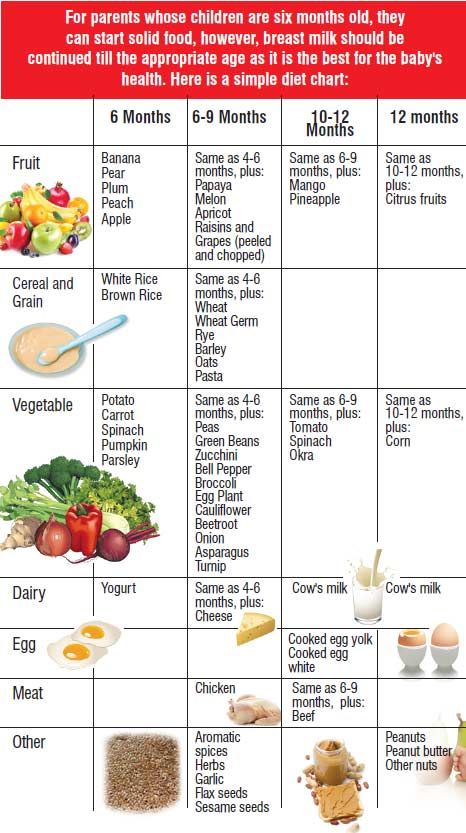
- Prepare for solid food. Most doctors advise giving a premature baby solid food at 4 to 6 months after the baby’s original due date (not the birth date). Premature babies aren’t as developed at birth as full-term babies. It may take them longer to develop their swallowing ability. If your baby has medical problems, your doctor may recommend a special diet.
- Give your baby plenty of opportunity for sleep. Although premature babies sleep more hours each day than full-term babies, they sleep for shorter periods of time. All babies should be put to bed on their backs, not on their stomachs. This includes premature babies. Use a firm mattress and no pillow. Sleeping on the stomach and sleeping on a soft mattress may increase your baby’s risk of sudden infant death syndrome (SIDS). Also called “crib death,” it is the sudden and unexplained death of a baby younger than 1 year. It usually happens while the infant is asleep.
- Check your baby’s vision.
 Crossed eyes are more common in premature babies than in full-term babies. The medical term for this condition is strabismus. This problem usually goes away on its own as your baby grows and develops. Your doctor may want you to take your baby to an eye doctor if your baby has this problem. Some premature babies have an eye disease called retinopathy of prematurity (ROP). This is where the small blood vessels in the eye grow abnormally. ROP usually occurs in babies who are born at 32 weeks of pregnancy or earlier. If there’s a chance your baby has ROP, your doctor will advise taking them to the eye doctor for regular checkups.
Crossed eyes are more common in premature babies than in full-term babies. The medical term for this condition is strabismus. This problem usually goes away on its own as your baby grows and develops. Your doctor may want you to take your baby to an eye doctor if your baby has this problem. Some premature babies have an eye disease called retinopathy of prematurity (ROP). This is where the small blood vessels in the eye grow abnormally. ROP usually occurs in babies who are born at 32 weeks of pregnancy or earlier. If there’s a chance your baby has ROP, your doctor will advise taking them to the eye doctor for regular checkups. - Check your baby’s hearing. Premature babies are also more likely than full-term babies to have hearing problems. If you notice your baby doesn’t seem to hear you, tell your doctor. You can check your baby’s hearing by making noises behind or to the side of the baby. If your baby doesn’t turn his or her head, or react to a loud noise, tell your doctor.
- Get your baby’s immunizations. Immunizations (also called vaccines or shots) are given to premature babies at the same ages they are given to full-term babies. Your baby may need a flu shot when they are 6 months old. Premature babies might get sicker with the flu than full-term babies. Talk with your doctor about flu shots for your entire family. This can help protect your baby from catching the flu from someone in the family.
- Protect your baby while traveling in a car. When traveling with your baby in a car, use a safety-approved infant car seat. Be sure that your baby’s head and body don’t slump over when they are in the car seat. Your premie baby may need extra support in the car seat. You can use rolled-up towels or receiving blankets to give your baby this extra support. The car seat should be installed in the back seat. You can have a friend or family member ride in the back seat with your baby to watch them. Your baby should start off in a rear-facing car seat.
 Ask your doctor when it’s safe to move your baby to a forward-facing car seat. Never leave your baby alone in the car, not even for a few minutes.
Ask your doctor when it’s safe to move your baby to a forward-facing car seat. Never leave your baby alone in the car, not even for a few minutes.
Things to consider
If your baby is born premature, there are certain things that can affect his or her health, learning, and your family’s schedule. Babies born prematurely may need to stay in the hospital longer than full-term babies. They may be in a special section of the hospital called the NICU (newborn intensive care unit). This hospital stay can be a strain on your family’s routine. It requires daily visits to the hospital until the baby is released. If you have other children, it requires dividing your time between the hospital and caring for your children at home. One or both parents may need to take additional time away from work during this period.
Once your baby comes home, you will need to protect them from exposure to others and illness. Germs and illness can be tougher on a premature baby. Finally, some premature babies struggle with learning, gross motor (crawling, walking), and fine motor (picking up things, feeding themselves) development. They will eventually catch up. However, it may take them longer to learn those skills.
Finally, some premature babies struggle with learning, gross motor (crawling, walking), and fine motor (picking up things, feeding themselves) development. They will eventually catch up. However, it may take them longer to learn those skills.
Questions to ask your doctor
- If my first baby was born premature, does that increase the risk for prematurity for additional babies?
- How can I help my premature baby catch up on his or her developmental milestones?
- How long should I wait to take my premature baby out or expose them to others once we’re home?
- Can being born premature increase my baby’s risk of cerebral palsy or other chronic health conditions?
Resources
March of Dimes: Premature Babies
National Institutes of Health, MedlinePlus: Premature Babies
Copyright © American Academy of Family Physicians
This information provides a general overview and may not apply to everyone. Talk to your family doctor to find out if this information applies to you and to get more information on this subject.
Talk to your family doctor to find out if this information applies to you and to get more information on this subject.
A Guide to Premature Baby Feeding and Preemie Nutrition
A Guide to Premature Baby Feeding and Preemie Nutrition
When it comes to premature baby feeding, you may have questions. Whether you're breastfeeding or formula feeding, learn more about preemie baby nutrition and your baby's feeding schedule.
Premature baby feeding
- Premature babies need to eat at least every three hours. Tiny babies have tiny tummies. This means they’ll have to eat a lot of small meals for them to gain weight.
