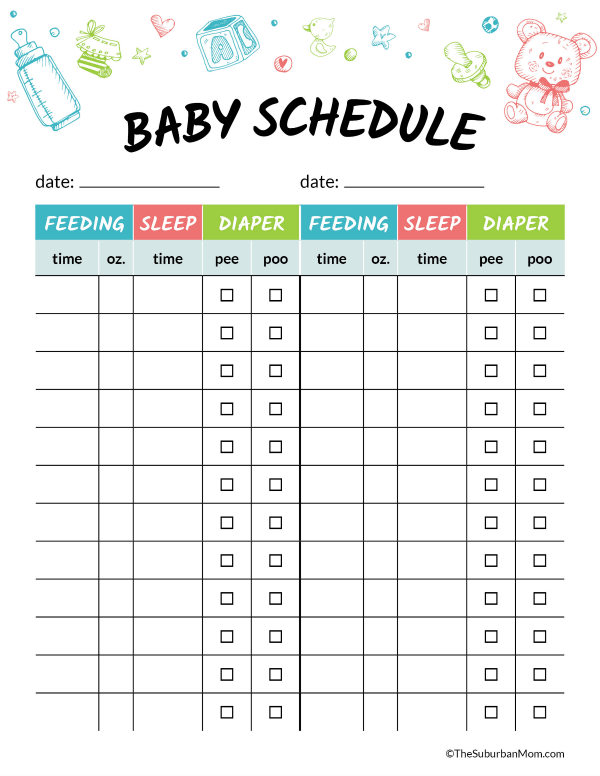
Putting baby on feeding schedule
Tips for the First Year
Eat, sleep, pee, poop, repeat. Those are the highlights in a day of the life of a brand new baby.
And if you’re a new parent, it’s the eating part that may be the source of many of your questions and worries. How many ounces should your baby take? Do you wake a sleeping baby to eat? Why do they seem hungry all the time? When can your child start solids?
Questions abound — and, despite Grandma’s insistence, the answers have changed since you were a tot. It’s now recommended that newborns, even formula-fed ones, eat on demand (consider it good preparation for the teenage years) and that babies wait to start solid foods until they’re 4 to 6 months old.
On day one of life, your baby’s stomach is the size of a marble and can only hold 1 to 1.4 teaspoons of liquid at a time. As your baby gets older, their stomach stretches and grows.
It’s hard (or impossible, really) to know how much milk your baby is taking in while breastfeeding. But if you’re bottle feeding due to any number of valid reasons, it’s a bit easier to measure.
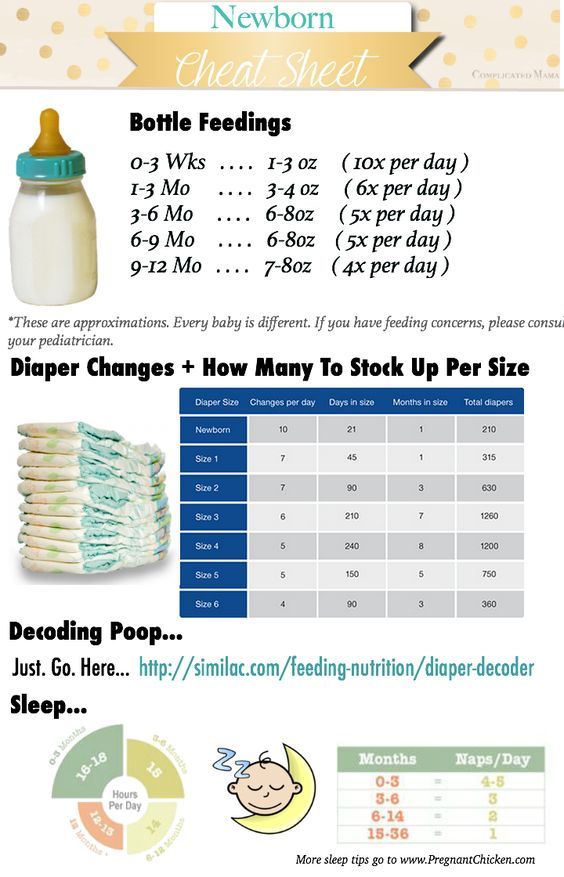
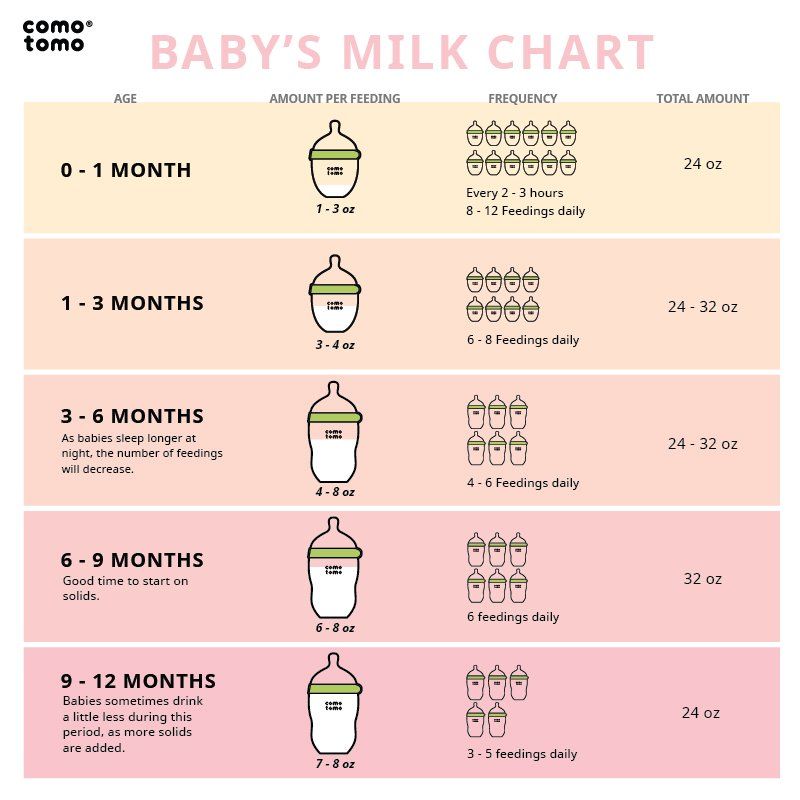
Here, from the American Academy of Pediatrics (AAP), a typical feeding schedule for bottle-fed babies.
| Age | Ounces per feeding | Solid foods |
|---|---|---|
| Up to 2 weeks of life | .5 oz. in the first days, then 1–3 oz. | No |
| 2 weeks to 2 months | 2–4 oz. | No |
| 2–4 months | 4-6 oz. | No |
| 4–6 months | 4–8 oz. | Possibly, if your baby can hold their head up and is at least 13 pounds. But you don’t need to introduce solid foods yet. |
| 6–12 months | 8 oz. | Yes. Start with soft foods, like one-grain cereals and pureed vegetables, meats, and fruits, progressing to mashed and well-chopped finger foods. Give your baby one new food at a time. Continue supplementing with breast or formula feedings.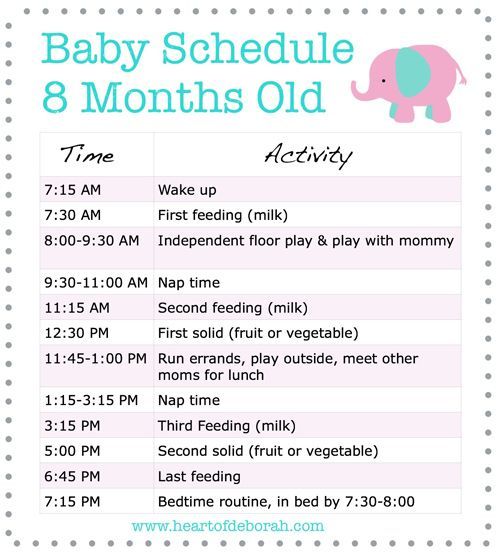 |
Every baby is unique — but one thing that’s pretty consistent is that breastfed babies eat more frequently than bottle-fed ones. That’s because breast milk is easily digested and empties from the stomach a lot quicker than formula.
Breastfed babies
There’s no rest for the weary. According to La Leche League International, you should begin nursing your baby within 1 hour of birth and provide about 8 to 12 feedings daily in the first few weeks of life (yeah, we’re exhausted for you).
At first, it’s important not to let your baby go more than 4 hours without feeding. You’ll likely need to wake them up if necessary, at least until breastfeeding is well established and they’re gaining weight appropriately.
As your baby grows and your milk supply amps up, your baby will be able to take in more milk in less time at one feeding. That’s when you might start to notice a more predictable pattern.
- 1 to 3 months: Your baby will feed 7 to 9 times per 24 hours.
- 3 months: Feedings take place 6 to 8 times in 24 hours.
- 6 months: Your baby will feed around 6 times a day.
- 12 months: Nursing may drop to about 4 times a day. The introduction of solids at about 6 months helps to fuel your baby’s additional nutritional needs.
Keep in mind that this pattern is just one example. Different babies have different paces and preferences, along with other factors that influence the frequency of feedings.
Bottle-fed babies
Like breastfed babies, bottle-fed newborns should eat on demand. On average, that’s about every 2 to 3 hours. A typical feeding schedule may look like this:
- Newborn: every 2 to 3 hours
- At 2 months: every 3 to 4 hours
- At 4 to 6 months: every 4 to 5 hours
- At 6+ months: every 4 to 5 hours
For both breastfed and bottle-fed babies
- Don’t give liquids other than formula or breast milk to babies under a year old. That includes juices and cow’s milk.
 They don’t provide the right (if any) nutrients and can be upsetting to your baby’s tummy. Water can be introduced around 6 months when you start offering a cup.
They don’t provide the right (if any) nutrients and can be upsetting to your baby’s tummy. Water can be introduced around 6 months when you start offering a cup. - Don’t add baby cereal to a bottle.
- It can create a choking hazard.
- A baby’s digestive system isn’t mature enough to handle cereal until about 4 to 6 months of age.
- You could overfeed your baby.
- Don’t give your baby any form of honey until after their first birthday. Honey can be dangerous for a baby, occasionally causing what’s called infant botulism.
- Do adjust your expectations based on your baby and their unique needs. Premature babies are likely to follow feeding patterns according to their adjusted age. If your baby has challenges like reflux or failure to thrive, you may need to work with your doctor on the appropriate feeding schedule and amount they should be eating.
Schedules are the holy grail of every parent. Your child will naturally start to fall into a feeding pattern as their tummy grows and they can take in more breast milk or formula at one sitting. This may begin to happen between 2 and 4 months of age.
This may begin to happen between 2 and 4 months of age.
