Feeding plates for cleft babies
Clear double layer Bioplast feeding plate for neonates with cleft palate
Eur J Dent. 2015 Oct-Dec; 9(4): 610–613.
doi: 10.4103/1305-7456.172629
,1,1 and 1
Author information Copyright and License information Disclaimer
An infant with cleft palate was referred to cleft clinic of the Orthodontic Department. The mother was concerned to feed the child because of the escape of milk from the nose. Intraoral examination revealed a large palatal cleft extending from hard to soft palate involving uvula. The impression was taken and dental cast obtained. A 3 mm soft and afterward a 1 mm hard Bioplast plate was pressed using Biostar device (Scheu-Dental Gmbh, Iserlohn, Germany) on the model. Finally, a hole was prepared on the anterior part to put a thread through it. The infant tolerated the plate immediately and encounters no difficulties during feeding. The inlaying soft Bioplast plates eliminate the risk of tissue irritation, whereas the covering hard Bioplast plate supplies endurance. The fabrication of the clear Bioplast feeding plate is easy and less time-consuming compared with acrylic plates and may be recommended in crowded and overloaded cleft centers.
Keywords: Bioplast feeding plate, cleft palate, infancy
Cleft lip and palate (CLP) is the second most common major congenital anomaly in the Turkish population.[1] The incidence is approximately 0.6% and more frequently recorded in Black Sea, South Eastern Anatolia, and Aegean region of Turkey.[2]
CLP has a complex genetic and environmental etiology associated with dental anomalies.[3,4] Infants with CLP have esthetic and functional problems. Infants with only cleft palate have not an atypical facial appearance but also functional problems, especially with feeding. In fact, the first highlighted topic of parents of infants with CLP after birth is how to feed their baby.[5] Recent studies suggested that the abnormal facial appearance not affected the mother-child relationship. [6,7] However, the longer feeding period and the disruption of feeding rhythm due to emission through the nose may lead to frustration of the mother.[8]
[6,7] However, the longer feeding period and the disruption of feeding rhythm due to emission through the nose may lead to frustration of the mother.[8]
In infants with cleft palate the anatomical obstruction between the oral and nasal cavity is not present, and feeding is a really hard job for the parents: Negative pressure required for sucking cannot be created, nasal regurgitation, and burping due to air intake during deglutition and choking make the feeding more problematic.[9,10] The parents are frequently in “psychosocial emergency,” in other words in a period of severe emotional crisis, and the anxiety of inability of adequate feeding the infant is not welcomed.[11,12,13]
Several specialists are involved in the management of CLP patients and work as a team. The orthodontist is one of the first specialists contacting with the infant as soon as possible after birth. The infants with cleft palate get maxillary feeding plates (obturators) in orthodontic clinics. Traditionally, the plate is made of clear acrylic using conventional methods. The fabrication of such a plate is time-consuming and soft tissue injuries are frequently observed due to the rigidity of this material.[14,15] Therefore, the objective of this case report is to present a quick and easy method to fabricate a feeding plate of double layer Bioplast material in a patient with an isolated soft and hard palate cleft.
Traditionally, the plate is made of clear acrylic using conventional methods. The fabrication of such a plate is time-consuming and soft tissue injuries are frequently observed due to the rigidity of this material.[14,15] Therefore, the objective of this case report is to present a quick and easy method to fabricate a feeding plate of double layer Bioplast material in a patient with an isolated soft and hard palate cleft.
A 7-day-old male infant with cleft palate was referred to the cleft clinic. The mother was concerned to feed the child because of the escape of milk from the nose. In addition, the milk intake was not satisfying the pediatrician. The intraoral evaluation revealed a large palatal cleft extending from hard to soft palate involving uvula []. The impression was taken in the operating room with C-silicone material (Zetaplus®, Zhermack, Bedia Polesine, Italy) under the supervision of the general anesthestist. Afterward, dental plaster cast models were obtained. A 3 mm Bioplast clear plate (soft plate) was pressed on the model using the Biostar device (Scheu-Dental Gmbh, Iserlohn, Germany) [Figure and ]. After trimming the edges of the soft plate, it was placed again on the cast and 1 mm Biocryl C Rose transparent plate (hard plate) was pressed. The edges of the plate were again trimmed so that the hard plate covering was 1 mm shorter than the soft plate. After final polishing, a hole was drilled on the anterior part []. A thread was applied through the hole to attach to one finger of the mother to prevent any emergencies []. Approximately, 1 h after the impression taking procedure, the Bioplast clear feeding plate was delivered to the infant. After the last control of the borders of the plate, the feeding process was started. The infant adapted immediately without any problems. The mother was educated about cleaning, insertion, and removal of the appliance. Two days later, an additional appointment was arranged to evaluate any complaints with using the feeding plate.