- Your baby will eat at their own pace. While they may be eating every three hours, the premature baby feeding process is often slow. You'll soon recognize their pattern of swallowing and breathing. Babies who eat slowly seem to take more milk at each feeding and may be satisfied and sleep longer between feedings.
- Their mouths are often extra-sensitive. If your baby has spent their first few days with tubes and respirators in their mouth, they may assume that anything that goes into their mouth is painful, which could include a breast or a bottle.
- Premature babies are slow to feed. Feeding them too fast by mouth may result in a feeding aversion or spitting up. They are also likely to have more digestive issues than a full-term baby, since their digestive system may not be as mature as a full-term baby's.
Try these premature baby feeding tips
- Each baby is unique. Follow the advice of your baby's doctor.
- Introduce your baby to a nipple. Even if they are still feeding by tube, this will help them adjust to bottle-feeding when they’re ready. You may need to try different nipples at first.
- Stick to breast milk or one type of formula and nipple to help them adjust.
- Keep a record of your baby's feedings.

- Get growth charts, specially designed for premature babies, from your baby's doctor to help monitor their progress.
- Keep your baby on a fairly regular schedule of awake and nap time, to help them eat better.
- Make sure your baby is fully awake before feeding.
- Don't force your baby to eat. If they’re not sucking as fast, sealing their lips or turning away, they may be full.
- Feed them on demand, not a schedule. Studies have shown that premature babies grew at a faster pace when fed on demand.
- When your baby is developmentally ready, slowly introduce solid foods while they are still on formula.
- Enlist the help and support of family and friends, to give yourself a break.
Preemie Nutrition
Most premature babies have low birth weight.
If a baby is too premature to breastfeed, moms are encouraged to pump their milk, as breast milk is considered to be best for the baby. Sometimes, doctors will recommend using a breast milk fortifier, to help give your baby the extra protein, vitamins, calcium and other nutrients they need at this early stage.
If you can't pump or breastfeed, or choose not to, ask your baby’s doctor about the specially designed formulas available for premature or low birth weight babies.
Premature babies may have more digestive issues than full-term babies.
Chances are, your baby’s feeding skills haven't fully developed yet. This means they’ll likely be slow to feed, or they may feed too fast and spit up or develop a feeding aversion. But there are some things you can try to help:
- Introduce your baby to a pacifier. This can help get them used to the feeling of bottle-feeding for when they’re ready to switch over from the tube.
- Record their feedings, so you can keep track of spit ups and how much they’re keeping down.
- Monitor your preemie’s progress with growth charts from the doctor.
- Try to keep them on a sleep schedule.
- Make sure they are fully awake before feeding
- Be aware of indicators, so you know when your little one is full or tired.
- Slowly introduce solids when they are developmentally ready.
Babies who are born premature often undergo developmental testing and programs.
If your baby weighs less than 3.5 lbs. at birth, they will most likely be referred for formal developmental testing around their 1st and 2nd birthdays. If your baby is born prematurely, your doctor may recommend an infant stimulation program. This usually involves working with a physical therapist or specialized healthcare professional to learn gentle exercises, positioning and other ways to interact with your premature baby and help them with physical development. Early intervention programs can help with social and functional skills and provide support for the family.
Preterm babies have a harder time maintaining the proper water balance in their bodies. These babies can become dehydrated or over-hydrated. This is especially true for very premature infants. Keep the following preemie nutrition facts in mind as you navigate feeding your baby:
- Premature babies may experience more water loss through the skin or respiratory tract than babies born at full term.
- The kidneys in premature babies have not grown enough to control water levels in the body.
- The NICU team keeps track of how much premature babies urinate (by weighing their diapers) to make sure that their fluid intake and urine output are balanced.
- Human milk from the baby's own mother is the best for babies born early and at very low birth weight.
- Human milk can help babies avoid infections and sudden infant death syndrome (SIDS) as well as necrotizing enterocolitis (NEC).
- Many NICUs will give donor milk from a milk bank to high-risk babies who are not able to get adequate amounts of milk from their own mother.
- Special preemie formulas can also be used. These formulas have more added calcium and protein to meet the special growth needs of premature babies.
- Older premature babies (34 to 36 weeks gestation) may be switched to regular formula or a transitional formula.

- Babies who are given breast milk may need a supplement called human milk fortifier mixed into their feedings. This gives them extra protein, calories, iron, calcium, and vitamins. Babies fed formula may need to take supplements of certain nutrients, such as vitamins A, C, and D, and folic acid.
- Some infants will need to continue taking nutritional supplements after they leave the hospital. For breastfeeding infants, this may mean a bottle or two of fortified breast milk per day as well as iron and vitamin D supplements. Some babies will need more supplementation than others. This may include babies who are not able to consume adequate amounts of milk through breastfeeding to get the calories they need to grow well.
- After each feeding, babies should seem satisfied. They should have 8 to 10 feedings and at least 6 to 8 wet diapers each day. Watery or bloody stools or regular vomiting could indicate an issue and you should discuss them with your doctor.
Preemie Weight Gain
Weight gain is monitored closely for all babies. Research suggests developmental delays could be associated with premature babies who experience slow growth.
- In the NICU, babies are weighed every day.
- It is normal for babies to lose weight in the first few days of life. Most of this loss is water weight.
- Most premature infants should start gaining weight within a few days of birth.
- The desired weight gain depends on the baby's size and gestational age. Sicker babies may need to be given more calories to grow at the desired rate.
- It might be as little as 5 grams a day for a tiny baby at 24 weeks, or 20 to 30 grams a day for a larger baby at 33 or more weeks.
- In general, a baby should gain about a quarter of an ounce each day for every pound (about 1/2 kilogram) they weigh. (This is equal to 15 grams per kilogram per day. It is the average rate at which a fetus grows during the third trimester).

If you are experiencing difficulty affording specialty premature formulas for your baby, financial assistance is available.
Enfamil has developed a program called Helping Hand for Special Kids, to help families who need specialty formulas for their premature baby but have difficulty affording them. Depending on your needs, the Helping Hand program provides either long-term assistance or a free, one-time shipment of products. To us, all babies deserve the very best start in life. Ask your doctor if you qualify for this program.
You may also like
Your baby was born prematurely | Regional Perinatal Center
Premature babies
If your baby is born too early, the joy of having a baby can be overshadowed by health concerns and thoughts about the possible consequences.
Instead of returning home with the baby, holding him and caressing him, you will have to stay in the department, learn to cope with the fear of touching the baby, realize the need for treatment and various manipulations, get used to the complex equipment that surrounds him. nine0005
nine0005
In this situation, not only your baby needs help, you need it too! The best assistants are your loved ones, their love and care, as well as professional advice and recommendations from doctors and psychologists. This section of articles will help you improve your knowledge of preterm infant care, development and nutrition.