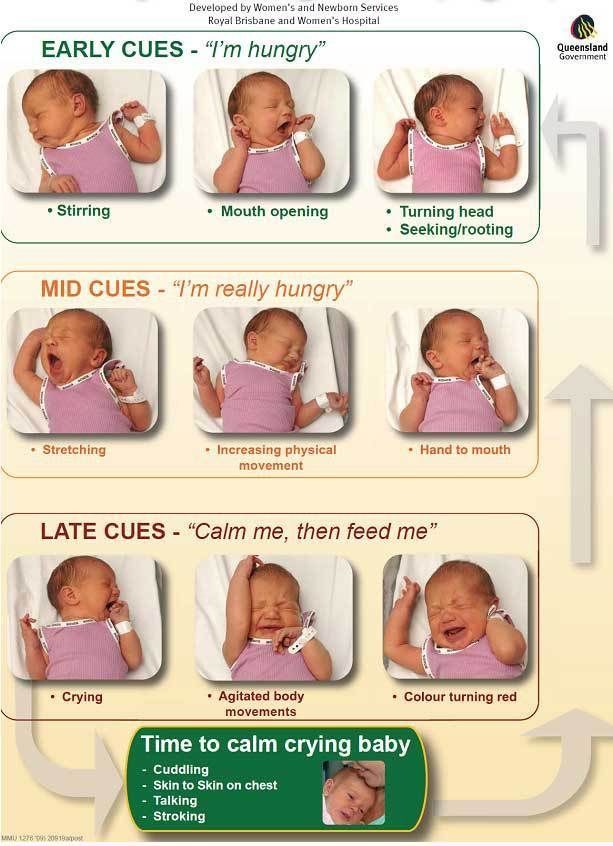
For now, though, focus on learning your baby’s hunger cues, such as:
- rooting around your chest, looking for a nipple.
- putting their fist in their mouth
- smacking or licking their lips
- fussing that can escalate quickly (don’t wait until your baby’s hangry to feed them)
Once your baby is a few months old, you may be able to introduce a sleep/feed schedule that works for you.
Let’s say, for example, your 4-month-old wakes every 5 hours for a feeding. That means if you feed at 9 p.m., your baby wakes around 2 a.m. But if you wake and feed the baby at 11 p.m., just before you go to bed, they may not rouse until 4 a.m., giving you a decent chunk of nighttime winks.
In general, if your baby seems hungry, feed them. Your baby will naturally eat more frequently during growth spurts, which typically occur around 3 weeks, 3 months, and 6 months of age.
Some babies will also “cluster feed,” meaning they’ll feed more frequently during certain periods and less at others.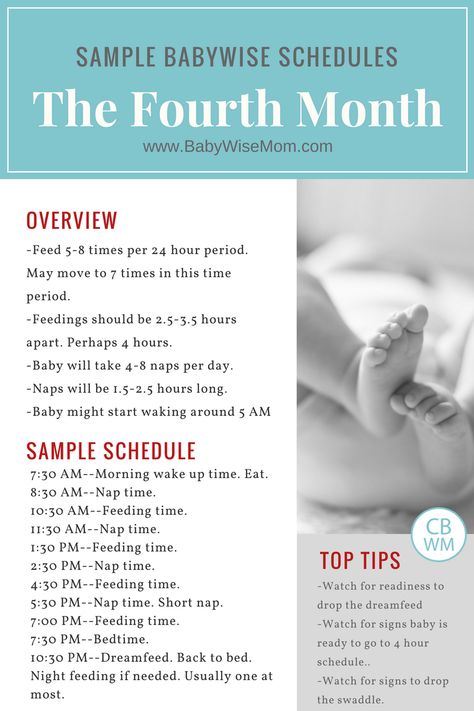 For example, your baby may cluster feed during the late afternoon and evening and then sleep longer at night (yay!). This is more common in breastfed babies than bottle fed babies.
For example, your baby may cluster feed during the late afternoon and evening and then sleep longer at night (yay!). This is more common in breastfed babies than bottle fed babies.
Worried about overfeeding? While this isn’t really possible to do with an exclusively breastfed baby, you can overfeed a baby who’s taking a bottle — especially if they’re sucking on the bottle for comfort. Follow their hunger cues, but talk to your pediatrician if you’re worried your little one may be overeating.
Your baby is probably ready for solids if they’re 4 to 6 months old and:
- have good head control
- seem interested in what you’re eating
- reach for food
- weigh 13 or more pounds
Which food to start with? The AAP now says it doesn’t really matter much in what order you introduce foods. The only real rule: Stick with one food for 3 to 5 days before offering another. If there’s an allergic reaction (rash, diarrhea, vomiting are common first signs), you’ll know which food is causing it.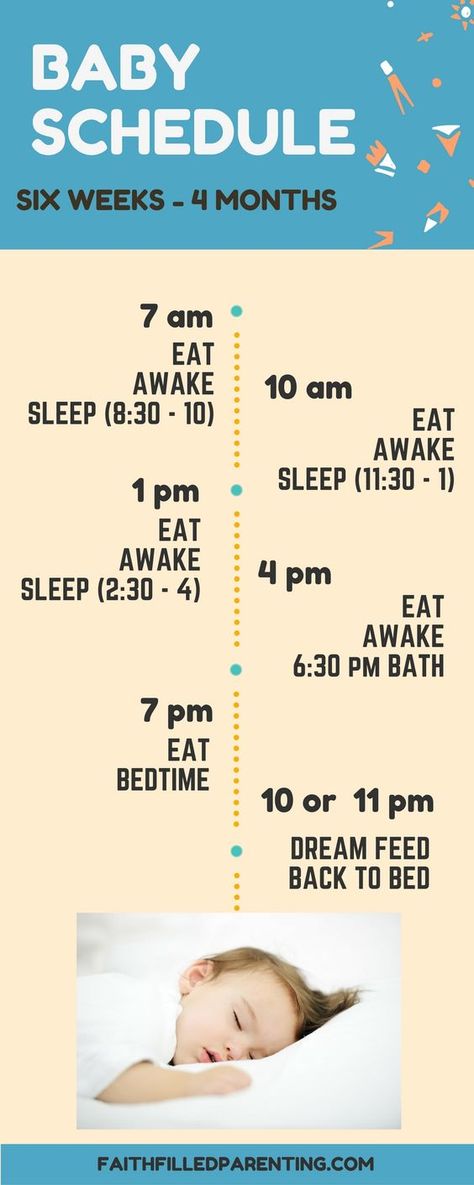
As your baby grows, move from pureed baby food to ones that have more texture (for example, mashed banana, scrambled egg, or well-cooked, chopped pasta). This generally happens around 8 to 10 months of age.
Your supermarket offers a variety of baby food products, but if you want to make your own, keep it sugar and salt free. Additionally, at this stage, don’t feed your baby anything that could be a choking hazard, including:
- hard foods, such as popcorn or nuts
- hard, fresh fruits, like apples; cook to soften or chop into very small pieces
- any meat that isn’t well cooked and very well chopped (this includes hot dogs)
- cheese cubes
- peanut butter (though talk to your pediatrician about this one — and the benefits of introducing diluted peanut butter before the age of 1)
As your baby nears their first birthday, they should be eating a variety of foods and taking in about 4 ounces of solids at each meal. Continue to offer breast milk or formula.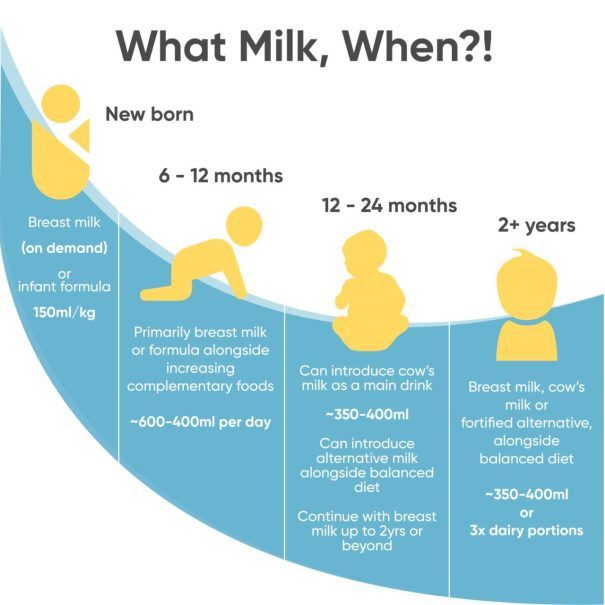 By 8 months, babies are drinking about 30 ounces a day.
By 8 months, babies are drinking about 30 ounces a day.
Oh yeah, and buy some stock in a company that makes stain-fighting laundry detergent. It’ll pay for college.
Babies aren’t cookie cutter. Some will gain weight easily, while others will have problems. Things that can affect a baby’s weight gain include:
- having a birth defect like a cleft lip or palate, which creates problems feeding
- having a milk protein intolerance
- being premature
- being fed with a bottle versus the breast
A 2012 study of more than 1,800 babies found that the infants who were fed with a bottle — regardless of whether the bottle contained breast milk or formula — gained more weight in the first year than babies who nursed exclusively.
Your baby’s doctor is the best one to advise you on a healthy weight range for your baby.
How, when, and what to feed a baby are top worries of every parent — but there’s good news: Most babies are pretty good judges of when they’re hungry and when they’re full — and they’ll let you know it.
You just need to present them with the right choices at the right time and pay attention to their cues. If you have any questions or concerns, your pediatrician is there to help you along the way.
Why feeding "on cue" benefits babies
© 2009 – 2021 Gwen Dewar, Ph.D., all rights reserved
The infant feeding schedule reconsidered
In the past, Western “baby experts” often instructed parents to feed their babies at regularly-spaced intervals of 3- or 4-hours. Today, official medical recommendations have shifted in favor of letting babies decide. Why the change?
There are a number of reasons, but the simple answer is this: When we let babies determine the timing and the length of their own feeds, they are more likely to get what they need: Not too little, and not too much.
It begins in the newborn period. If newborn babies aren’t fed frequently enough, they are at higher risk for dehydration and underfeeding. So the American Academy of Pediatrics (AAP) advises parents to feed infants at least once every 2-3 hours — whenever babies show signs of hunger (AAP 2015).
During the subsequent months, babies may be able to go longer between meals. But feeding responsively — on cue — remains the ideal approach.
- It can help breastfed babies adjust to natural variations in milk quality (Institute of Medicine, National Academy of Sciences 1991).
- It can help bottle-bed babies avoid overfeeding.
- And it can help any infant cope with the challenges of getting enough to eat during a growth spurt.
All babies experience fluctuations in their energy requirements. Feeding on cue makes it easier for infants to increase or decrease their intake as needed (Tylka et al 2015).