A 3 mm Bioplast clear plate (soft plate) was pressed on the model using the Biostar device (Scheu-Dental Gmbh, Iserlohn, Germany) [Figure and ]. After trimming the edges of the soft plate, it was placed again on the cast and 1 mm Biocryl C Rose transparent plate (hard plate) was pressed. The edges of the plate were again trimmed so that the hard plate covering was 1 mm shorter than the soft plate. After final polishing, a hole was drilled on the anterior part []. A thread was applied through the hole to attach to one finger of the mother to prevent any emergencies []. Approximately, 1 h after the impression taking procedure, the Bioplast clear feeding plate was delivered to the infant. After the last control of the borders of the plate, the feeding process was started. The infant adapted immediately without any problems. The mother was educated about cleaning, insertion, and removal of the appliance. Two days later, an additional appointment was arranged to evaluate any complaints with using the feeding plate./pub/media/catalog/product/b/b/bbluv-plato-pink.jpg) The intraoral evaluation revealed no soft tissue irritations. The infant was followed up periodically every month. The mother mentioned that the nutrition intake and weight gain was found adequate by the pediatrician.
The intraoral evaluation revealed no soft tissue irritations. The infant was followed up periodically every month. The mother mentioned that the nutrition intake and weight gain was found adequate by the pediatrician.
Open in a separate window
Intraoral photograph presenting a large palatal cleft, extending from hard to soft palate involving uvula
Open in a separate window
Fabrication of feeding plate using Biostar device (Scheu-Dental Gmbh, Iserlohn, Germany), (a) during, and (b) after pressing process of Bioblast plate
Open in a separate window
Feeding plate after (a) final polishing and a hole drilling on anterior part, (b) a thread was applied through the hole to attach to one finger of the mother to prevent any emergencies during feeding
Management of patients with cleft is a longstanding period starting at the birth and not ending until skeletal maturity.[16] Specialists from different disciplines such as pediatrics, plastic and reconstructive surgery, maxillofacial surgery, orthodontics, genetics, ear-nose-throat, psychology, and speech therapy are involved in the treatment. The orthodontist is involved in the treatment team at an early period infancy.[17]
The orthodontist is involved in the treatment team at an early period infancy.[17]
The infants with CLP get presurgical orthopedic therapy in the first months, whereas infants with cleft palate are treated with feeding obturators/plates. Feeding plates are only preferred in cases that will benefit from it. For example, in cases with small dimensional, notch-like, and on soft palate located clefts, information of the upright feeding position may be more helpful for the parents instead of serving a plate.[18] Feeding plates are only used in cases with large clefts involving the hard palate. The advantages of such plates were described as facilitation of feeding, normalization of tongue position, the guidance of maxillary growth, and prevention of collapse of alveolar segments and also improvement of the psychology of parents.[9]
Our cleft clinic, as a part of the orthodontic department, is a crowded and workload clinic dealing with approximately 100 infants pro year. The majority of the patient population has complete CLP. These patients get nasoalveolar molding therapy to enhance esthetic and function. After the fabrication of the intraoral plate, the patient was followed up with weekly appointments by two specialists until the lip surgery at approximately 3–4 months of age. The intraoral plate has to be used 24 h/day except the cleaning period. The estimated follow-up visits in an infant with a unilateral cleft is approximately 13–14 times.[18] In these appointments, modifications rather than new appliance fabrication were performed.[16,19] On the other hand, in cases with isolated palatal clefts, feeding plates are preferred to enhance the feeding activity. The feeding plate is used only during the feeding activity. After the fabrication of the first plate, the patients are followed at monthly intervals until the palatal surgery at approximately 1-year of age. In approximately every third appointment, the plates were renewed because of the growth of the infant.