Your help for the baby
Previously, parents were often not allowed into the neonatal unit and, especially, into the intensive care unit because of the fear of infection of the baby, but now the contact of the parent with the child is recognized as desirable and is prohibited only in exceptional cases (for example, if parents have acute infections)
Close communication between you and your baby is very important from the first days of his life. Even very immature premature babies recognize the voices and feel the touch of their parents.
The newborn needs this contact. Studies have shown that it greatly contributes to the faster adaptation of an immature child to new conditions and the stabilization of his condition. The baby's resistance to therapy increases, he absorbs large amounts of food and quickly begins to suck on his own. Contact with the child is important for parents. Taking part in the care of the baby, they feel their involvement in what is happening and quickly get used to a new role, especially when they see how he reacts to their presence. nine0005
The baby's resistance to therapy increases, he absorbs large amounts of food and quickly begins to suck on his own. Contact with the child is important for parents. Taking part in the care of the baby, they feel their involvement in what is happening and quickly get used to a new role, especially when they see how he reacts to their presence. nine0005
By constantly and attentively observing the baby, parents can notice the smallest changes in his condition before others. In addition, communication in the hospital is a good practice that will undoubtedly come in handy after discharge. For parents, early physical contact with the baby is very valuable, because it allows them to feel him, despite the incubator and other obstacles, and show him their love.
Treatment in the neonatal intensive care unit requires parents to have full confidence in all medical staff. nine0005
Nursing premature babies in the hospital
Many premature babies cannot breathe, suckle and regulate their body temperature sufficiently after birth. Only in the last weeks of pregnancy is the maturation of the lungs, gastrointestinal tract, kidneys, brain, which regulates and coordinates the work of all organs and systems.
Only in the last weeks of pregnancy is the maturation of the lungs, gastrointestinal tract, kidneys, brain, which regulates and coordinates the work of all organs and systems.
Fluid loss due to the immaturity of the skin of premature babies and the insufficiency of thermoregulation processes require constant attention. Modern approaches focused on nursing premature babies help to cope with these problems. nine0005
Heat regulation incubator
Premature babies are very susceptible to temperature fluctuations. At the same time, clothing can interfere with the monitoring of the baby's condition and its treatment. That is why an incubator is used to provide the conditions necessary for premature babies. It maintains a certain temperature and humidity, which change as the child grows. When the body weight of a premature infant reaches 1500-1700 g, he can be transferred to a heated bed, and after reaching a weight of 2000, most premature babies can do without this support. There are no strict rules here: when nursing children with low body weight, doctors are guided by the severity of the condition of each premature baby and its degree of maturity. nine0005
There are no strict rules here: when nursing children with low body weight, doctors are guided by the severity of the condition of each premature baby and its degree of maturity. nine0005
In incubators, very young premature babies are placed in special "nests" - soft hemispheres in which the baby feels comfortable and assumes a position close to intrauterine. It must be protected from bright lights and loud noises. For this purpose, special screens and coatings are used.
Critical treatments during the first days of life of premature babies with low and very low birth weight:
Use of an incubator or heated bed. nine0005
Oxygen supply for respiratory support.
If necessary, artificial ventilation of the lungs or breathing using the CPAP system.
Intravenous administration of various drugs and fluids.
Carrying out parenteral nutrition with solutions of amino acids, glucose and fat emulsions.
Don't worry: not all premature babies need such extensive treatment!
Mechanical ventilation and CPAP for respiratory support
When it comes to nursing, oxygen supply is of the utmost importance for premature babies. In a child born before the 34-35th week of pregnancy, the ability of the lungs to work independently is not yet sufficiently developed. The use of a constant flow of air with oxygen, which maintains a positive airway pressure (CPAP), leads to an increase in blood oxygen saturation.
In a child born before the 34-35th week of pregnancy, the ability of the lungs to work independently is not yet sufficiently developed. The use of a constant flow of air with oxygen, which maintains a positive airway pressure (CPAP), leads to an increase in blood oxygen saturation.
This new method made it possible for the majority of even very immature children to do without mechanical ventilation. The need for intubation of children has disappeared: during treatment with CPAP, oxygen is supplied through short tubes - cannulas that are inserted into the nasal passages. CPAP or mechanical ventilation is continued until the lungs can function at full capacity on their own. nine0005
In order for the lungs to expand and remain in such a state in the future, a surfactant is needed - a substance that lines the alveoli from the inside and reduces surface tension. Surfactant is produced in sufficient quantities starting from the 34-35th week of pregnancy. Basically, it is by this time that the formation of the lungs is completed. If the baby was born earlier, modern technologies allow the introduction of surfactant into the lungs of premature babies immediately after their birth.
If the baby was born earlier, modern technologies allow the introduction of surfactant into the lungs of premature babies immediately after their birth.
Parenteral nutrition - administering nutrient solutions by vein
Premature babies, especially those born weighing less than 1500 g, are not able to get and absorb enough nutrients, even when fed through a tube. For the rapid growth of the baby, a large amount of nutrition is needed, and the size of the stomach is still very small, and the activity of digestive enzymes is also reduced. Therefore, such children are given parenteral nutrition.
Special nutrients are injected into a vein using infusion pumps that deliver solutions slowly at a predetermined rate. In this case, amino acids necessary for building proteins, fat emulsions and glucose, which are sources of energy, are used. These substances are also used for the synthesis of a number of hormones, enzymes and other biologically active substances. Additionally, minerals and vitamins are introduced. nine0005
Additionally, minerals and vitamins are introduced. nine0005
Gradually, the volume of enteral nutrition increases, and parenteral nutrition decreases until it is completely canceled.
Premature infants with gastrointestinal disease require parenteral nutrition for a longer period of time.
By the time your grown baby is discharged from the hospital, everything should be well prepared at home. And this applies not only to the environment, clothes and means of caring for the child.
All family members must be ready to receive the baby. Of course, the main care will fall on the shoulders of the parents. Although you have already gained some experience in the hospital, it is important to feel the support of others, especially in the early days.
Older children can also help. The discharge of your baby is a great joy that you want to share with all your relatives.