That’s probably why responsive feeding is associated with healthier growth trajectories in babies (Chen et al 2020; Fuglestad et al 2017).
And that’s not all. Research hints that responsive feeding benefits babies in additional ways. It might affect an infant’s emotional functioning. It might support better cognitive outcomes.
So it seems that the best infant feeding schedule is the one that babies devise for themselves.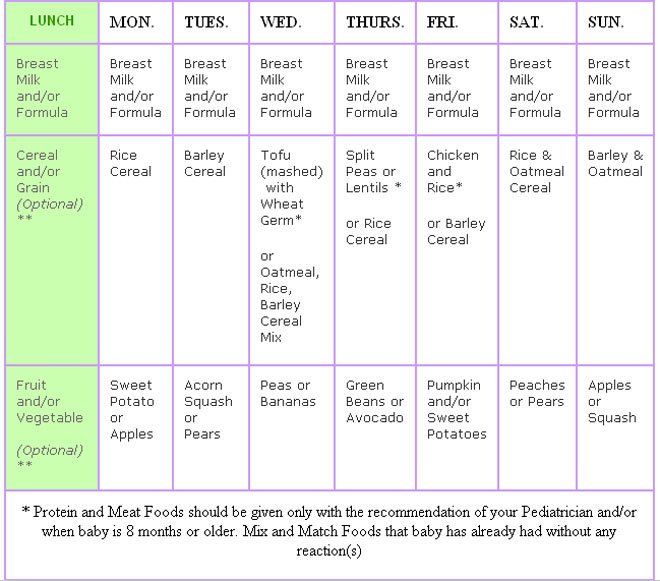
But what is the evidence? Let’s take more detailed look.
The infant feeding schedule in evolutionary perspective
Mammal babies everywhere begin life on a diet of milk. But they don’t all time their feedings in the same way. In some species, mothers “park” or “cache” their young in nests, and leave them there.
It’s a strategy that allows the mother to go foraging without the fuss of a tag-along infant. But it only works if there’s a way to keep the babies from starving during those long separations. How do they cope?
The solution is two-fold.
1. Mothers produce milk that is high in fat, and high in protein — what we might call super-fuel.
2. Infants have the ability to suckle very fast and efficiently when they finally get to feed.
Together, these elements permit babies to “tank up” on a highly-concentrated food–enough to last them for many hours.
Mammals that follow this strategy are called “spaced feeders,” and their milk is very rich indeed.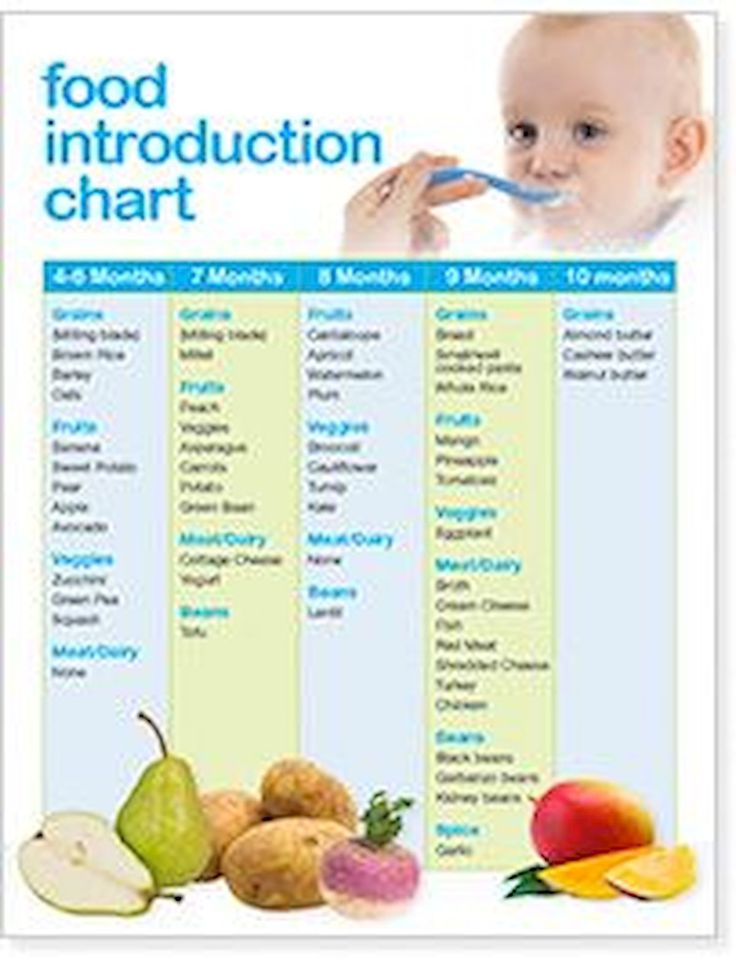
A good example of a spaced feeder is the rabbit, which produces milk that is 18.3% fat and 13.9% protein (Jenness 1974).
By contrast, other mammals keep their babies with them as they forage. Exactly how they do this varies from species to species. Some, like monkeys, carry their babies. Others, like cows, have their infants follow them around on foot.
But regardless, the babies stay close, and along with proximity comes frequent meals. Babies tend to initiate feedings, and suckle at a more leisurely rate. They don’t need to tank up on a super-fuel, and so their mothers don’t make one. The milk is less caloric, more dilute.
A good example of a continual feeder is a cow, which produces milk that is typically 3.7% fat and 3.4% protein (Jenness 1974).
What about humans?
In some modern, industrial societies, humans act like spaced feeders. Babies are “parked” in cribs or cradles and get fed after intervals of 3-4 hours.
But were we designed for this strategy?
Does the biology of human breastfeeding have the earmarks of spaced feeding?
The answer is no because
- human milk is relatively low in fat (3.
 8%) and protein (1%), and
8%) and protein (1%), and - human infants suckle at the slow pace typical of continual feeders.
So our basic physiology gives us away. We don’t produce super-fuel, and our infants lack the spaced-feeder’s knack for super-fast milk extraction. And that’s consistent with the behavior of other members of our family tree. Continual feeding is the strategy of choice among all of our close relatives — including bonobos, chimpanzees, and gorillas.
It is also the strategy observed among human beings living in traditional societies.
In hunter-gatherer societies, babies aren’t just nursed on cue. They are also nursed very frequently — about 2-4 times an hour (Konner 2006).
In other traditional societies, parents don’t match this extreme pace, but feedings are nonetheless initiated by the infants.
In a survey of non-industrial societies (which included nomadic pastoralists and settled agricultural peoples) anthropologists found that “on demand” feeding was the rule. In every society for which information about the infant feeding schedule was available (25 out of 25), people fed their infants on cue (Severn Nelson et al 2000).
In every society for which information about the infant feeding schedule was available (25 out of 25), people fed their infants on cue (Severn Nelson et al 2000).
This, then, is our basic physiology and our evolutionary heritage. But how much does it matter? Is this something we can work around?
Mightn’t we be able to keep babies equally happy and healthy using a strict infant feeding schedule? Perhaps it’s just a matter of tweaking the timing of feeds.
It sounds straightforward, but there are stumbling blocks.
Babies vary in their needs — from individual to individual, and from day to day
Different babies have different needs, and the same baby experiences fluctuations in energy requirements over time.
What if your baby has the urge to be more active, and needs more food to fuel her activities?
What if your infant needs more fluids because it’s hot, or because he’s coming down with a virus?
What if your baby is in the middle of a growth spurt?
It isn’t merely that you need to adopt a schedule that is individualized to your baby’s current needs. You also need a schedule that keeps changing in response his or her future needs.
You also need a schedule that keeps changing in response his or her future needs.
That’s pretty hard to do unless you are paying attention to your baby, offering meals when you observe signs of hunger. And if you are doing that, you aren’t imposing a strictly-timed infant feeding schedule. By definition, you are feeding on cue.
Moreover, the baby’s need for food and fluids is only one side of the equation — the demand side. There is also the supply side of the equation. If your baby is on formula, it’s easy to figure out what your baby is being supplied with. You can read the label, and know your baby is getting the same formulation from one feed to the next.
But breast milk doesn’t work that way. Human breast milk is roughly similar in composition from one woman to the next, but there are significant differences. Not only does breast milk vary between individuals. It also varies between milk samples produced by the same woman at different points in time.
Breast milk varies in caloric content
When Shelly Hester and her colleagues analyzed 22 published studies on the metabolizable energy content of breast milk, the researchers were able to estimate the calories found per serving: About 65 calories per 100 milliliters (mL) of breast milk.
But hang on. That estimate is the average for milk expressed between 2 weeks and 6 weeks postpartum (Hester et al 2012).
Milk produced earlier is substantially less caloric. Colostrum, the milk produced during the first few days, has only about 53 calories per 100 mL. Then, between approximately 6 and 14 days postpartum, the caloric density increases slightly, averaging 58 calories per 100 mL (Hester et al 2012).
And milk produced later — after the 6 weeks postpartum — becomes increasingly caloric as time goes by. That’s because the fat content of breast milk tends to increase the longer a woman continues to nurse.
When researchers have tracked lactating mothers over time, they’ve found that the fat content in milk produced at 6 months is higher than it is at 3 months (Szabó et al 2010).
That’s a lot of variation already, but we’ve only scratched the surface because individual mothers vary substantially in the energy content of their milk. Studies indicate that individual woman may range widely in the fat content of their milk — from 2 grams per 100mL to 5 grams per mL (Institute of Medicine, National Academy of Sciences 1991).
And other research has identified some of the causes of this variation: Diet, body mass index, maternal age, socioeconomic status, and even smoking habits have been linked with differences in the amount of fat in breast milk (Daniel et al 2021; Innis 2014; Rocquelin et al 1998; Argov-Argaman et al 2017; Al-Tamer et al 2006; Agostoni et al 2003).
So it shouldn’t surprise us if there is no “one size fits all” infant feeding schedule that’s going to serve every baby equally well. Babies vary in their needs, and different breastfed babies may be receiving very different types of breast milk. Some get milk that is richer than average. Others get milk that is much lighter.
Others get milk that is much lighter.
And since babies can only drink so much before their stomachs are full, the fat content of milk is going to make a substantial difference in the calories they obtain from any given feeding session. Some babies will need more frequent feedings than other babies do, simply because their milk has fewer calories per serving.
Just as important, milk from the same mother can fluctuate in quality from day to day, and even from hour to hour (Khan et al 2013). So it’s possible that an infant feeding schedule that works pretty well one day might leave a baby dissatisfied on another.
Finally, it’s worth noting that the quality of breast milk changes during the course of a feed.