The majority of the patient population has complete CLP. These patients get nasoalveolar molding therapy to enhance esthetic and function. After the fabrication of the intraoral plate, the patient was followed up with weekly appointments by two specialists until the lip surgery at approximately 3–4 months of age. The intraoral plate has to be used 24 h/day except the cleaning period. The estimated follow-up visits in an infant with a unilateral cleft is approximately 13–14 times.[18] In these appointments, modifications rather than new appliance fabrication were performed.[16,19] On the other hand, in cases with isolated palatal clefts, feeding plates are preferred to enhance the feeding activity. The feeding plate is used only during the feeding activity. After the fabrication of the first plate, the patients are followed at monthly intervals until the palatal surgery at approximately 1-year of age. In approximately every third appointment, the plates were renewed because of the growth of the infant. In summary, in cases with cleft palate approximately 3–4 appliances are fabricated.
In summary, in cases with cleft palate approximately 3–4 appliances are fabricated.
Over years, acrylic materials were used for fabrications of these plates in our clinics.[14] However, acrylic resin has disadvantages such as: (1) Time consuming, (2) complicated fabrication, and (3) prone to soft tissue irritation, and therefore not well-tolerated by the infant. In crowded and workload cleft centers the time to fabricate such plates is of essential importance. Therefore, the aim of the presented case report was to present a quick, easy method to fabricate a feeding plate, which also not irritates the soft tissue resulting in a well adaptation by the infant.
Bioplast material was preferred in the fabrication of feeding plates by Erkan et al.[11] They used such a plate to obstruct the soft palate cleft in a patient with unilateral CLP. They suggested that if the bulb of the appliances set in the cleft is fabricated from 1 mm Bioplast clear soft plates, the adaptation is excellent, and the movements are synchronized with functions. However, in the present case the aim by Bioplast soft plate was to prevent soft tissue irritation and not to obstruct the cleft. Intraoral soft tissue complications are not rare during the presurgical orthopedic treatment period. Uneven flanges or unrelieved areas of the inner surface of the plate may cause to ulcerations.[15] In the present case report, 3 mm soft Bioplast plate was used as an inner layer to prevent any soft tissue irritations. In addition, the hard Bioplast plate was removed 1 mm above the borders of the feeding plate, to obtain the only contact between the soft Bioplast plate and soft tissue. The hard Bioplast plate enhance the endurance of the plate, indeed no breakage was encountered.
However, in the present case the aim by Bioplast soft plate was to prevent soft tissue irritation and not to obstruct the cleft. Intraoral soft tissue complications are not rare during the presurgical orthopedic treatment period. Uneven flanges or unrelieved areas of the inner surface of the plate may cause to ulcerations.[15] In the present case report, 3 mm soft Bioplast plate was used as an inner layer to prevent any soft tissue irritations. In addition, the hard Bioplast plate was removed 1 mm above the borders of the feeding plate, to obtain the only contact between the soft Bioplast plate and soft tissue. The hard Bioplast plate enhance the endurance of the plate, indeed no breakage was encountered.
The present case report showed a new approach to fabricate feeding plates using Bioplast material in infants with cleft palate. Traditionally presurgical orthopedic treatment appliances fabricated of acrylic are preferred in patients with CLP. The aim of these appliances is first to align the alveolar segments by adding of and removing of soft and hard acrylic and secondly to perform nasal molding. The most advantage of Bioplast feeding plate is that it speeds the fabrication time. Probably the plate for nasoalveolar molding can be fabricated from Bioplast material. However, the nasal stent coverage and also the modifications may need soft acrylic usage. Consequently, if Bioplast material is also advantageous in infants with CLP is questionable and need forthcoming research. Overall, this is a case report and studies about the performance, time consumption, and comfort are also required to take this method into routine management.
The most advantage of Bioplast feeding plate is that it speeds the fabrication time. Probably the plate for nasoalveolar molding can be fabricated from Bioplast material. However, the nasal stent coverage and also the modifications may need soft acrylic usage. Consequently, if Bioplast material is also advantageous in infants with CLP is questionable and need forthcoming research. Overall, this is a case report and studies about the performance, time consumption, and comfort are also required to take this method into routine management.