While you are getting used to your new role, it is important that nothing distracts you from communicating with your child. Now all the care and responsibility for the baby lies entirely with you. Everything you need to take care of him should be at hand. nine0005
Now all the care and responsibility for the baby lies entirely with you. Everything you need to take care of him should be at hand. nine0005
Preparing for discharge from the hospital
Before discharge, you must make sure that:
- Prepared the crib, bath for bathing and a place for changing clothes, preferably a changing table. A crib should be placed in the parents' bedroom, the child should not be left alone even at night. A stroller is also required. you have baby milk that was recommended by the doctor before discharge (if the child is on mixed or artificial feeding). As a rule, this is a specialized medical product. You need a certain number of small bottles and teats of the appropriate size, as well as a sterilizer. All premature babies will need pacifiers. nine0126
- You have fully mastered breastfeeding or bottle feeding.
- If your baby is not suckling all the required amount of milk from the breast and is supplementing from a bottle, you have purchased a breast pump that you have learned to use; you may also need it if you have a lot of breast milk.
- You have asked your doctor how often your child's weight should be monitored.
- If your baby still needs medication, you have the required amount at home. And you know exactly how and when to give them to your child. nine0126
- You know which warning signs to look out for.
- After the baby is discharged, a pediatrician and a neonatologist will look after the baby, to whom you will give the discharge summary from the hospital.
- You know how the hospital from which your child is being discharged will provide follow-up care after discharge.
- You know which specialists and how often should examine your baby (oculist, neuropathologist, etc.). nine0126
- All the emergency phone numbers you need are at your fingertips.
When can a child go home
This question is very difficult to answer because all children are different. The stay in the hospital can last from 6 days to 6 months, depending on the degree of prematurity of the child, the severity of his condition, as well as the presence of certain complications.
Of course, all parents look forward to the moment when the baby can be brought home. Long-term nursing of a premature baby is often a difficult test for you. But we must not forget that safety comes first, and the baby can be discharged home only when the doctors are confident in the stability of his condition. It is certainly in your interest as well. nine0005
The rate of increase in body weight and length
Weight gain is the main indicator of the growth of the baby and the adequacy of the treatment. The weight of the child, especially in the first days and weeks of life, is influenced by a number of factors: the presence of milk in the stomach (immediately after feeding), the time of bowel movement, the degree of filling of the bladder, the presence of edema. Therefore, if an edematous child does not gain weight for several days, and perhaps even loses it, do not worry. It should be remembered that children grow unevenly and periods of high weight gain alternate with lower ones.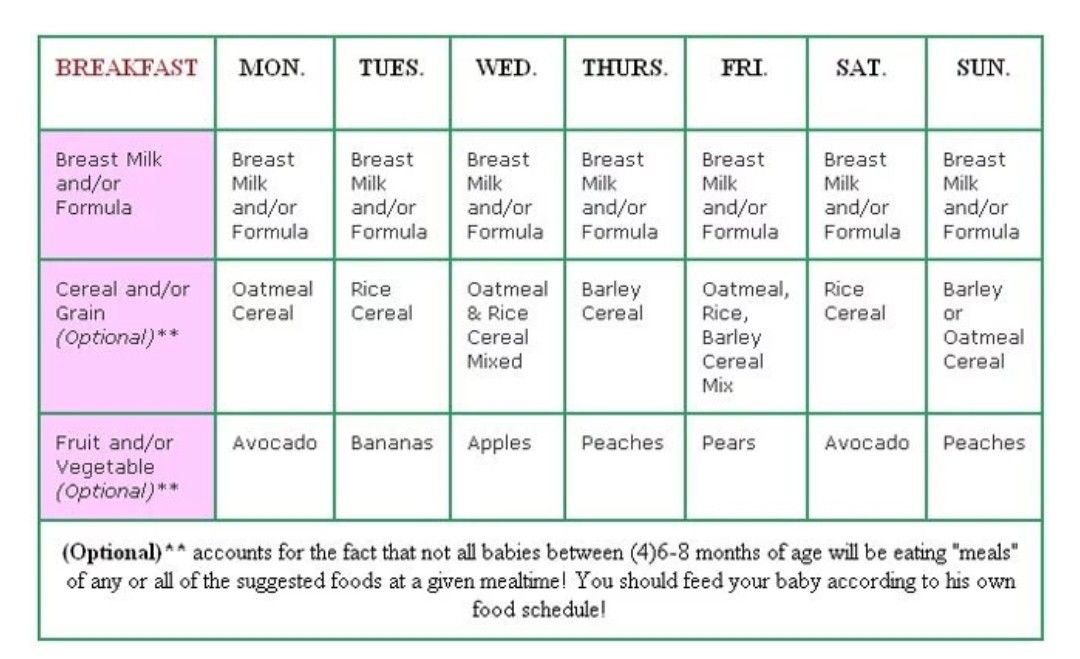 It is better to focus not on weight gain per day, but on the dynamics of this indicator over several days or a week. nine0005
It is better to focus not on weight gain per day, but on the dynamics of this indicator over several days or a week. nine0005
It is currently accepted that in the interval corresponding to 28-34 weeks of pregnancy, the normal weight gain of the child is 16-20 g/kg per day. Then it is reduced to 15 g/kg.
It is also important to take into account the rate of increase in body length. With malnutrition, at first the child gains less weight (or even loses it), and with a more pronounced deficiency of nutrients, his growth is also disturbed.
The weight must not only increase at a certain rate, but must also correspond to the length of the baby. An important parameter characterizing the development of the baby is an increase in the circumference of the head. The brain most actively increases in size during the first 12–18 months of life. But an excessively rapid increase in head circumference, as well as a slowdown in its increase, indicate neurological disorders. nine0005
A premature baby can be discharged from the hospital if:
- he is able to independently maintain the required body temperature;
- does not need breathing support and constant monitoring of the work of the respiratory and cardiovascular systems;
- can suck out the required amount of nutrition on its own;
- does not need round-the-clock monitoring and frequent determination of biochemical or other indicators; nine0126
- supportive care can be provided at home;
- he will be under the supervision of a local pediatrician and neonatologist at the place of residence.

The decision to discharge home is made for each patient individually. In addition to the state of health of the baby, the degree of preparedness of parents, their ability to provide high-level care for a premature baby is also taken into account.
Feeding a premature baby after discharge
Breastfeeding is the ideal way to feed premature babies.