At the beginning of a feeding session, when the breast appears full, the milk that is released is relatively diluted and low in fat. Then, as the session continues, the breast takes on a softer, emptier appearance, and the milk changes.
The earlier “foremilk” gives way to a more concentrated, fattier “hindmilk” (Woolridge 1995), and you can see the difference in this photo.
The foremilk looks watery and bluish. The hindmilk — produced by the same breast, but later in the session — is ivory in color, and thicker.
Thus, if the adult terminates the breastfeeding session too soon, or forces a baby to switch breasts too soon, the baby will miss out on hindmilk (Woolridge and Fisher 1988).
Babies in this situation will fill up on a low calorie meal, and require more frequent feedings to obtain the energy they need.
In addition, they may be at higher risk for symptoms associated with consuming low quality milk. As breastfeeding expert Michael Woolridge (MD and PhD) has pointed out, low-fat milk can contribute to colic, vomiting, diarrhea, and flatulence in infants (Woolridge 1995).
What about formula-fed babies? Don’t they need us to impose restrictions — so they won’t overfeed?
You may have heard about research linking formula-feeding with rapid infant growth and an increased risk of childhood obesity. The links have been replicated in many studies, have prompted concern. Why are formula-fed babies more likely to become overweight?
The links have been replicated in many studies, have prompted concern. Why are formula-fed babies more likely to become overweight?
One answer is that formula might be too energy-dense for some babies (Hester et al 2012). But it also appears that the delivery system — drinking from a bottle — is a contributing factor.
For example, in one study of 1250 American infants, researchers found that bottle-feeding in early infancy was associated with a tendency to eat everything on offer, regardless of whether the babies consumed formula or breast milk.
The more frequently babies drank from bottles during their first 6 months, the more likely they were to become big eaters later. As toddlers, they were more likely to completely drain any bottle or cup given to them (Li et al 2010).
A smaller study conducted in the United Kingdom reports similar results (Brown and Lee 2012).
It’s not clear what this means, but we know that infants can extract milk more quickly from a bottle than they can from a breast.
Perhaps the fast pace leads to consuming more during a feed, so babies become accustomed to taking in bigger meals.
Whatever the underlying cause, it invites the obvious question: Isn’t this a good reason to impose an infant feeding schedule? Aren’t bottle-fed babies better off if we restrict the timing of their meals?
The evidence suggests not.
For instance, experimental research indicates that babies are sensitive to internal cues of hunger and satiety. When allowed to feed on demand, both breastfed (Woolridge and Baum 1992) and formula-fed (Fomon et al 1975) infants adjust their intakes in response to the caloric content of their milk or formula.
And when researchers have tracked infant development over time, they haven’t found that feeding restrictions — including timed feeding schedules — reduce the risk of a child becoming overweight. On the contrary.
In one study, researchers found that scheduled feeding was a risk factor for rapid weight gain (Mihrshahi et al 2011). And — overall — research suggests that restrictive feeding is more likely than responsive feeding to lead to high weight gain (Gubbels et al 2011; DiSantis et al 2011b; Dinkevich et al 2015; Gross et 2014; Spill et al 2019).
And — overall — research suggests that restrictive feeding is more likely than responsive feeding to lead to high weight gain (Gubbels et al 2011; DiSantis et al 2011b; Dinkevich et al 2015; Gross et 2014; Spill et al 2019).
Surprising? Perhaps it shouldn’t be. These observations are consistent with studies of older children.
It appears that intrusive, restrictive rules about eating may interfere with the development of self-regulation. They may actually increase a child’s tendency to engage in emotional overeating (Jani et al 2015; Rodgers et al 2013), and lead to excessive weight gain (Tylka et al 2015).
So researchers suspect that imposing restrictions — like a strict infant feeding schedule — are counterproductive for preventing obesity.
Kids might learn to ignore their own hunger cues, and eat in response to social cues (“it’s time!”) or emotions (“I’ve been denied — now it’s time to make up for that”). By allowing infants to initiate feedings, we may be helping them develop a more healthy relationship with food.
Other considerations: Do the effects of an infant schedule extend beyond matters of nutrition and energy regulation?
That’s an interesting question.
From birth, infants get distressed when their signals to nurse are ignored. And studies indicate brief, token acts of feeding can help newborns bounce back from stress.
Newborns cry less and show signs of reduced pain when they receive small amounts of milk, formula, or sucrose (see review by Shaw et al 2007; also Blass 1997a; Blass 1997b; Blass and Watt 1999; Barr et al 1999). The act of suckling is itself an analgesic (Blass and Watt 1999). And breastfeeding may be a painkiller and stress-reducer.
In one study, newborns subjected to a painful blood collection procedure cried much less if they were permitted to breastfeed (Gray et al 2002). They cried just 4% of time total procedure time, versus 43% for infants in a control group.
Babies who fed during the procedure also showed markedly reduced rates of grimacing (8% v. 50%), and their heart rates increased less (6 beats per minute v. 29 beats per minute).
50%), and their heart rates increased less (6 beats per minute v. 29 beats per minute).
Some of these differences may be attributable to the extra skin-to-skin contact that the breastfed babies got. But in a follow-up study, the researchers confirmed that breastfeeding was more soothing than skin-to-skin contact alone (Gray et al 2000; Gray et al 2002). And the authors noted that babies who were held without being fed tended to get frustrated, and required much more time to settle down (Gray et al 2002).
So what might happen to a baby who finds that her signals for quick comfort are routinely ignored?
While I’ve found no studies that bear directly on this question, responsive care has been linked with development of better stress regulation skills — even among highly irritable, “at risk” babies.
Moreover, a variety of studies suggest that sensitive, responsive parenting contributes to secure attachment relationships and better child outcomes.
And there is intriguing research regarding cognitive development.
In what is perhaps the largest study yet to investigate the effects of an infant feeding schedule, Maria Iacovou and Almudena Sevilla (2013) tracked the development of more than 10,000 British children — breastfed and bottle-fed alike — from birth to age 14.
There were no experimental manipulations. The researchers merely noted whether babies had been fed on schedule or “on demand”, and then followed their cognitive and academic progress. And the results? They favored feeding “on demand”.
At every age, kids who’d been subjected to an infant feeding schedule performed more poorly on standardized tests. Moreover, their IQs were, on average, 4.5 points lower.
Correlation doesn’t prove causation, of course, and this is just one study. It needs to be replicated.
But it’s interesting to note that the study’s results remained much the same even after researchers controlled for a variety of potential confounds, like parents’ education levels, economic factors, health, breastfeeding, maternal smoking, and the children’s exposure to negative discipline tactics.
There wasn’t any obvious reason for the difference between groups. Just the distinction between feeding on cue and following an infant feeding schedule.
Summing up: What do we really know?
As with most science, we still have a lot left to learn.
We don’t yet understand all the determinants of breast milk quality, or why the composition of breast milk changes over time.
We don’t yet understand all the causes of increased obesity risk in formula-fed and bottle-fed infants.
And it isn’t yet clear how much impact an infant feeding schedule might have over the long-term. In particular, we need more research on the possible effects an infant feeding schedule might have on stress regulation and cognitive development.
Meanwhile, what we do know is that human beings exhibit the characteristics of continual feeders, and it’s a sure bet that relatively frequent, “on demand” feedings have been the historic and evolutionary norm for our species.
It’s also clear that breast milk can vary substantially in fat composition and caloric density, so that babies will benefit from being able to schedule the timing of their own feeds.
And all babies — whether they consume breast milk or formula — experience fluctuations in their needs for fluids and energy. When we are responsive to their cues of hunger and thirst, we’re more likely to meet these needs.
More reading
How can you tell if a newborn is hungry? Find answers to this and other questions in my article, “The newborn infant feeding schedule: A review of the evidence against regimented feedings.”
In addition, you can read more about this topic in “Breastfeeding on demand: A cross-cultural perspective.” And for more information about the composition of breast milk, read this Parenting Science article.
Wondering if you can time your baby’s meals to optimize sleep at night? Check out my article, “Dream feeding: An evidence-based guide to helping babies sleep longer.”
What about solid foods? When and how should you introduce your baby to solids? This Parenting Science article will guide you through the process, and answer interesting questions about infant behavior, adding spices to foods, and more.
And are some other Parenting Science articles that might interest you:
- Baby sleep patterns for the science-minded
- The newborn senses: What can babies feel, see, hear, smell, and taste
- Stress in babies: How to keep babies calm, happy, and healthy
- Motor milestones: How do babies develop during the first two years?
References: The best infant feeding schedule
Agostoni C, Marangoni F, Grandi F, Lammardo AM, Giovannini M, Riva E, Galli C. 2003. Earlier smoking habits are associated with higher serum lipids and lower milk fat and polyunsaturated fatty acid content in the first 6 months of lactation. Eur J Clin Nutr. 57(11):1466-72.
Al-Tamer YY and Mahmood AA.2006. The influence of Iraqi mothers’ socioeconomic status on their milk-lipid content. Eur J Clin Nutr. 60(12):1400-5.
American Academy of Pediatrics. 2015. Caring for your baby and young child: Birth to age 5. 7th Edition. T. Altmann (ed). Bantam.
Argov-Argaman N, Mandel D, Lubetzky R, Hausman Kedem M, Cohen BC, Berkovitz Z, Reifen R. 2017. Human milk fatty acids composition is affected by maternal age. J Matern Fetal Neonatal Med 30(1):34-37.
2017. Human milk fatty acids composition is affected by maternal age. J Matern Fetal Neonatal Med 30(1):34-37.
Barr RG, Pantel MS, Young SN, Wright JH, Hendricks LA, Gravel R. 1999. The response of crying newborns to sucrose: is it a “sweetness” effect? Physiol. Behav 66: 409-417.
Bergmeier HJ, Skouteris H, Haycraft E, Haines J, Hooley M. 2015. Reported and observed controlling feeding practices predict child eating behavior after 12 months. J Nutr. 145(6):1311-6.
Blass EM. 1997a Milk-induced hypoanalgesia in human newborns. Pediatrics 99: 825-829.
Blass EM. 1997b. Infant formula quiets crying newborns. Journal of Dev Behavioral Pediatrics. 18:162-165.
Brown A and Lee M. 2012. Breastfeeding during the first year promotes satiety responsiveness in children aged 18-24 months. Pediatr Obes. 7(5):382-90.
Chen TL, Chen YY, Lin CL, Peng FS, Chien LY. 2020. Responsive Feeding, Infant Growth, and Postpartum Depressive Symptoms During 3 Months Postpartum. Nutrients. 12(6):1766.
12(6):1766.
Daly SE, DiRosso A, Owens RA and Hartmann PE. 1993. Degree of breast emptying explains fat content, but not fatty acid composition, of human milk. Exp Physiol 78: 741-755.