The fabrication of a feeding plate of double layer clear Bioplast material for infants with cleft palate is advantageous. The inlaying soft Bioplast plates eliminate the risk of tissue irritation, whereas the covering hard Bioplast plate supplies endurance. Therefore, the Bioplast feeding plate was handy for the mother and also well-tolerated by the infant. Overall, the fabrication of the clear Bioplast feeding plate is easy and less time-consuming compared with acrylic plates and may be recommended in crowded and overloaded cleft centers.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
1. Tomatir AG, Demirhan H, Sorkun HC, Köksal A, Ozerdem F, Cilengir N. Major congenital anomalies: A five-year retrospective regional study in Turkey. Genet Mol Res. 2009;8:19–27. [PubMed] [Google Scholar]
2. Nur RB, İlhan D, Fişekçioğlu E, Oktay İ, Arun T. Prevalence of orthodontic malocclusion and evaluation criteria in 7 geographic regions of Turkey. Turk J Orthod. 2014;26:154–61. [Google Scholar]
3. Cakan DG, Ulkur F, Taner T. The genetic basis of dental anomalies and its relation to orthodontics. Eur J Dent. 2013;7(Suppl 1):S143–7. [PMC free article] [PubMed] [Google Scholar]
4. Subasioglu A, Savas S, Kucukyilmaz E, Kesim S, Yagci A, Dundar M. Genetic background of supernumerary teeth. Eur J Dent. 2015;9:153–8. [PMC free article] [PubMed] [Google Scholar]
5. Chuacharoen R, Ritthagol W, Hunsrisakhun J, Nilmanat K. Felt needs of parents who have a 0- to 3-month-old child with a cleft lip and palate. Cleft Palate Craniofac J. 2009;46:252–7. [PubMed] [Google Scholar]
Cleft Palate Craniofac J. 2009;46:252–7. [PubMed] [Google Scholar]
6. Speltz ML, Armsden GC, Clarren SS. Effects of craniofacial birth defects on maternal functioning postinfancy. J Pediatr Psychol. 1990;15:177–96. [PubMed] [Google Scholar]
7. Maris CL, Endriga MC, Speltz ML, Jones K, DeKlyen M. Are infants with orofacial clefts at risk for insecure mother-child attachments? Cleft Palate Craniofac J. 2000;37:257–65. [PubMed] [Google Scholar]
8. Pruzinsky T. Social and psychological effects of major craniofacial deformity. Cleft Palate Craniofac J. 1992;29:578–84. [PubMed] [Google Scholar]
9. Grabber TM, Vanarsdall RL, Vig KW. 4th ed. St. Louis, MO: Elsevier Mosby; 2005. Orthodontics: Current Principals and Techniques; pp. 1097–121. [Google Scholar]
10. Osuji OO. Preparation of feeding obturators for infants with cleft lip and palate. J Clin Pediatr Dent. 1995;19:211–4. [PubMed] [Google Scholar]
11. Erkan M, Karaçay S, Atay A, Günay Y. A modified feeding plate for a newborn with cleft palate. Cleft Palate Craniofac J. 2013;50:109–12. [PubMed] [Google Scholar]
Cleft Palate Craniofac J. 2013;50:109–12. [PubMed] [Google Scholar]
12. Dar H, Winter ST, Tal Y. Families of children with cleft lips and palates: Concerns and counseling. Dev Med Child Neurol. 1974;16:513–7. [PubMed] [Google Scholar]
13. Nur RB, Germeç-Çakan D, Türkyılmaz Uyar E, Arun T. Evaluation of causes and levels of anxiety in mothers of infants with cleft lip and palate. Clin Dent Res. 2014;38:20–30. [Google Scholar]
14. Kuttenberger J, Ohmer JN, Polska E. Initial counseling for cleft lip and palate: Parents’ evaluation, needs and expectations. Int J Oral Maxillofac Surg. 2010;39:214–20. [PubMed] [Google Scholar]
15. Germeç Çakan D, Nur B, Sayınsu K, Arun T. Guidance to orthodontic clinics of infants with cleft lip and palate (Dudak Damak Yarıklı Bebeklerin Ortodonti Kliniklerine Yönlendirilmesi) 7 Tee Klinik. 2009;2:21–7. [Google Scholar]
16. Santiago PE, Barry H. Grayson role of the craniofacial orthodontist on the craniofacial and cleft lip and palate team. Semin Orthod. 2009;15:225–43. [Google Scholar]
Semin Orthod. 2009;15:225–43. [Google Scholar]
17. Canady JW, Means ME, Wayne I, Thompson SA, Richman LC. Continuity of care: University of Iowa Cleft Lip/Palate Interdisciplinary Team. Cleft Palate Craniofac J. 1997;34:443–6. [PubMed] [Google Scholar]
18. Turner L, Jacobsen C, Humenczuk M, Singhal VK, Moore D, Bell H. The effects of lactation education and a prosthetic obturator appliance on feeding efficiency in infants with cleft lip and palate. Cleft Palate Craniofac J. 2001;38:519–24. [PubMed] [Google Scholar]
19. Grayson BH, Cutting CB. Presurgical nasoalveolar orthopedic molding in primary correction of the nose, lip, and alveolus of infants born with unilateral and bilateral clefts. Cleft Palate Craniofac J. 2001;38:193–8. [PubMed] [Google Scholar]
Cleft Feeding Instructions - Seattle Children's
Why do babies with clefts have problems with feeding?