However, if the baby was born much prematurely and his birth weight did not exceed 1800-2000 g, his high nutritional requirements cannot be met by breastfeeding. The growth rate will be insufficient. Moreover, over time, the content of many nutrients, including protein, in milk decreases. And it is the main material for building organs, and primarily brain tissue. Therefore, proteins must be supplied to the body of a premature infant in the optimal amount. nine0005
In addition, premature babies have a significantly increased need for calcium and phosphorus, which are essential for bone formation.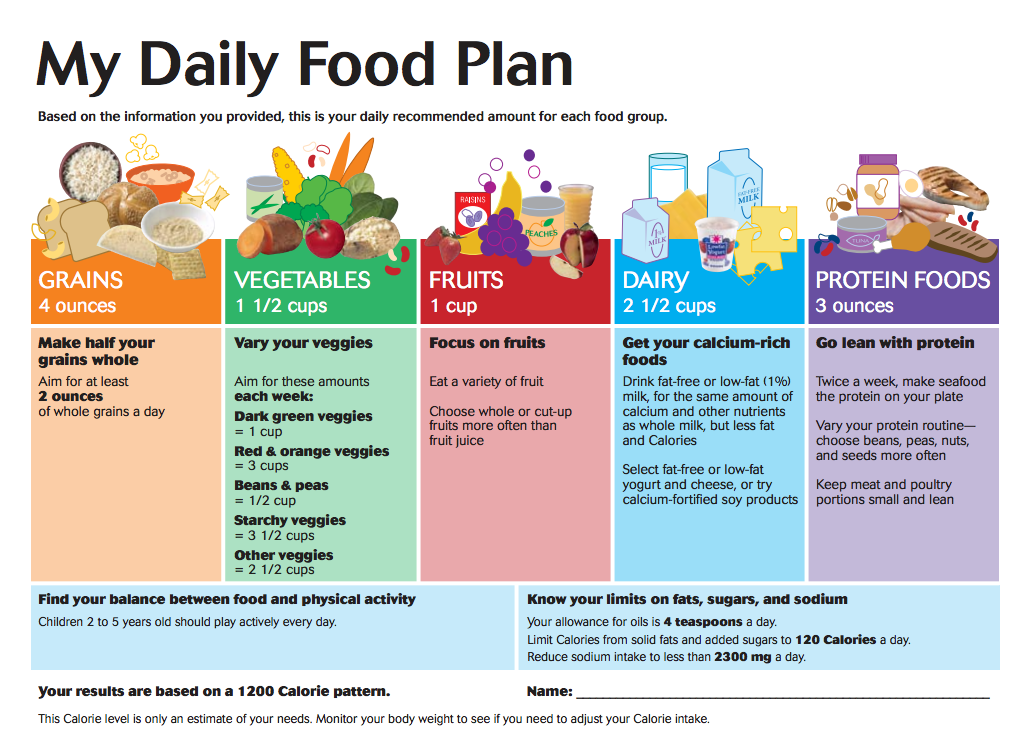
In order for the baby's nutrition to be complete even after being discharged from the hospital, special additives - "enrichers" are introduced into breast milk in a certain amount, already less than in the hospital. They make up for the lack of protein in it, as well as some vitamins and minerals. As a result, the child receives them in the optimal amount. The duration of their use will be determined by your doctor. If there is not enough milk or it does not exist at all, children born prematurely should be transferred to artificial feeding. Complementary feeding of premature babies is carried out with special children's dairy products designed for children with low birth weight. This baby milk is ideally suited to both the ability of immature children to digest and assimilate nutrients, and their needs. nine0005
Premature infant milk contains more protein, fat and carbohydrates than term infant milk, resulting in a higher calorie content. In specialized baby milk, the concentration of many minerals is higher, especially iron, zinc, calcium, phosphorus, as well as vitamins, including vitamin D. Long-chain polyunsaturated fatty acids of the Omega-3 and Omega-6 classes are introduced into such products, which are necessary for proper development of the brain and organ of vision, as well as nucleotides that contribute to the optimal development of immunity. However, when the child reaches a certain weight (2000-2500 g), you should gradually switch to feeding with standard baby milk, but not completely. Specialized baby milk can be present in the diet of a premature baby for several months. This time, as well as the volume of the product, will be determined by the doctor. He will answer all your questions about how to feed your baby. nine0005
Long-chain polyunsaturated fatty acids of the Omega-3 and Omega-6 classes are introduced into such products, which are necessary for proper development of the brain and organ of vision, as well as nucleotides that contribute to the optimal development of immunity. However, when the child reaches a certain weight (2000-2500 g), you should gradually switch to feeding with standard baby milk, but not completely. Specialized baby milk can be present in the diet of a premature baby for several months. This time, as well as the volume of the product, will be determined by the doctor. He will answer all your questions about how to feed your baby. nine0005
At present, specialized children's dairy products have been developed and are being used to feed premature babies after discharge from the hospital. In its composition, it occupies an intermediate position between a specialized product for premature babies and regular baby milk. Your baby will be transferred to such baby milk while still in the hospital. You will continue to give it to your child at home, and the doctor, watching him, will tell you when it will be possible to switch to regular standard baby milk. If the baby was born with a very low body weight or is not gaining weight well, special baby milk can be used for a long time - up to 4 months, 6 or even 9months. The beneficial effect of such children's dairy products on the growth and development of the child has been proven in scientific studies.
You will continue to give it to your child at home, and the doctor, watching him, will tell you when it will be possible to switch to regular standard baby milk. If the baby was born with a very low body weight or is not gaining weight well, special baby milk can be used for a long time - up to 4 months, 6 or even 9months. The beneficial effect of such children's dairy products on the growth and development of the child has been proven in scientific studies.
Feeding needs for premature babies
Higher caloric intake because they need to gain weight faster than term babies.
More protein as premature babies grow faster.
More calcium and phosphorus for bone building.
More trace elements and vitamins for growth and development. nine0005
A premature baby grows faster than a term baby. Nutrition for such children is calculated taking into account body weight at birth, the age of the baby and its growth rate. As a rule, the calorie content of the daily diet is about 120-130 calories per 1 kg of body weight.
It is very important that your baby continues to gain weight quickly and grow in length after discharge. To do this, feeding premature babies must be carried out using a specialized fortified diet prescribed by a doctor. nine0005
Feeding premature babies | Breastfeeding premature babies
Premature babies have a special need for breast milk, but it can be difficult to breastfeed them directly. Our expert advice will help you provide your premature baby with healthy breast milk.
Share this information
Professor Katsumi Mizuno, Department of Pediatrics, Showa University Koto Toyosu Hospital:
Katsumi is a Certified Breastfeeding Consultant, Professor of Pediatrics at Showa Medical University and one of the leading neonatologists in Japan. His research focuses on neonatal suckling skills, breast milk banking, and the use of breast milk for feeding premature babies in neonatal intensive care units.