Daniel AI, Shama S, Ismail S, Bourdon C, Kiss A, Mwangome M, Bandsma RHJ, O’Connor DL. 2021. Maternal BMI is positively associated with human milk fat: a systematic review and meta-regression analysis. Am J Clin Nutr. 113(4):1009-1022.
Dinkevich E, Leid L, Pryor K, Wei Y, Huberman H, Carnell S. 2015. Mothers’ feeding behaviors in infancy: Do they predict child weight trajectories? Obesity (Silver Spring). 23(12):2470-6.
Disantis KI, Collins BN, Fisher JO, and Davey A. 2011a. Do infants fed directly from the breast have improved appetite regulation and slower growth during early childhood compared with infants fed from a bottle? Int J Behav Nutr Phys Act. 8:89.
Disantis KI, Hodges EA, Johnson SL, and Fisher JO. 2011b. The role of responsive feeding in overweight during infancy and toddlerhood: a systematic review. International Journal of Obesity 35: 480–492
International Journal of Obesity 35: 480–492
Fomon SJ, Filmer, Jr., JA, Thomas LN, Anderson TA and Nelson SE. 1975. Influence of formula concentration on caloric intake and growth of normal infants. Acta Pediatrica Scandinavica 64: 172-181.
Fuglestad AJ, Demerath EW, Finsaas MC, Moore CJ, Georgieff MK, Carlson SM. 2017. Maternal executive function, infant feeding responsiveness and infant growth during the first 3 months. Pediatr Obes. 12 Suppl 1:102-110.
Gubbels JS, Thijs C, Stafleu A, van Buuren S, Kremers SP. 2011. Association of breast-feeding and feeding on demand with child weight status up to 4 years. Int J Pediatr Obes. 6(2-2):e515-22.
Gray L, Miller LW, Philipp BL, Blass EM. 2002. Breastfeeding is analgesic in healthy newborns. Pediatrics 109: 590-593.
Gray L, Watt L, Blass EM. Skin-to-skin contact is analgesic in healthy newborns. Pediatrics 105(1).
Gross RS, Mendelsohn AL, Fierman AH, Hauser NR, Messito MJ. 2014. Maternal infant feeding behaviors and disparities in early child obesity. Child Obes. 10(2):145-52.
Child Obes. 10(2):145-52.
Hausman Kedem M, Mandel D, Domani KA, Mimouni FB, Shay V, Marom R, Dollberg S, Herman L, Lubetzky R. 2013. The effect of advanced maternal age upon human milk fat content. Breastfeed Med. 8(1):116-9.
Hester SN, Hustead DS, Mackey AD, Singhal A, and Marriage BJ. 2012. Is the macronutrient intake of formula-fed infants greater than breast-fed infants in early infancy? Journal of Nutrition and Metabolism: 891201.
Iacovou M and Sevilla A. 2013. Infant feeding: the effects of scheduled vs. on-demand feeding on mothers’ wellbeing and children’s cognitive development. Eur J Public Health. 23(1):13-9.
Illingworth RS, Stone DHG, Jowett JH and Scott JF. 1952. Self-demand feeding in a maternity unit. Lancet 1: 683-687.
Innis SM. 2014. Impact of maternal diet on human milk composition and neurological development of infants. Am J Clin Nutr. 99(3):734S-41S.
Institute of Medicine, National Academy of Sciences. 1991. Nutrition during lactation.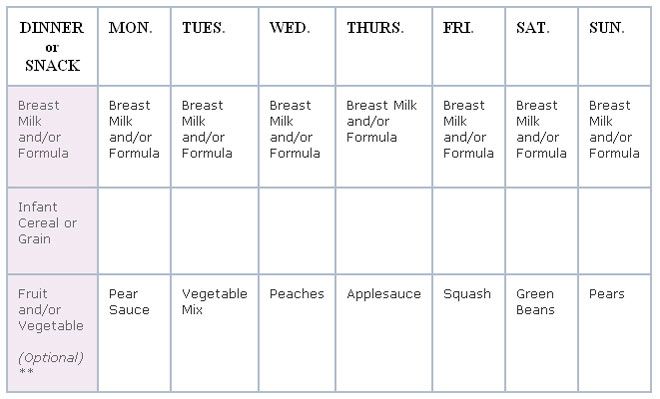 Washington, DC: National Academy Press.
Washington, DC: National Academy Press.
Jackson DA, Imong SM, Silpraset A, Preunglumpoo Ruckphaopunt S, Williams AF, Woolridge MW, Baum JD, and Amatayakul K. 1988. Circadian variation in fat concentration of breastmilk in rural Northern Thailand. British Journal of Nutrition 59: 365-371.
Jani R, Mallan KM, Daniels L.2015. Association between Australian-Indian mothers’ controlling feeding practices and children’s appetite traits. Appetite 84:188-95
Jenness 1974. Biosynthesis and composition of milk. Journal of investigative dermatology. 63: 109-118.
Kersting M and Dulon M. 2001. Assessment of breastfeeding promotion in hospitals and follow up survey of mother-infant pairs in Germany: The Su-Se study. Public Health Nutrition 5(4): 547-552.
Khan S, Hepworth AR, Prime DK, Lai CT, Trengove NJ, Hartmann PE. 2013. Variation in fat, lactose, and protein composition in breast milk over 24 hours: associations with infant feeding patterns. J Hum Lact. 29(1):81-9
Konner M. 2005. Hunter-gatherer infancy and childhood: The !Kung and others. In: Hunter-gatherer childhoods: Evolutionary, developmental and cultural perpectives. BS Hewlett and ME Lamb (eds). New Brunswick: Transaction Publishers.
2005. Hunter-gatherer infancy and childhood: The !Kung and others. In: Hunter-gatherer childhoods: Evolutionary, developmental and cultural perpectives. BS Hewlett and ME Lamb (eds). New Brunswick: Transaction Publishers.
Li R, Fein SB, Grummer-Strawn LM. 2010. Do infants fed from bottles lack self-regulation of milk intake compared with directly breastfed infants? Pediatrics. 125(6):e1386-93.
Mandel D, Lubetzky R, Dollberg S, Barak S, Mimouni FB. 2005. Fat and energy contents of expressed human breast milk in prolonged lactation. Pediatrics. 116(3):e432-5.
Mihrshahi S, Battistutta D, Magarey A, Daniels LA. 2011. Determinants of rapid weight gain during infancy: baseline results from the NOURISH randomised controlled trial. BMC Pediatr. 11:99.
Prentice AM and Prentice A. 1988. Energy costs of lactation. Annual review of nutrition 8: 63-79.
Prentice A, Prentice AM and Whitehead RG. 1981. Breast-milk concentrations of rural African women I. Short-term variations within individuals.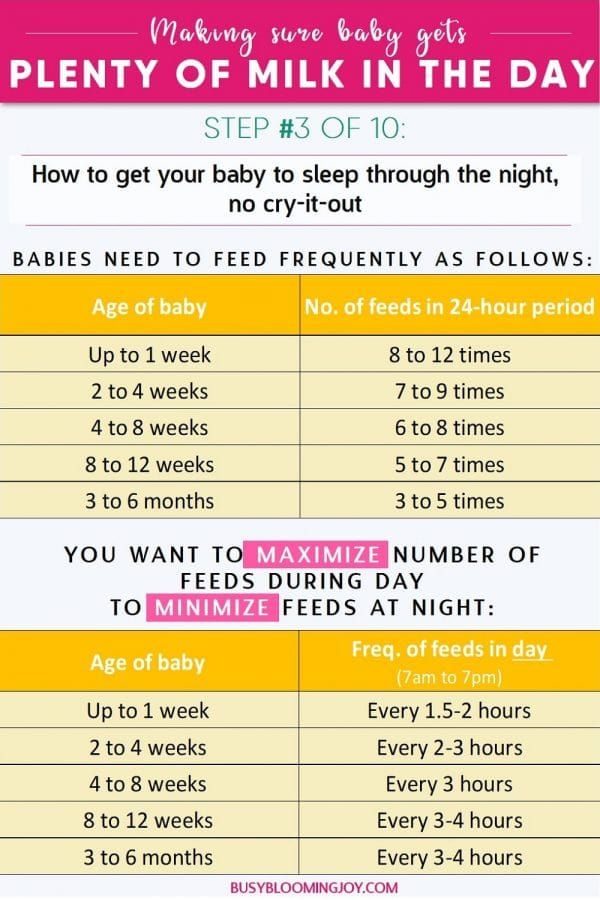 British Journal of Nutrition 45: 483-494.
British Journal of Nutrition 45: 483-494.
Rocquelin G, Tapsoba S, Dop MC, Mbemba F, Traissac P, Martin-Prével Y. 1998. Lipid content and essential fatty acid (EFA) composition of mature Congolese breast milk are influenced by mothers’ nutritional status: impact on infants’ EFA supply. Eur J Clin Nutr. 52(3):164-71
Rodgers RF, Paxton SJ, Massey R, Campbell KJ, Wertheim EH, Skouteris H, Gibbons K. 2013. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: a prospective study. Int J Behav Nutr Phys Act. 10:24
Saxon TF, Gollapalli A, Mitchell MW, and Stanko S. 2002. Demand feeding or schedule feeding: infant growth from birth to 6 months. Journal of reproductive and infant psychology 20(2): 89-99.
Severn Nelson EA, Schiefenhoevel W, and Haimerl F. 2000. Child care practices in nonindustrial societies. Pediatrics 105: 75-79.
Shah PS, Aliwalas L, and Shah V. 2007. Breastfeeding or breast milk to alleviate procedural pain in neonates: a systematic review. Breastfeeding medicine 2:74-82.
Breastfeeding medicine 2:74-82.
Spill MK, Callahan EH, Shapiro MJ, Spahn JM, Wong YP, Benjamin-Neelon SE, Birch L, Black MM, Cook JT, Faith MS, Mennella JA, Casavale KO. 2019. Caregiver feeding practices and child weight outcomes: a systematic review. Am J Clin Nutr. 109(Suppl_7):990S-1002S.
Szabó E, Boehm G, Beermann C, Weyermann M, Brenner H, Rothenbacher D, Decsi T. 2010. Fatty acid profile comparisons in human milk sampled from the same mothers at the sixth week and the sixth month of lactation. J Pediatr Gastroenterol Nutr. 50(3):316-20.
Tilden CD and Oftedal OT. 1997. Milk composition reflects pattern of maternal care in prosimian primates. American Journal of Primatology 41: 195-211.
Tylka TL, Lumeng JC, Eneli IU. 2015. Maternal intuitive eating as a moderator of the association between concern about child weight and restrictive child feeding. Appetite 95:158-65.
