Feeding your premature baby
Caring for a Premature Baby: Feeding
How often should I feed my baby?
Feeding patterns differ between babies and vary from day to day. Before discharge from your NICU (Newborn Intensive Care Unit), the nurses can give you an idea of your baby's feeding pattern. Most preemies feed every 2 1/2 - 4 hours. Look for cues that your baby is hungry. Premature babies do not always cry, but may move around and become restless if it has been 2-3 hours since they last ate. Often the doctor will want you to awaken your baby if it has been longer than 4 or 5 hours since the last feed. Discuss this with your doctor.
How much should I feed my baby?
A baby who weighs about 4 1/2 lbs. usually needs 12-15 ounces of formula or milk per day. A good way to see if your baby is getting enough to eat is to observe how many wet diapers he/she has in a 24 hour period. Your baby should have 6-8 wet diapers every day. Most formula fed baby's will be taking 2-3 ounces every 3-4 hours when discharged from the hospital. If your baby is finishing the feeding in a shorter time and still acting hungry offer an extra ounce or two. A breast feeding baby will usually increase its feeding time by sucking longer or wanting to eat more often. This builds up the mothers milk supply. Sometimes this means that your baby will want to eat every 2 hours until your supply will meet his/her demands. Your doctor will check your baby's weight at each visit and let you know if the weight gain is appropriate.
When will my baby gain weight?
Almost all babies lose weight before they begin to gain weight. This weight loss typically is 5-15% of the baby's birth weight. Much of the weight loss is loss of water because the baby is no longer surrounded by fluid. Sometimes very sick babies gain weight the first few days. This is not real weight gain; it is retention of water. As the baby's condition improves, the baby will lose weight. Usually a baby does not regain his/her birth weight until two or more weeks of age.
Our baby will be getting formula, what should we know about it?
There are three forms of formula: powdered, concentrate, and ready to feed. The nutritional content of the three preparations of formula are the same. Most formula found in stores has 20 calories per ounce. Your doctor will want you to use 20 calorie, unless she/he has specifically told you to use a higher calorie. It is very important to use only what the doctor has ordered. Higher calorie formulas containing 24 or 27 calories per ounce, need to be ordered and can be very expensive. Here are recipes for mixing formula from powder or concentrate.
Powdered formula
- least expensive to buy.
- try using warm water and mixing it in a blender to help dissolve formula.
- with measuring scoop in the can:
- to make 20-calorie-per-ounce formula: 1 scoop powder + 2 ounces of water.
- to make 24-calorie-per-ounce formula: 3 scoops powder + 5 ounces of water
- once the can is opened the powder must be used within 1 month.
Concentrated formula
- most convenient to use.
- to make 20-calorie-per-ounce formula: 1 ounce concentrate + 1 ounce water.
- to make 24-calorie-per-ounce formula: 3 ounces concentrate + 2 ounces water.
- to make 27-calorie-per-ounce formula: 13 1/2 ounces concentrate + 6 1/2 ounces of water.
- should be sealed and kept in the refrigerator, once the can is opened.
- should be used within 48 hours.
Never add more water than what is called for in the preparation. Follow the directions correctly.
How do I take care of the bottles and other equipment when using formula?
Bottles, nipples, measuring cups, containers, brushes and any other equipment used for feeding should be washed in hot, soapy water and then rinsed in hot, running water. Glass or metal pieces can be washed in the dishwasher.
Should I plan to breast or bottle feed my baby?
Just because your baby is premature does not mean s/he must have formula. In fact, there are many advantages to mother's breast milk over formula. These advantages include:
In fact, there are many advantages to mother's breast milk over formula. These advantages include:
- Fewer infections
- Less risk for Necrotizing Enterocolitis (NEC)
- Better tolerance of feeds
- Less risk of allergy
- Enhanced development
Early breast milk, called colostrum, is especially rich in antibodies and cells that help fight infection. Babies who are too young to suckle at the breast can get your milk in their tube feedings. Even if you planned to bottle feed or cannot breast feed long term, you might consider providing breast milk for your preemie while s/he is in the hospital. It is something special that only you can do for your baby.