Babies with clefts have trouble with feeding because it changes how parts of the mouth are formed and how they work and fit together.
- Cleft lip makes it hard for babies to make a good seal around the nipple.
- Cleft palate makes it hard to create suction because the mouth cannot be closed off from the nose.
Normally, a baby pulls the nipple into their mouth and makes a seal with the lips around the nipple. When the baby sucks and swallows, the back of the roof of their mouth (soft palate) rises up and closes off the mouth from the nose. This creates suction and holds the breast or bottle nipple in the mouth, and the baby sucks to draw out milk.
How do I feed my baby with cleft lip?
Babies with only cleft lip can usually be fed by breast or regular bottle. Our nurses and infant-feeding specialists can help you make sure your baby gets a tight seal around the nipple.
Breast-feeding
- During breast-feeding, the soft breast tissue often will fill the opening in the lip and/or gum line. This seals off the mouth and lets your baby create enough suction.

- Sometimes it helps to hold a finger across the cleft while your baby feeds.
- Swallowing noises and normal weight gain are signs that breast-feeding is going well.
- If your baby is "noisy" with feeding, making clicking or kissing noises, they may not have enough suction.
Bottle-feeding
- If you bottle-feed your baby, feeding may work better using special bottles or nipples with a wider base.
- When starting a feeding, hold your baby in a slightly upright position.
- Touch the baby's lower lip with the nipple.
- When the baby latches on, direct the nipple slightly downwards.
- Try to keep the nipple in the center of the baby's mouth. Do not let it slip up into the cleft.
How do I feed my baby with cleft palate?
Babies with cleft palate usually need special bottles and techniques to feed well, whether or not they have cleft lip. It is rarely possible to breast-feed or use a regular bottle.
With cleft palate, a baby cannot create suction to get milk out of the breast or bottle.
A baby who is put to the breast may look like they are latching on and sucking well. But they are using up energy and getting little or no milk.
If you planned to breast-feed, we encourage you to express your milk and feed your baby using a special bottle.
Breast milk is considered the most ideal food for all babies. There are added benefits for babies with cleft palate, such as fewer middle ear infections.
Often, mothers who were looking forward to breast-feeding feel great sadness at the loss of this experience. We encourage you to acknowledge this loss and seek support. We can help with feeding techniques to help you maintain closeness with your baby.
What kind of bottle should I use for feeding with cleft palate?
There are 4 types of bottles for feeding babies with clefts:
- Cleft Lip/Palate Nurser by Mead Johnson
- SpecialNeeds Feeder by Medela
- Pigeon feeder with one-way valve
- Dr. Brown’s Specialty Feeding System with one-way valve
The Pigeon nipple with one-way valve can be used with any bottle.
The Cleft Palate Foundation website has a video on feeding your baby and information on how to order supplies online.
Cleft Lip/Palate Nurser by Mead Johnson
Cleft Lip/Palate Nurser
by Mead Johnson
The Cleft Lip/Palate Nurser by Mead Johnson is a low-cost, soft, squeezable bottle.
We suggest that you replace the long yellow nipple that comes with the bottle. Use any shorter, softer nipple.
- Before using the bottle for the first time, put some water in it and practice squeezing the liquid out of the nipple. This will help you get a feel for how firmly you need to squeeze.
- When you squeeze the bottle, the liquid should flow easily but not too fast.
- As your baby begins to suck, squeeze the bottle with a firm, steady pressure to the count of "squ-e-e-ze-2, 3." Relax your squeeze on the 2, 3 count. This pauses the flow of milk.