Babies born before the 37th week of pregnancy are considered premature. 1 The causes of preterm birth are not always obvious, but certain factors increase the likelihood of such an event. These include: twin or multiple pregnancy, certain diseases of the mother or fetus, as well as a history of premature birth. nine0005
1 The causes of preterm birth are not always obvious, but certain factors increase the likelihood of such an event. These include: twin or multiple pregnancy, certain diseases of the mother or fetus, as well as a history of premature birth. nine0005
Because premature babies spend less time in the womb, they are not mature enough and may be more susceptible to infection and disease. They often require hospitalization in the neonatal intensive care unit.
Why is breast milk so important for premature babies?
Breast milk is essential for optimal growth and development of term babies, but it is even more important for premature babies.
During pregnancy, the fetus receives important substances from the mother through the placenta, such as DHA (a fatty acid essential for brain and eye development) and immunoglobulin G (an antibody). nine0242 2.3 A premature baby did not receive all of these substances. However, the milk produced by a premature mother contains more fat and secretory immunoglobulin than mothers of full-term babies. 4
4
In addition, premature babies have an underdeveloped gastrointestinal tract, which can make digestion and absorption of nutrients difficult, so they need food that their sensitive stomach and intestines can easily digest. Breast milk contains enzymes that make it easier for the baby to digest, 5 as well as epidermal growth factor, which accelerates the development of the gastrointestinal tract 6 . Premature infants who are predominantly breastfed have much lower intestinal permeability than formula-fed infants, meaning fewer potentially harmful particles from the stomach and intestines enter their bloodstream. 7
Breast milk is so important for premature babies that if the baby's mother does not produce enough breast milk at first for any reason, it is recommended that the deficiency be replenished with donor milk rather than formula. nine0005
Does breast milk improve the condition of premature babies?
Breast milk contains protective substances that can prevent serious diseases that preterm infants are susceptible to, 8 such as severe infections, 9 retinopathy of prematurity (which can cause vision loss) 10 and bronchopulmonary dysplasia (chronic lung disease). 11
11
The more milk your baby gets, the lower the risk of developing diseases. nine0242 12 Every additional 10 ml of milk per kilogram of body weight per day reduces the risk of sepsis by 19%. 9 The risk of developing necrotizing enterocolitis (a potentially fatal bowel disease) in premature infants who are breastfed is ten times lower than those who are formula fed. 13 That's why every drop counts!
Most importantly, preterm infants who are breastfed are typically discharged an average of two weeks earlier than formula-fed infants. nine0242 14 They also have a 6% lower risk of readmission in the first year of life. 15
Breast milk has been proven to have a beneficial effect on mental and physical development in the long term. Studies show that low-birth-weight babies who are breastfed in the neonatal intensive care unit have an average IQ of up to five points higher than those who are not breastfed. 15 In addition, their cardiovascular system works better during their lifetime. nine0242 17
15 In addition, their cardiovascular system works better during their lifetime. nine0242 17
Will milk be produced if the baby was born prematurely?
Yes, the mother's body is ready to produce milk by the middle of pregnancy. After the baby is born and the placenta is born, the level of progesterone, the pregnancy hormone, drops, and the production of colostrum, the first milk, starts in the breast. This usually happens after the newborn is put to the breast and begins to suckle rhythmically, but if the baby was born prematurely, he most likely will not be able to latch on at first. nine0005
To replicate the sensations that trigger milk production, you can manually stimulate the breasts and nipples, or use a breast pump to express nutrient-rich colostrum for your baby. 18 Read below for more information on what to do if your premature baby is not yet able to breastfeed.
Breast milk usually comes in two to four days after birth, but if it was premature, the milk supply may be delayed. However, a recent study shows that moms who started pumping within one hour of giving birth had milk coming in as expected. nine0242 19 This is why it is important to start expressing breast milk as early as possible.
However, a recent study shows that moms who started pumping within one hour of giving birth had milk coming in as expected. nine0242 19 This is why it is important to start expressing breast milk as early as possible.
How to prepare if the baby is expected prematurely?
Visit the neonatal intensive care unit to see how it works and how premature babies are cared for. In addition, it will be useful to learn how breast milk is produced and secreted and why it is not only a healthy food, but also an important medicine for premature babies. Read more about this in our free e-book Surprising Breast Milk Facts .
What if a premature baby cannot breastfeed?
Many babies born before 34 weeks have difficulty coordinating sucking, swallowing and breathing. Until the baby masters these skills, nurses will feed him through a tube that is inserted into the nose or mouth and provides food directly into the stomach. In this way, the baby can be fed continuously until he is ready to breastfeed.
If your baby is too weak to latch on and suckle milk, you can use a breast pump* available at the hospital or maternity hospital to “do the job for the baby”. Breast stimulation with research-based technology, 20 reproduces the rhythm of the suckling of the baby, plays an important role in starting and maintaining milk production in the first hours after childbirth 21 .
Milk should be expressed at the same frequency as term infants are usually fed every two to three hours, i.e. 8 to 12 times a day.
You can try putting a small amount of expressed breast milk into the baby's mouth with a syringe, or putting milk-soaked cotton swabs in the baby's mouth. 22 This way your baby will recognize the taste of your milk, which will facilitate the transition to breastfeeding in the future. In addition, the protective substances that make up breast milk will help strengthen the local immunity of the baby's oral cavity. You can be involved in the care of your premature baby in a variety of ways - check with your healthcare provider for details.
Very low birth weight babies - less than 1.5 kg - usually need extra protein, calcium and phosphorus, so they are given fortified breast milk. In some countries, such additives are made on human milk, and, for example, in Japan, on cow's milk. nine0005
Recommendations for pumping milk
If the baby will be in the neonatal intensive care unit for a long time, neonatologists recommend using a double breast pump for pumping. I always recommend Medela Symphony*. Double pumping not only speeds up the process, but also produces an average of 18% more milk than pumping from each breast in turn. 23
In addition, I advise you to create the most comfortable conditions for pumping. It is generally agreed that it is best to express milk during or after prolonged skin-to-skin contact with the baby (more on this "kangaroo method" below). Another good option is to sit next to the crib and watch your baby while he pumps. Oxytocin (the hormone that stimulates milk flow) is released when you look at your baby, touch him, smell him and think about him, 24 Therefore, comfortable and calm conditions must be created for this in the neonatal intensive care unit.
What is kangaroo care for premature babies?
The so-called kangaroo method involves prolonged skin-to-skin contact between parents and infant. This is extremely beneficial for you and your baby, as well as for milk production. Skin-to-skin contact normalizes the baby's breathing and heartbeat, keeps him warm and allows him to be as close to the parent as possible. Kangaroo care is believed to have a beneficial effect on the health of premature babies, 25 and it helps mothers express more milk 26 and breastfeed longer. 27 Skin-to-skin contact 30-60 minutes before feeding gives baby time to wake up and be hungry so he can eat without being forced.