Ventura AK, Inamdar LB, Mennella JA. 2015. Consistency in infants’ behavioural signalling of satiation during bottle-feeding. Pediatr Obes. 10(3):180-7.
Pediatr Obes. 10(3):180-7.
Wojcik KY, Rechtman DJ, Lee ML, Montoya A, Medo ET. 2009. Macronutrient analysis of a nationwide sample of donor breast milk. J Am Diet Assoc. 109(1):137-40.
Woolridge MW. 1995. Baby-controlled breastfeeding: Biocultural implications. In: Breastfeeding: Biocultural perspectives. P. Stuart-Macadam and KA Dettwyler (eds). New York: Aldine deGruyter.
Woolridge MW and Baum JD. 1992. Infant appetite-control and the regulation of breast milk supply. Children’s hospital quarterly 3:133-119.
Woolridge MW and Fisher C. 1988. Colic, ‘Overfeeding,’ and Symptoms of Lactose Malabsorption in the Breast-Fed Baby: A Possible Artifact of Feed Management. Lancet 13: 382-384.
Note: Portions of this article, “Jettisoning the infant feeding schedule: Why babies are better off feeding on cue,” are taken from an earlier Parenting Science article, “The infant feeding schedule: Why babies benefit from feeding on demand.” The material here has been updated and substantially revised.
For more references pertaining to the infant feeding schedule, see my article on breastfeeding on demand.
Image credits for “The best infant feeding schedule”
image of infant breastfeeding by istock / Jomkwan
Content of “The best infant feeding schedule” last modified 5/2021
Mixed infant feeding: how to start and introduce | Scheme and diet, menu for mixed feeding
Co-author, editor and medical expert - Klimovich Elina Valerievna.
Number of views: 71 278
Date last updated: 11/24/2022
Average read time: 4 minutes
, which means switching to mixed feeding. It is recommended to make a decision on the transfer of a newborn to mixed feeding together with a pediatrician who will help you choose the right mixture.
Contents:
When do mothers switch to mixed feeding?
How to organize mixed feeding?
When do mothers switch to mixed feeding?
1. Lack of own milk
Lack of own milk
In some cases, even if the mother puts the baby to the breast on demand, the child may still remain hungry and gain weight poorly. This is often evidenced by loud crying after eating. In this case, experts speak of hypolactia, when milk production is reduced due to a hormonal disorder.
The “wet diaper” method will help to make sure that the baby really does not have enough milk. Do not put "diapers" on your baby and count the number of his urination in one day. From two weeks of age to six months, the result is evaluated as follows: if you counted 12 or more wet diapers, then you have nothing to worry about, 8–10 wet diapers indicate that lactation has decreased, 6 or less - the child does not have enough milk, and urgent action should be taken.
Tip! Today there are many ways to increase lactation, but if they do not help, you should consult a pediatrician who will choose the right formula for supplementary feeding.
2. Lack of calories
Some mothers think that their milk is not nutritious enough. Most often, they come to such conclusions by expressing clear milk with a bluish tint. But it cannot be nonnutritive or nutritious. Milk is “rear”, saturated white, thicker and fatter (for a child, this is “food”), and “front”, liquid with a bluish tint (“drink”).
Tip! If the amount of urination is normal, but the baby is not gaining weight, then you need to think about whether your baby is getting "hind" milk. To do this, offer him only 1 breast during 1 feeding.
3. Coming to work
Some mothers have to reduce the number of feedings after going to work. And their first impulse is to switch to mixed feeding. But you should always remember that the best food for a child is mother's milk. If you want to go to work, try to prepare for this in advance. Make a "strategic stock" of breast milk in the freezer so your baby always has food, even when you're not around.
Tip! If you plan to go to work when your baby has started to receive complementary foods, then try to organize meals so that complementary foods are given to him in your absence. So you will have the opportunity to reduce the amount of formula or defrosted in his diet
Up to the content
How to organize mixed feeding?
Mixed nutrition has its own characteristics, which are very important for a nursing mother to know.
Basic rules for mixed feeding:
- The timing of the introduction of complementary foods depends on the amount of breast milk the baby receives. If it is 50-70%, then it is administered as with breastfeeding (at 6 months). If less than 50% of breast milk is present in the baby's diet, then complementary foods can be introduced at the age of 5 months.
- Always offer the breast first. Only if you see that the baby is not full, and the breasts are empty, then give him a mixture. It also helps increase lactation.
 The mixture should be introduced gradually. On the first day - 10 ml / 1 time, the second - 10 ml / 3 times, the third - 20 ml / 3 times. Increase the portion, bringing it to the norm.
The mixture should be introduced gradually. On the first day - 10 ml / 1 time, the second - 10 ml / 3 times, the third - 20 ml / 3 times. Increase the portion, bringing it to the norm. - Only the breast should be given at night and formula should be avoided. This is due to the fact that from 3 to 8 am, prolactin is actively produced, which is responsible for lactation.
- Feed according to schedule (every 3-4 hours) and breastfeed on demand.
- Keep water boiled and utensils and formula sterile. You need to cook right before eating.
- Use a spoon instead of a bottle for complementary foods. Then you can avoid breast rejection.
- Remember that mixed-fed babies should be given water, as dehydration can lead to poor digestion.
Follow these simple rules and try to keep your baby breastfed for as long as possible. Your milk, even though it's not your baby's only food, contains invaluable trace minerals that will keep your baby healthy and strong.
Back to Contents
The information in this article is for reference only and does not replace professional medical advice. For diagnosis and treatment, contact a qualified specialist.
Women's consultations | Genus. House number 5
The function of the mammary glands after childbirth reaches its highest development. During pregnancy, milk ducts form and glandular tissue grows. Under the influence of prolactin, blood flows intensively to the mammary glands and increased secretion of milk begins. Mother's milk is the only natural biological product that provides physiologically adequate nutrition for infants. It is the gold standard for early childhood nutrition.
Women's breasts are a generous source of baby food that can saturate the baby's growing body with the necessary substances, protect it from diseases, and bind mother and child together for several hours a day.
Breastfeeding is a soft and optimal postpartum adaptation of mother and child, the basis for the health and proper development of the child.
BREASTFEEDING BENEFITS
Breastfeeding promotes the formation of a close, tender relationship between mother and child, from which the mother receives emotional deep satisfaction. Close contact with the child immediately after birth helps to establish these relationships. Feeding time is not just for feeding your baby, it gives you the opportunity to get to know and love each other. Babies cry less and develop faster if they stay with their mothers immediately after birth. Breastfeeding mothers respond affectionately to their children.
Mother's milk is the only food that fully meets the needs of the newborn. It is easily digested and completely absorbed, has the necessary temperature, contains antibodies that help protect the child from certain infections and allergies. Breastfeeding helps avoid unwanted pregnancies, protects the health of the mother, and is less expensive than artificial nutrition. Contributes to the best social adaptation of the child
It is important to have the desire to breastfeed even during pregnancy, and for this you need to learn, because pregnancy is just the right time to replenish your knowledge about the health of the unborn baby.
The amount of breast milk depends in part on the thoughts, feelings and sensations of the mother. It is important that the baby and the mother are together all the time, day and night, it is necessary to help the mother so that she strives to continue breastfeeding. Many difficulties can arise from improper attachment of the baby to the breast. The amount of milk in the breast depends on how long the baby suckles and how much milk he sucks. The more the baby suckles, the more milk the mother produces. Breastfeeding will be successful in most cases if the mother feels well, the baby is properly attached to the breast to allow him to suckle effectively, the baby suckles as often and for as long as he wants, and the environment is conducive to breastfeeding. For the formation of a warm relationship, it is necessary that the mother stroke the child during feeding, look at him, talk to him. Those sensations that the child receives during feeding, according to some reports, can affect his entire subsequent life.![]()
Sucking for a baby is a necessity and a pleasure that is not directly related to the feeling of hunger. Thanks to sucking, the baby develops the jaw apparatus, muscles of the mouth and tongue, which is important in the development of speech .
Two hormones involved in milk production are prolactin and oxytocin. Oxytocin is produced before and during feeding. The baby suckles the breast, sensory impulses come from the nipple to the pituitary gland, oxytocin enters the bloodstream and acts on muscle cells, causing them to contract and milk to be released. The release of oxytocin promotes uterine contraction. Prolactin is released after feeding to prepare the next feeding. The baby suckles the breast, sensory impulses from the nipple go to the pituitary gland. Entering the blood, prolactin acts on the cells that secrete milk and ducts, forcing them to secrete milk. Prolactin - inhibits ovulation, preventing unwanted pregnancy.
CHANGES IN THE COMPOSITION OF MILK
Colostrum is breast milk that is produced in a woman within 3-5 days after birth. It is thick yellowish in color, rich in immunoglobulins, which provides protection against infections and allergies. It has a laxative effect, promotes the removal of meconium and helps prevent jaundice. Contains growth factors, promotes intestinal maturation. Rich in vitamin A, prevents eye diseases.
It is thick yellowish in color, rich in immunoglobulins, which provides protection against infections and allergies. It has a laxative effect, promotes the removal of meconium and helps prevent jaundice. Contains growth factors, promotes intestinal maturation. Rich in vitamin A, prevents eye diseases.
Mature milk is milk produced after a few days, its amount increases, the breasts fill up, swell and become heavy. This moment is called the arrival of milk.
A distinction is also made between foremilk and hindmilk.
Foremilk is produced at the beginning of feeding, has a bluish tint and is produced in large volume, providing the baby with a sufficient amount of proteins, lactose and other components. Since the baby consumes a lot of foremilk, he receives with him all the amount of water he needs and he does not need to give additional water in the first six months of life. If he quenches his thirst with water, he will consume a small amount of milk. For the same reason that foremilk and hindmilk are different in composition, it is necessary to feed the baby in one feeding with one breast.
For the same reason that foremilk and hindmilk are different in composition, it is necessary to feed the baby in one feeding with one breast.
Hindmilk is the milk produced at the end of a feeding and is whiter in color because it contains more fat, which is the main source of nutrition during breastfeeding. Mother's milk has a unique individual composition, polyunsaturated fatty acids of breast milk contribute to the development of the brain.
A child is born with innate skills, and has:
Grasping reflex - when something touches the child's lips, he opens his mouth, the tongue goes down and moves forward.
Sucking reflex - when something touches the child's palate, he starts to suck.
Swallowing reflex - when the baby's mouth fills with milk, he swallows. These reflexes are especially pronounced in the first hour after birth, so it is very important to start breastfeeding during this period.
By carefully observing the baby, the midwife or nurse notes the signs of the newborn's readiness to suckle the breast (opens the mouth, sticks out the tongue, turns the head, tries to crawl towards the breast) and draws the attention of the mother to them. And then they help to attach the baby to the breast for the first time.