- You should only squeeze when your baby is sucking. Watch your baby closely and listen for swallowing sounds.
- If your baby pauses to breathe, you should pause also. If your baby is getting milk out of the bottle, you should see air bubbles in the milk.
- If you forget to stop squeezing the bottle when your baby pauses, your baby may cough and sputter. Just take the nipple out of the baby's mouth for a moment and let them settle. Then continue feeding.
If sputtering happens throughout the feeding, call the Craniofacial team for advice: 206-987-2208. Most parents quickly learn to adjust squeezing to their baby's sucking rhythm.
SpecialNeeds Feeder
SpecialNeeds Feeder
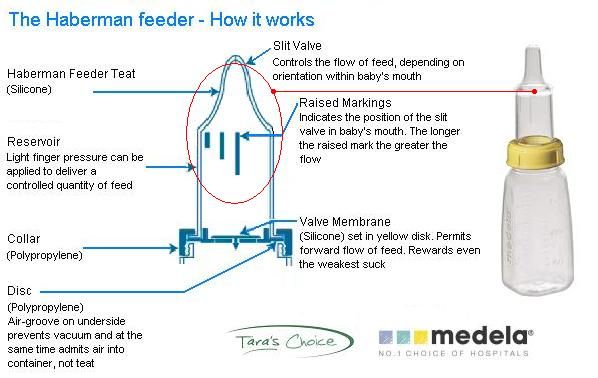
The SpecialNeeds Feeder by Medela has a one-way valve that keeps milk in the nipple. It does not require suction.
This bottle used to be called the Haberman feeder.
Sometimes babies can get milk from this feeder themselves by pushing the nipple against their gum line. The nipple is soft-sided. For many babies, it works best for the parent to squeeze the bottle to match their baby’s rhythm of sucking and swallowing (as described earlier for the Mead Johnson nurser).
There is a “Y” cut in the nipple. Turning the nipple in the baby’s mouth changes the orientation of the “Y” cut in the baby’s mouth. This varies the rate of flow. The nipple has 3 lines that indicate which flow rate is in effect.
Dr. Brown’s Specialty Feeding System with one-way valve
Dr. Brown’s Specialty
Feeding System
You can buy Dr. Brown’s Specialty Feeding System with one-way valve through Amazon. The Dr. Brown’s bottles sold in stores do not have the one-way valve.
Dr. Brown’s Specialty Feeding System uses a bottle with a one-way valve at the base of the nipple to keep the nipple full of milk. It does not require suction.
- When the baby bites or compresses the nipple, milk flows into their mouth and not back into the bottle.
- The one-way valve ensures that there is always milk in the nipple.
- The baby controls the rate of the feeding.
Pigeon feeder
Pigeon nipple with one-way valve
The Pigeon feeder has a nipple with a one-way valve. The nipple can be used with any bottle.
The nipple can be used with any bottle.
The nipple comes in 2 sizes. The smaller size has a slower flow. It is best for newborns.
The larger, faster-flowing nipple works well for babies 6 weeks and older.
The Pigeon nipple with one-way valve works by compression only. No squeezing is needed.
- A plastic one-way valve that fits into the nipple keeps milk in the nipple. Place the valve with the flat side toward the tip of the nipple.
- When your baby begins to suck, milk flows easily. Your baby controls the flow of milk.
- The nipple has a firm side that goes against your baby’s gum line and a softer side that goes on their tongue.
- A small notch near the rim of the nipple serves as an air vent. This notch should be under your baby's nose when feeding. This puts the nipple correctly in your baby’s mouth.
- Tightening the nipple slows the flow of milk. Loosening it makes the flow faster.
- If the nipple collapses, loosen and retighten it.

The Cleft Palate Foundation website has information on how to order these supplies online.
How do I care for the bottles and nipples?
All of these bottles and nipples can be hand washed in hot soapy water. Rinse and allow to air dry.
Do not boil the bottles or parts. Do not wash them in the dishwasher or put them in a microwave. They may soften and start to leak.
How do I express breast milk for my baby?
If you want to express breast milk for your baby, we recommend a hospital-grade electric breast pump with a double pumping system.
Birth hospitals have pumps for mothers to use in the hospital. You can rent or buy a breast pump for use at home. Insurance can cover rental or purchase of a breast pump for a baby with a cleft palate.