I can't or don't wish to breast feed. Will I be hurting my baby?
Babies can and do develop normally when fed only formula. Although encouraged, breast feeding is a personal choice. You and your baby can still benefit from close skin to skin contact.
When can my baby nipple or breast feed?
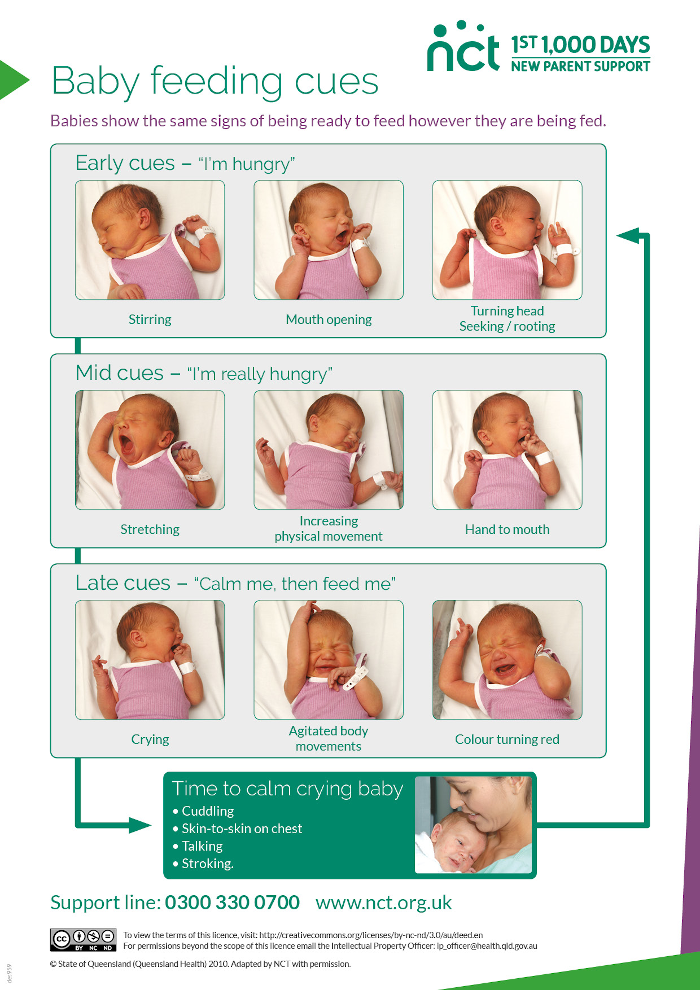
When babies are born prematurely their sucking is not well coordinated with their breathing. This suck-swallow-breathe pattern usually becomes coordinated enough to safely breast or bottle feed at about 34 weeks of gestation. However, there are big differences among babies. Some are ready at 32 weeks; others are not ready at 36 weeks. Nurses can often tell when a baby is getting close to this time by how a baby acts during a tube feeding. Your baby's doctors and nurses will determine when to start. At first your baby will have only one or two feeds a day that are not by tube. This will gradually increase as the baby gets used to the extra work of feeding. Because nipple and breast feeding requires more work, babies who have had severe respiratory problems may be slower to start and slower to advance on feedings. Before your baby is ready to feed by breast or bottle, s/he may enjoy sucking. A pacifier may be used to encourage sucking. When the baby is being tube fed, s/he may like to suck on a pacifier or the breast that is empty of milk. This is called non-nutritive sucking. Sucking on the empty breast or nuzzling the breast during tube feeding can be combined with kangaroo care.