And then they help to attach the baby to the breast for the first time.
To do this, the mother and child are located in the same plane, the mother needs to relax and listen to her feelings. The child should not be in diapers, he is pressed tightly against the mother's body. The mother presses the buttocks with her elbow, holds the back with her forearm, and the hand slightly supports the head, without pressing it to the chest. The child's nose is located at the level of the nipple or slightly higher, the mother takes the breast in such a way that 4 fingers are located under the breast, and one large one is on top. We move the nipple of the breast along the lips and nose of the child, it is necessary that the child opens his mouth wide and then he will grasp the breast well, it is necessary to carefully insert the nipple together with the areola into the child's mouth, directing the nipple to the upper palate. From the captured nipple and areola, a nipple is formed, in which the nipple occupies only 1/3 of the part. The child begins to suck quickly, then the sucking movements become more rare, measured, which indicates a good milk flow. As a rule, the child himself releases the breast, satisfied and sleepy.
The child begins to suck quickly, then the sucking movements become more rare, measured, which indicates a good milk flow. As a rule, the child himself releases the breast, satisfied and sleepy.
Signs of proper breastfeeding .
-
The baby's mouth is wide open;
- chin and nose touching the chest;
-
mother and child are in the same plane;
-
the child captures most of the areola, more from below than from above;
-
the tip of the nipple is in the depths of the mouth and touches its soft palate;
-
baby's cheeks are round,
-
the lower lip is turned outward;
-
the child makes swallowing movements.
-
the mother is not in pain, the child is happy.
Correct and incorrect application
Timely mastering the technique of applying the baby to the breast minimizes the appearance of possible problems that arise during breastfeeding.
On the first day, newborns may require the breast no more than 2-4 times. However, the main task of the mother is to learn how to give the child the breast correctly, and the child to suckle correctly. For this purpose, on the first day, it is advisable to put the baby to the chest during the day up to 10 times, and at night as many times as he wakes up.
Starting from 2-3 days after birth, breastfeeding is carried out at the request of the child. The mother must learn to recognize when the child asks for food, and not offer him the breast as soon as he shows concern, for any reason. However, free (on demand) feeding, during the neonatal period, for a number of reasons (the formation of lactation, the small size of the child's stomach, a high metabolic rate) requires quite frequent (from 7-8 to 12-16 times a day) energy intake into the child's body. and plastic material. Breast milk contains a sufficient amount of liquid, therefore, as a rule, there is no need for regular (daily) supplementation of the child with water. Water can carry the risk of infection and lack of demand for breast milk in sufficient quantities.
Water can carry the risk of infection and lack of demand for breast milk in sufficient quantities.
On the other hand, sometimes babies may just want water instead of the liquid in breast milk. Once complementary foods are introduced, water can be offered daily. Mothers must learn to identify the water needs of a child. Exclusively breastfed babies tend to wake up at night and need to be fed. By the way, frequent awakenings of the child also have a positive side, because. waking up and awake reduces the risk of sudden death syndrome.
The success of maintaining and maintaining lactation largely depends on the ability of the mother and child to give and take the breast.
There are several ways to breastfeed a baby: lying down (on the side, on the back), sitting (holding the baby in the cradle position or from under the arm), standing up (upright or bent over a lying child), from under the arm . The most common position used by mothers to feed their babies is sitting. However, in almost all these positions, especially during the neonatal period, it is necessary to ensure closer contact between mother and child. Babies learn the world through sensations, and the more pleasant these sensations are, the more benevolent and calmer your child will be, and along with him, you.
However, in almost all these positions, especially during the neonatal period, it is necessary to ensure closer contact between mother and child. Babies learn the world through sensations, and the more pleasant these sensations are, the more benevolent and calmer your child will be, and along with him, you.
Current provisions for breastfeeding
« Classic cradle»
The child is located in the arms of the mother, as in a cradle: his head is on the elbow of one arm, with the other hand, the mother grabs and holds the back. The baby is turned to the mother "belly to stomach", and his mouth is directly opposite the nipple. In this position, the mother can feed from both the right and left breasts, shifting the baby's head from one hand to the other. A variation of this pose can be called standing feeding. The baby in the mother's arms is in the same position, only the mother herself does not sit, as is most often the case, but stands. Usually, this is how babies are fed during motion sickness and when they go to bed, with stitches on the perineum, when you can’t sit.
Usually, this is how babies are fed during motion sickness and when they go to bed, with stitches on the perineum, when you can’t sit.
"cross cradle"
The sitting mother holds the child with one hand - the opposite breastfeeding breast. His head rests in his mother's palm, and his body supports her forearm. This position is relevant in establishing a correct grip on the breast by a child, more often in premature babies
hand feeding
Mom sits straight, the child is under her arm on the side, at chest level, with her head towards her knees. A pregnancy pillow can be used to support the baby. This position is relevant when feeding twins, with blockage of the milk duct, with difficulties in grabbing the breast, with flat nipples, with the prevention of congestion in the lower and lateral segments of the mammary glands, with nipple cracks
Twin feeding
Feeding two children is very different from feeding one child.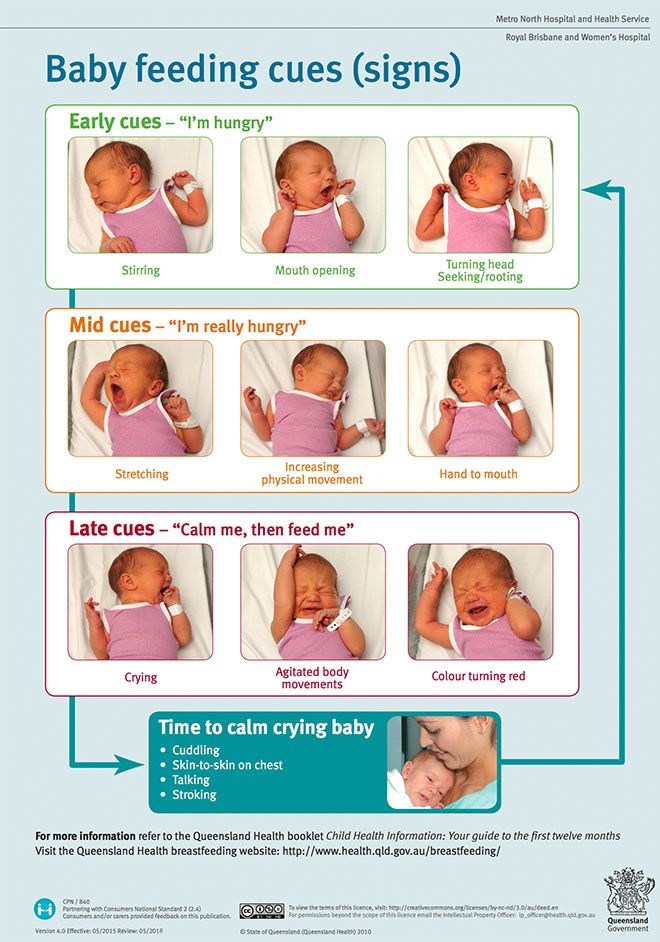 It can be organized in different ways. You can feed each separately. But in this way, more time per day for feeding may be required. You can feed at the same time.
It can be organized in different ways. You can feed each separately. But in this way, more time per day for feeding may be required. You can feed at the same time.
Try, in a combination of individual and group feedings, to give each baby at least one "personal" feeding per day. This approach cuts down on the total number of feeding hours, but allows you to have a little interaction with each one. You might want to put your expressed milk in the refrigerator so dad can give it to another baby during private feedings, or so you can get some sleep. Parents should be aware that each of the twins has its own personality. Their needs and diet are different. Please don't treat twins the same.
Frequent and prolonged breast sucking and an “empty breast” that seems to you is not a reason for supplementing a child with artificial mixtures. Before taking this serious step, be sure to check with your doctor, a breastfeeding specialist, remember that other liquid tea, water, milk formula, suppresses appetite. The newborn will not actively suckle the breast and this will lead to a decrease in milk production. One of the most common reasons mothers switch to bottle-feeding or stop breastfeeding is because they believe they are “not getting enough milk.” Studies show that less than 1% of women have actual physiological causes for inadequate milk production.
The newborn will not actively suckle the breast and this will lead to a decrease in milk production. One of the most common reasons mothers switch to bottle-feeding or stop breastfeeding is because they believe they are “not getting enough milk.” Studies show that less than 1% of women have actual physiological causes for inadequate milk production.
Signs of insufficient breast milk
If the mother does not have enough milk, the child has a feeling of hunger - the state of his health, as well as development in the first months of life, can be significantly shaken.
Therefore, you should pay attention to a number of signs of milk deficiency:
Valid:
Poor weight gain (in two weeks the child did not restore the “physiological” weight loss or gained less than 500 g in one month), 125 g in 1 week.
The average daily weight gain is less than 20 grams.
Infrequent urination with concentrated urine (less than 6 urination per day, provided that it is not supplemented with water, yellow urine).
Likely:
baby cries often
very frequent breastfeeding (after 1-1.5 hours)
Very long breastfeeding (more than 30 minutes)
stool rare, dense, "hungry", dry, not yellow
The mother feels that there is no milk in the mammary glands
If you notice such signs - do not make an independent decision about feeding the baby! Be sure to discuss this with your doctor or pediatric nutritionist.
Breast milk sufficiency criteria.
If a child gains weight at least 500 grams per month and urinates at least 6-8 times a day, his skin is of normal moisture, which means that he is getting enough milk.
Lactation crisis - temporary decrease in milk production, after seemingly already established lactation. The reasons for the decrease in milk production may be associated with periods of intensive growth of the child, with the physical or mental overwork of the mother, with hormonal changes in the woman's body (resumption of menstruation), with a sharp restriction in fluid and food intake, as well as with the mother's illness.
Calm down and believe that lactation will definitely be restored.
To restore a sufficient amount of milk produced, continue frequent breastfeeding (up to 10-15 times a day), including at night. Feed from both breasts in one feeding, be with the baby around the clock, sleep with him. Try to rest and improve your diet. Ask your family and friends to do housework. Use special lactogenic drinks, herbal teas, homeopathic medicines. Be sure to make sure that you are feeding your baby properly and that he is suckling properly. Do not hesitate to contact a medical institution for help. In the antenatal clinic, maternity hospital, children's clinics, the staff will do everything possible for the success of your breastfeeding.
A few tips: it is very good to drink hot freshly brewed green tea (you can use it with milk), juice, any fermented milk drink just before feeding. Various lactogenic drinks perfectly stimulate lactation. For example, blackcurrant juice, milk infusion with walnuts increases milk production. Since ancient times, various collections of lactogenic herbs have been used in folk medicine, but medicinal plants must be used very carefully .