At first, pump at least 8 times in 24 hours, including at least once during the night. After several weeks of frequent pumping, most mothers make enough milk by pumping about 6 times a day. Tips for pumping breast milk (PDF).
How much should my baby eat?
Newborn babies begin with frequent feedings of very small amounts of milk (1 ounce or less). Over time, they increase the amount they can take.
By 2 weeks of age, a baby needs at least 2 to 2.5 ounces of milk per pound of weight each day. For example, a 3-week old baby who weighs 9 pounds should have at least 18 to 22.5 ounces of breast milk or formula in 24 hours.
A feeding session should take no longer than 30 minutes. If it takes longer, your baby is working too hard and burning calories needed for growth.
We recommend weighing babies weekly until they show a normal rate of growth. Usually this happens in 4 to 6 weeks.
How often does my baby need to eat?
During the first month of life, a baby will feed 8 to 12 times per day — every 2 to 3 hours. A baby this young usually feeds at least 2 times during the night.
At 2 to 4 months, a baby will feed 6 to 8 times per day — every 3 to 4 hours.
How will I know if my baby is gaining enough weight?
A baby usually loses weight the first week of life. The loss is usually 5% to 10% of their body weight. Your baby should regain this weight by 2 weeks old.
The loss is usually 5% to 10% of their body weight. Your baby should regain this weight by 2 weeks old.
At first, we expect your baby to gain 5 to 7 ounces per week. At 4 to 6 months old, the rate of weight gain slows. Your baby should gain about 3.5 to 4.5 ounces per week.
What if my baby is not gaining enough weight?
Sometimes babies with cleft lip and palate have difficulties taking enough breast milk or formula to grow.
Ask your medical team for advice. They can give you an approved recipe for adding formula powder to breast milk or regular formula. This gives your baby extra calories, protein and vitamins. Talk to your healthcare team before doing this.
What about starting solid foods?
Babies with clefts can start solid foods at the same age as other babies. Most often, this is at 4 to 6 months.
Experiment to find the right consistency for solids. It needs to be just right so your baby can eat without the food coming out their nose. This is not harmful to your baby. Sneezing will usually clear the food out of the nose. Most babies learn quickly to get the food down their throats rather than out their noses.
Sneezing will usually clear the food out of the nose. Most babies learn quickly to get the food down their throats rather than out their noses.
Can my baby drink from a cup?
Cup feeding can also be started at the usual age, 8 to 12 months. Cups with plain lids can help limit spills. Do not use spill-proof cups with valves. These require that baby create suction to get any fluid.
See the Cleft Palate Foundation website for a video on feeding your baby and information on how to order supplies online.
Crockery
JavaScript seems to be disabled in your browser.
You must have JavaScript enabled in your browser to utilize the functionality of this website.
NUK. Understanding life.
Shop By
- Farbe
- Blue (1)
- Yellow (2)
- Sea wave (2)
- Purple (2)
- Pistachio (2)
- Alter
- 6-18 months (4)
- 18+ months (2)
- Collection
- Winnie the Pooh (2)
From about 6 months of age, the child's physical condition allows him to eat and drink on his own. In order to teach children to drink and eat "like adults", NUK has developed a special series of products. All items designed for this series "grow" and develop with the baby. They are suitable for various types of food and correspond to the phases of a child's natural development, making the transition from liquid to solid food not so difficult.
In order to teach children to drink and eat "like adults", NUK has developed a special series of products. All items designed for this series "grow" and develop with the baby. They are suitable for various types of food and correspond to the phases of a child's natural development, making the transition from liquid to solid food not so difficult.
4 pcs.
Display
twenty 25 thirty 35 40 All
On the page
Select by
Name
-
- To learn more
- To learn more
- To learn more
- To learn more
Feeding children with cleft lip or palate
Cleft palate makes it difficult (and often impossible) to create a vacuum because the oral cavity is not isolated from the nasal cavity.
Feeding a child with cleft palate in the first hours and days after birth requires particularly prompt and clear advice from a lactation consultant. After all, parents are usually too upset and confused. They find it difficult to even formulate questions.
As with any baby, the best practice is to:
1. create all conditions for feeding the baby, in any way
2. improve milk production
fully appreciate the features of suckling
In the first hours and days, the volume of colostrum is too small to be poured into a bottle. The small volume and viscous consistency of colostrum have their advantages. Spoon or syringe feeding is a good place to start. The likelihood that the child will choke is extremely small.