What if the neonatal intensive care unit offers formula feeding?
Feel free to state that you want to breastfeed your baby instead of formula. If you don't have enough breast milk to feed your baby, ask the ward for help to increase your milk supply. nine0005
It is natural for mothers whose babies are in the neonatal intensive care unit to experience anxiety and stress. Sometimes these experiences interfere with milk production, so it's important to ask for any help you may need. Remember that you have the right to seek support. Your healthcare provider may be able to recommend a suitable lactation specialist, such as a lactation consultant, for you.
Sometimes these experiences interfere with milk production, so it's important to ask for any help you may need. Remember that you have the right to seek support. Your healthcare provider may be able to recommend a suitable lactation specialist, such as a lactation consultant, for you.
How to switch from pumping to breastfeeding? nine0248
At whatever gestational age a baby is born, as long as the baby is stable enough for skin-to-skin contact, it can seek the breast for sedative suckling. This is the perfect way for your baby to learn sucking skills before they learn to coordinate sucking, swallowing and breathing.
Babies love the smell of breast milk, so you can put some milk on the nipple before you put your baby to the breast to make him want to suckle. He might even be able to suck some milk. Don't worry if your baby seems to suck very little - he learns every time. He can start with one or two sips and gradually move on to full breastfeeding. Until then, the baby can be fed through a tube, pressed to the breast, so that the taste of milk and touching the breast is associated with a feeling of satiety. nine0005
nine0005
You can put your baby to the breast for sedative suckling as soon as you are ready for kangaroo care, unless your baby is suffering from bradycardia (slow heartbeat) or low oxygen levels in the blood. You can switch to breastfeeding as soon as the baby is ready for it. Gradually, he will gain enough strength to suckle longer and suck out more milk.
Literature
1 World Health Organization. Geneva, Switzerland; 2018. Media Centre: Preterm birth fact sheet; November 2017 [03/26/2018]. Available from : http://www.who.int/mediacentre/factsheets/fs363/en/ - World Health Organization Geneva, Switzerland; 2018. "Media Center: Prematurity Fact Sheet"; November 2017 [3/26/2018]. Article at: http://www.who.int/mediacentre/factsheets/fs363/en/
2 Duttaroy AK. Transport of fatty acids across the human placenta: a review. nine0315 Prog Lipid Res . 2009;48(1):52-61. - Duttaroy A.K., "Transfer of fatty acids across the human placenta: a review". Prog Lipid Res. 2009;48(1):52-61.
2009;48(1):52-61. - Duttaroy A.K., "Transfer of fatty acids across the human placenta: a review". Prog Lipid Res. 2009;48(1):52-61.
3 Palmeira P et al. IgG placental transfer in healthy and pathological pregnancies. Clin Dev Immunol. 2012;2012: 985646. - Palmeira P. et al., Placental transfer of immunoglobulin
5 Pamblanco M et al. Bile salt - stimulated lipase activity in human colostrum from mothers of infants of different gestational age and birthweight. Acta Paediatr. 1987;76(2):328-331. - Pamblanco M. et al., "Bile salt-activated lipase and its activity in colostrum of mothers of infants of various gestational ages and birth weights." Akta Pediatr. 1987;76(2):328-331.
6 Dvorak B. Milk epidermal growth factor and gut protection. J Pediatr. 2010;156(2): S 31-35. - Dvorak B. , "Epidermal growth factor in milk and gut protection". F Pediatrician (Journal of Pediatrics). 2010;156(2):S31-35.
, "Epidermal growth factor in milk and gut protection". F Pediatrician (Journal of Pediatrics). 2010;156(2):S31-35.
7 Taylor SN et al. Intestinal permeability in preterm infants by feeding type: mother's milk versus formula. Breastfeed Med . 2009;4(1):11-15.- Theilon S.N. et al., "Intestinal permeability in preterm infants and its association with type of feeding: breast milk or formula." Brestfeed Med (Breastfeeding Medicine). 2009;4(1):11-15.
8 Newburg DS. Innate immunity and human milk. J Nutr . 2005;135(5):1308-1312. — Newburgh, D.S., "Natural Immunity and Breast Milk." F Nut. 2005;135(5):1308-1312. nine0315
9 Patel AL et al. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J Perinatol . 2013;33(7):514-519. - Patel A.L. et al., "Impact of early breast milk on sepsis and health care costs in extremely low birth weight infants". Zh Perinatol (Journal of Perinatology). 2013;33(7):514-519.
- Patel A.L. et al., "Impact of early breast milk on sepsis and health care costs in extremely low birth weight infants". Zh Perinatol (Journal of Perinatology). 2013;33(7):514-519.
10 Zhou J et al . Human milk feeding as a protective factor for retinopathy of prematurity: a meta-analysis. Pediatrics. 2015;136(6): e 1576-1586. - Zhou Q. et al., "Breastfeeding as a protective factor against retinopathy of prematurity: a meta-analysis." Pediatrix (Pediatrics). 2015;136(6):e1576-1586.
11 Patel AL et al. Influence of own mother's milk on bronchopulmonary dysplasia and costs. Arch DIS Child FETAL Neonat 2017;102(3): F 256- F 261. - Patel A.L. et al., "Effect of breast milk on bronchopulmonary dysplasia and health care costs." Arch Dis Child Fetal Neonate Ed. 2017;102(3): F 256- F 261.
- Patel A.L. et al., "Effect of breast milk on bronchopulmonary dysplasia and health care costs." Arch Dis Child Fetal Neonate Ed. 2017;102(3): F 256- F 261.
12 Meier PP et al . Improving the use of human milk during and after the NICU stay. Clin Perinatol. 2010;37(1):217-245. - Meyer P.P. et al., "Optimizing the use of breast milk during and after a stay in the neonatal intensive care unit." nine0315 Perinatol wedge. (Clinical perinatology). 2010;37(1):217-245.
13 Lucas A, Cole TJ. Breast milk and neonatal necrotizing enterocolitis. Lancet. 1990;336(8730-8731):1519-1523. — Lucas A, Cole TJ, "Breast milk and neonatal necrotizing enterocolitis." Lancet 1990;336(8730-8731):1519-1523.
14 Schanler RJ et al. Randomized trial of donor human milk versus preterm formula as substitutes for mothers' own milk in the feeding of extremely premature infants. nine0315 Pediatrics. 2005;116(2):400-406. - Chanler R.J. et al., "Randomized Trial of Donor Human Milk Versus Prematurity Formula as a Breast Milk Substitute in Severely Preterm Infants". Pediatrix (Pediatrics). 2005;116(2):400-406.