Since ancient times, various collections of lactogenic herbs have been used in folk medicine, but medicinal plants must be used very carefully .
For this reason, instant herbal teas of industrial production, produced by both domestic and foreign manufacturers, are of undoubted interest. Cooking them is very fast and convenient, besides, the components included in them undergo strict environmental control. Instant herbal teas from different manufacturers differ from each other in composition, the number of herbs they contain, and the presence of additional additives. They not only increase lactation, but also have a general strengthening effect, promote good sleep, relieve the mother’s neuro-emotional stress, and normalize the functioning of the intestines of a nursing woman. Such tea well satisfies the increased need for fluid that occurs in the mother during breastfeeding, and also becomes an additional source of vitamins, but be careful not to overdose!
Laktostasis is the stagnation of milk, occurs when one or more lobes of the mammary gland cease to be released from milk. The duct leading to the lobe remains blocked. Your child can help you deal with lactose intolerance. To do this, apply the baby more often to the chest so that his chin is directed towards the seal. After a few feedings, you will notice how the seal becomes smaller. If the baby is unable to suckle, express milk manually or with a breast pump. Before feeding or pumping, apply a warm compress, do a light massage of the breast. After feeding or pumping, you can put a towel moistened with cold water on your chest for 5-10 minutes. Cold will help relieve discomfort and reduce the flow of milk into the stagnant lobe.
The duct leading to the lobe remains blocked. Your child can help you deal with lactose intolerance. To do this, apply the baby more often to the chest so that his chin is directed towards the seal. After a few feedings, you will notice how the seal becomes smaller. If the baby is unable to suckle, express milk manually or with a breast pump. Before feeding or pumping, apply a warm compress, do a light massage of the breast. After feeding or pumping, you can put a towel moistened with cold water on your chest for 5-10 minutes. Cold will help relieve discomfort and reduce the flow of milk into the stagnant lobe.
You should not use alcohol-based compresses, you can replace them with compresses from a mashed cabbage leaf
If the seal does not go away within a day, consult a doctor to prevent a serious problem like mastitis.
Milk stasis (Lactostasis) is a temporary difficulty that, with the right tactics of management, can be easily dealt with!
When, how and how much to express breast milk?
Readings :
Possibly while in the maternity hospital, for a successful start of lactation
On days of lactation crises, for additional stimulation of the mammary glands
· To leave milk in your absence
· With engorgement of the mammary glands
For feeding a low birth weight or weak baby
· When it is necessary to alleviate the condition of the mother. Usually this situation occurs with the "tides" of breast milk. To alleviate the condition, milk is not completely expressed, but only until the mother feels comfortable
Usually this situation occurs with the "tides" of breast milk. To alleviate the condition, milk is not completely expressed, but only until the mother feels comfortable
· To create an individual breast milk bank.
No equipment is required to express breast milk. Wash your hands thoroughly, sit/stand comfortably with the milk collection vessel next to your breast. The thumb is set on top along the edge of the halo, the index finger is opposite from below. Slightly press the gland towards the chest, then point the index finger and thumb towards each other. If the pumping technique is correct, then the woman does not experience pain. It is not recommended to place the nipple between other fingers, as the milk duct may be squeezed, which can cause milk stasis. The first movement of the brush is carried out towards the chest. Then the movement of the fingers of the 1st and 2-3rd towards each other is carried out. Pumping movements must be alternated with massaging the chest. The procedure is repeated until the breast is soft. Fingers should not touch the nipple. Please also note that when pumping by hand, the purity of the milk is violated, a large number of microorganisms enter it, which creates the danger of the development of harmful bacterial flora. Therefore, hand-expressed milk must be consumed within 2 hours and is not recommended for freezing and breast milk banking.
The procedure is repeated until the breast is soft. Fingers should not touch the nipple. Please also note that when pumping by hand, the purity of the milk is violated, a large number of microorganisms enter it, which creates the danger of the development of harmful bacterial flora. Therefore, hand-expressed milk must be consumed within 2 hours and is not recommended for freezing and breast milk banking.
Expression with a breast pump
In some cases, there are problems that prevent normal sucking and emptying of the mammary gland, which leads to the formation of lactostasis and threatens the development of mastitis.
Manual pumping requires skills and strength, so mothers need to learn how to use modern breast pumps.
Breast pumps are designed for gentle and comfortable pumping of breast milk. During the period of formation, maintenance of lactation or the creation of a breast milk bank, breast pumps may be required by every woman who is breastfeeding a child.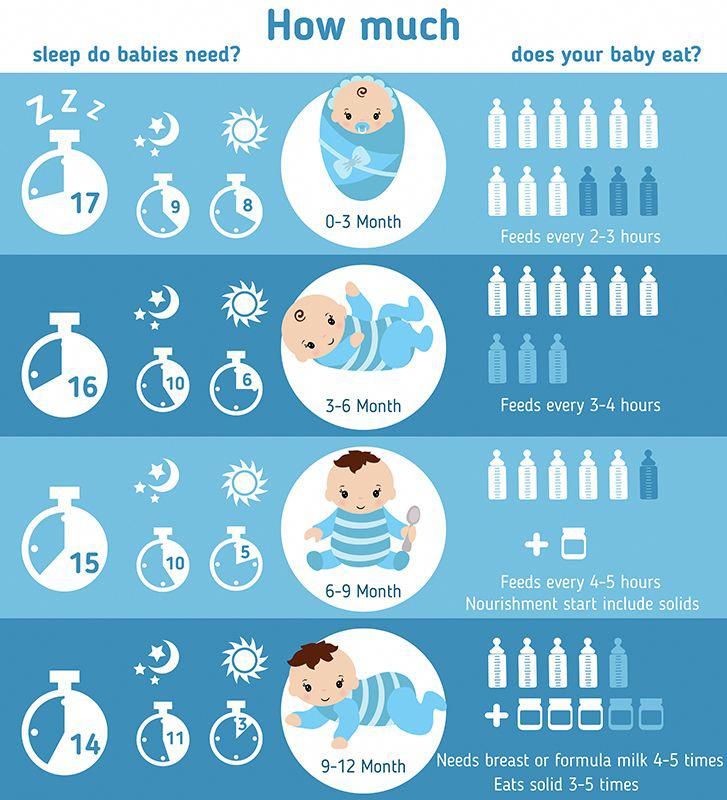
Sometimes a mother can be separated from her baby. The breast pump will allow her to express milk in such a way that the breastfeeding process will not be interrupted.
Using a breast pump will help eliminate lactose and also ensure that the mammary glands receive the stimulation they need to increase milk production.
If a mother works outside the home, using a breast pump will allow her to go to work and continue breastfeeding. In addition, the breast pump provides the opportunity to breastfeed premature babies or those who have difficulty suckling.
Setting up a breast milk bank
During breastfeeding, situations may arise when a nursing mother needs to express and store milk for her baby. This happens when a mother needs to be away from home, when a mother must undergo a course of treatment that makes it impossible to breastfeed. In all these cases, prolonging breastfeeding will help INDIVIDUAL BREAST MILK BANK . It is personal expressed breast milk, which is placed in portions in convenient containers, stored at low temperatures and can be used to feed the baby at any time.
It is personal expressed breast milk, which is placed in portions in convenient containers, stored at low temperatures and can be used to feed the baby at any time.
In the first months of a baby's life, the mother usually produces more milk than is necessary for feeding the baby. During this period, it is recommended to prepare milk for future use. The safety of the quality of frozen breast milk also depends on the container in which it is stored. Glass containers are the least convenient, as they can burst or break. In addition, some biologically active components adhere strongly to the glass and are thus lost from the milk. This disadvantage is less inherent in plastic bags and polypropylene containers. They are sold sterile packaged and do not need to be sterilized before first use. Allow multiple sterilization.
The container with a portion of expressed milk should be tightly closed with a lid. If you use bags, tightly snap a special fastener on them. Write the date and time of pumping on the surface of the container. Milk from multiple pumping episodes in the same day can be pooled into one serving. After each pumping, the milk should be placed in the refrigerator, taken out after the next pumping to top up the next portion, and placed again in the refrigerator. 150-200 ml is an approximate portion, sufficient for one feeding.
Milk from multiple pumping episodes in the same day can be pooled into one serving. After each pumping, the milk should be placed in the refrigerator, taken out after the next pumping to top up the next portion, and placed again in the refrigerator. 150-200 ml is an approximate portion, sufficient for one feeding.
Breast milk should be stored in tight plastic or glass containers, or in special bags for storing frozen milk.
IMPORTANT Remember that before adding a new batch to already frozen milk, it must be cooled.
Milk that has been at room temperature for 2 hours must not be frozen or refrigerated!
Thawed milk cannot be re-frozen, but can be stored in the refrigerator for up to 24 hours.
thawed breast milk
Frozen breast milk that has been reheated can be left in the refrigerator for up to 24 hours. Attention! It is impossible to re-freeze such milk!
How to heat breast milk
In order to defrost milk, you need to put the container in the refrigerator chamber. Then, after it melts, heat to room temperature. After that there are several ways:
Then, after it melts, heat to room temperature. After that there are several ways:
Warm up in a water bath to 30-35 ° C. This method is low-cost and technically not always easy to use. In addition, it is difficult to control the temperature of the milk, so overheating is possible.
REMEMBER: only boil-resistant, BPA-free bottles may be placed in the water bath*
*a harmful substance contained in the polycarbonate used in the production of traditional low-price plastic bottles. When heated or when food is stored for a long time in a dish, Bisphenol-A passes from plastic to food. Dangerous even in very small quantities.
Under running hot water. Shake the bottle periodically to evenly distribute the heat. Use special surface thermometers to monitor temperature changes.
In a bottle warmer. Specially designed for warming baby food, the devices are equipped with a thermostat, you only need to set the desired temperature. At the same time, overheating of milk is excluded, and, therefore, all useful substances are preserved.
Do not heat breast milk in the microwave! During heating, it is difficult to control the temperature of the milk. In addition, some pediatricians consider the use of microwave technologies to be wrong, since a microwave can be used to sterilize, for example, dishes, during which vitamins and other biologically active substances are destroyed.
How long to breastfeed?
Let the little creature determine the duration of breastfeeding
The child continues to receive vitamins and other nutrients in the second year of life. Breast sucking for a child older than a year is needed not so much to get enough, but to communicate with his mother. Responding to anxiety and crying by breastfeeding, you form in the crumbs the confidence that mom is always there and ready to help.
Listen to our advice - and you will succeed!
· Begin breastfeeding within the first 30-40 minutes after delivery.