- Teach mom how to feed upright or face down.
- Finger feeding with a syringe in some cases allows you to block the hole in the palate with the pad of your finger and in all cases stimulate sucking movements.

- When the volume of milk per feeding exceeds 30 ml, and the consultant or mother has studied the characteristics of the baby's sucking enough, you can choose the right device for feeding.
Children with clefts usually need special bottles and methods to feed properly. Rarely is it possible not only to breastfeed, but also to use a regular bottle.
Today there are several options for feeding devices for babies with clefts:
(Special Needs)
The long nipple has a voluminous base. During feeding, the soft silicone base is squeezed with fingers to ensure milk flows into the baby's mouth. You can adjust the strength of the flow and the volume of milk flow by turning the bowl according to the divisions on the base. Available for order in many online stores in Russia, the price is about 2000 rubles.
2. "Dr.Brown's Natural Flow® Special Feeding Bottle with Valve". Dr. Brown's standard anti-colic bottle with nipple has a special membrane check valve that allows milk to move only towards the mouth and does not allow it to return to the bottle. With this system, the baby can compress the teat with their gums, adjusting the flow. Available for order in many online stores in Russia, the price is about 800 rubles.
3. " Pigeon teat, with valve for feeding babies with cleft palate and/or lips" . Available in two sizes, for newborns and standard. Made of silicone, the sides are of different thicknesses: the softer side lies on the tongue, the harder one is turned towards the palate. Thus, the cleft in the palate is closed, and the child has the opportunity to squeeze out the milk with the movements of the tongue. Suitable for all bottles with a standard neck. According to parents, these nipples wear out quickly, one is enough for 3-4 weeks. Available for order in many online stores in Russia, the price is about 350 rubles.
4. " Mead Johnson Cleft Cup" . Long nipple, flat bottle, soft enough to squeeze while nursing. Experts recommend trying to change the long yellow pacifier to a regular one if the baby is choking. It is not sold in Russia, but can be ordered on foreign websites.
5. " Nuk Teat for children with cleft palate ". A rather large soft latex nipple designed to cover a cleft palate to help create a sucking vacuum. Initially sold without a hole, which parents are encouraged to do themselves on the recommendation of a doctor, depending on the type of cleft. Suitable for all standard bottles. Nipples wear out quickly, one is enough for 3-4 weeks. Available for order in some online stores, the price is about 700 rubles.
Feeding tips for babies with special needs :
- Like any feeding device, a cup or pacifier should be carefully selected according to its characteristics and the special needs of the child.

- Before the first feeding, fill the bottle with some water and practice squeezing the liquid out of the nipple. This will help to feel the features of the flow and, if necessary, calculate the compression force.
- Fluid should flow easily, but not too fast.
- As soon as the baby begins to suckle. At the expense of “ra-a-a-a-az”, smoothly squeeze the bottle / nipple, with firm, steady pressure. At the expense of "2, 3" smoothly release.
- Squeeze only when the baby suckles. Watch your baby carefully and listen for the sounds of sips.
- If the baby stops to breathe, you should also pause.
- Most parents quickly learn to adjust to their baby's suckling rhythm.
Should I breastfeed a baby with a cleft?
Yes, it is worth doing: although sucking is unlikely to be effective due to the lack of vacuum, there are no obstacles to the actual attachment, but there are significant advantages.
- Even non-nourishing suckling stimulates the mother's oxytocin reflex, increases milk production, and facilitates pumping.
- A mother's feelings of grief and disappointment will be significantly reduced if she can soothe her baby at the breast, hold him "skin to skin" and act within the normal scenario of mother-newborn interaction.
- With a cleft lip, it is sometimes possible to establish full breastfeeding: if the mother has the opportunity to cover the cleft during attachment to the breast (for example, with a finger), in some cases this allows the baby to create a vacuum that is quite sufficient for effective sucking. It's not always enough, but it's definitely worth a try.
- The mother and counselor will have the opportunity to observe the baby's sucking patterns from all angles. This will help develop the best feeding strategy and select the most suitable devices.
- There is evidence of additional benefits of breastfeeding for children with clefts, such as a reduced risk of middle ear infections.