Randomized trial of donor human milk versus preterm formula as substitutes for mothers' own milk in the feeding of extremely premature infants. nine0315 Pediatrics. 2005;116(2):400-406. - Chanler R.J. et al., "Randomized Trial of Donor Human Milk Versus Prematurity Formula as a Breast Milk Substitute in Severely Preterm Infants". Pediatrix (Pediatrics). 2005;116(2):400-406.
15 Vohr BR et al. Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birth weight infants at 18 months of age. nine0315 Pediatrics. 2006;118(1): e 115-123. - Thief B.R. et al., Developmental Beneficial Effects of Breast Milk in the Intensive Care Unit on Extremely Low Birth Weight Infants by 18 Months of Age. Pediatrix (Pediatrics). 2006;118(1):e115-123.
16 Victora CG et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. nine0315 2016;387(10017):475-490. - Victor S.J. et al., "Breastfeeding in the 21st century: epidemiology, mechanisms and long-term effects". Lancet (Lancet). 2016;387(10017):475-490.
Lancet. nine0315 2016;387(10017):475-490. - Victor S.J. et al., "Breastfeeding in the 21st century: epidemiology, mechanisms and long-term effects". Lancet (Lancet). 2016;387(10017):475-490.
17 Lewandowski AJ et al. Breast milk consumption in preterm neonates and cardiac shape in adulthood. Pediatrics. 2016;138(1): pii : e 20160050. - Lewandowski, A.J. et al., "Breastfeeding in preterm infants and cardiovascular health in adulthood." nine0315 Pediatrix (Pediatrics). 2016;138(1):pii:e20160050.
18 Meier PP et al. Which breast pump for which mother: an evidence-based approach to individualizing breast pump technology. J. Perinatol. 2016;36(7):493-499. - Meyer P.P. et al., Breastpump Selection: A Scientific Approach to Customizing Pumping Technology. J Perinatol (Journal of Perinatology). 2016;36(7):493-499.
19 Parker LA et al. Effect of early breast milk expression on milk volume and timing of lactogenesis stage II among mothers of very low birth weight infants: a pilot study. J Perinatol. 2012;32(3):205-209. - Parker L.A. et al., "Effect of early pumping on milk supply and timing of the second stage of lactogenesis in mothers of extremely low birth weight infants: a pilot study." J Perinatol (Journal of Perinatology). 2012;32(3):205-209.
Effect of early breast milk expression on milk volume and timing of lactogenesis stage II among mothers of very low birth weight infants: a pilot study. J Perinatol. 2012;32(3):205-209. - Parker L.A. et al., "Effect of early pumping on milk supply and timing of the second stage of lactogenesis in mothers of extremely low birth weight infants: a pilot study." J Perinatol (Journal of Perinatology). 2012;32(3):205-209.
20 Meier PP et al. Breast pump suction patterns that mimic the human infant during breastfeeding: greater milk output in less time spent pumping for breast pump-dependent mothers with premature infants. J Perinatol. 2012;32(2):103-110. - Meyer P.P. et al., "Pumping patterns that mimic breastfeeding behavior: more milk and less time for constantly pumping mothers of preterm infants." nine0315 J Perinatol (Journal of Perinatology). 2012;32(2):103-110.
21 Parker LA et al. Association of timing of initiation of breastmilk expression on milk volume and timing of lactogenesis stage II among mothers of very low-birth-weight infants. Breastfeed Med . 2015;10(2):84-91. - Parker L.A. et al., "Effect of early pumping on milk supply and timing of the second stage of lactogenesis in mothers of extremely low birth weight infants: a pilot study." nine0315 Brestfeed Med (Breastfeeding Medicine). 2015;10(2):84-91.
Association of timing of initiation of breastmilk expression on milk volume and timing of lactogenesis stage II among mothers of very low-birth-weight infants. Breastfeed Med . 2015;10(2):84-91. - Parker L.A. et al., "Effect of early pumping on milk supply and timing of the second stage of lactogenesis in mothers of extremely low birth weight infants: a pilot study." nine0315 Brestfeed Med (Breastfeeding Medicine). 2015;10(2):84-91.
22 Lee J et al. Oropharyngeal colostrum administration in extremely premature infants: an RCT. Pediatrics. 2015;135(2): e 357-366. - Lee J. et al., "Oropharyngeal colostrum ingestion in very preterm infants: a randomized controlled clinical trial." Pediatrix (Pediatrics). 2015;135(2):e357-366. nine0315
23 Prime PK et al. Simultaneous breast expression in breastfeeding women is more efficacious than sequential breast expression. Breastfeed Med 2012; 7(6):442–447. - Prime D.K. and co-authors. "During the period of breastfeeding, simultaneous pumping of both breasts is more productive than sequential pumping." Brestfeed Med (Breastfeeding Medicine). 2012;7(6):442-447.
Breastfeed Med 2012; 7(6):442–447. - Prime D.K. and co-authors. "During the period of breastfeeding, simultaneous pumping of both breasts is more productive than sequential pumping." Brestfeed Med (Breastfeeding Medicine). 2012;7(6):442-447.
24 Uvn 9 K , Prime K. Oxytocin effects in mothers and infants during breastfeeding. Infant 2013; 9(6):201–206. - Uvenas-Moberg K, Prime DK, "Oxytocin effects on mother and child during breastfeeding". Infant. 2013;9(6):201-206.
25 Boundy EO et al. nine0315 Kangaroo mother care and neonatal outcomes: a meta-analysis. Pediatrics. 2015;137(1): e 20152238. - Boundi I.O. and co-authors, "The Kangaroo Method and Its Impact on Newborns: A Meta-Analysis". Pediatrix (Pediatrics). 2015;137(1): e20152238.
26 Acuña-Muga J et al. Volume of milk obtained in relation to location and circumstances of expression in mothers of very low birth weight infants. nine0315 J Hum Lact . 2014;30(1):41-46 - Akunya-Muga, J. et al., "The amount of milk expressed by location and circumstances of pumping in mothers of extremely low birth weight infants." G Hum Lakt. 2014;30(1):41-46
27 Nyqvist KH et al. Towards universal kangaroo mother care: recommendations and report from the first European conference and seventh international workshop on kangaroo mother care. nine0315 Acta Paediatr . 2010;99(6):820-826.- Nukvist K.H. et al., "On the Universality of the Kangaroo Method: Recommendations and Report from the First European Conference and the Seventh International Kangaroo Method Workshop". Akta Pediatr. 2010;99(6):820-826.
28 American Academy of Pediatrics - Section on Breastfeeding.