This suck-swallow-breathe pattern usually becomes coordinated enough to safely breast or bottle feed at about 34 weeks of gestation. However, there are big differences among babies. Some are ready at 32 weeks; others are not ready at 36 weeks. Nurses can often tell when a baby is getting close to this time by how a baby acts during a tube feeding. Your baby's doctors and nurses will determine when to start. At first your baby will have only one or two feeds a day that are not by tube. This will gradually increase as the baby gets used to the extra work of feeding. Because nipple and breast feeding requires more work, babies who have had severe respiratory problems may be slower to start and slower to advance on feedings. Before your baby is ready to feed by breast or bottle, s/he may enjoy sucking. A pacifier may be used to encourage sucking. When the baby is being tube fed, s/he may like to suck on a pacifier or the breast that is empty of milk. This is called non-nutritive sucking. Sucking on the empty breast or nuzzling the breast during tube feeding can be combined with kangaroo care. This helps the mother with milk production and readies the baby for future breast feeding. In addition, babies stay warm while held.
This helps the mother with milk production and readies the baby for future breast feeding. In addition, babies stay warm while held.
Will my baby be able to nurse even though he/she has been taking the bottle at the hospital?
Most nurseries encourage the mothers to pump their breasts while their baby is in the hospital. The nurses will work with you and your baby once your baby is able to begin the process of sucking, swallowing and breathing.
Premature babies may take days or weeks to learn how to nurse. It is important to remember to be patient and try not to become discouraged if you have chosen to breast feed. There are times when this transition is not entirely successful; it is important to not feel guilty.
How will my body know to produce milk early?
After delivery, hormones change rapidly, signaling to your breast to begin making milk. With stimulation by the baby's sucking (or by the breast pump) the breasts will continue to make milk. The more stimulation the more milk the breasts make.
When should I start pumping?
It is best to start as soon after delivery as you can, within the first 6 hours is best, but definitely within the first 24 hours. Early pumping is very important for establishing a milk supply. Even if your baby is very sick and not being fed, you need to pump your breast regularly so there will be milk when your baby is ready. Electric breast pumps are the best. Ask your nurse or a lactation consultant for assistance in learning to use one and in preparing to rent one when you are out of the hospital.
How often should I pump?
You should pump at least five times a day and for a total time of at least 100 minutes a day. Ideally increase this to 8 to 12 times a day for 10 minutes per side. Frequent pumping signals your body to keep making milk. At first you may get very little milk, sometimes just a few drops. But, it is important to save all that you get of this early milk for your baby. About the third day your breasts will become full and swollen. This is your milk coming in. At this time your milk supply will increase. With frequent pumping you will produce more than your baby can use, but don't decrease the amount of pumping. It is important to build a good supply early.
This is your milk coming in. At this time your milk supply will increase. With frequent pumping you will produce more than your baby can use, but don't decrease the amount of pumping. It is important to build a good supply early.
My baby is sick and not eating. What do I do with my milk?
Pumped milk can be frozen for later use. Unless told otherwise, the milk from an entire pumping should be pooled and then divided into containers for freezing. The nutrients of milk are not changed by freezing, but frozen milk does not protect against infection. Your baby's doctor may want to use fresh milk when the baby starts to feed. Fresh milk is milk that has not been frozen, but it can be refrigerated for 24-48 hours. Ask you baby's nurse about the guidelines for your nursery.
Will my milk provide my baby with all the things that s/he needs to grow?
Milk from mothers who deliver early is different from milk from mothers who deliver on time. It has more protein, sodium, calcium and some other nutrients. Even so, it not as rich in some of these things as what the baby would receive from the placenta if s/he were not born early. Some preemies grow well on their mother's milk alone. Others, especially very small or sick preemies, cannot handle the amount of milk that it would take to get all the calories and nutrients that they need. The same is true of formula - preemie formulas are richer in these things than regular formulas. Your baby's doctor may decide to enrich your milk to provide your baby with more calories and/or minerals. There are many ways to do this:
Even so, it not as rich in some of these things as what the baby would receive from the placenta if s/he were not born early. Some preemies grow well on their mother's milk alone. Others, especially very small or sick preemies, cannot handle the amount of milk that it would take to get all the calories and nutrients that they need. The same is true of formula - preemie formulas are richer in these things than regular formulas. Your baby's doctor may decide to enrich your milk to provide your baby with more calories and/or minerals. There are many ways to do this:
- Adding specific nutrients to the milk such as fat, protein or sugars.
- Mixing your milk with preemie formula. This is common if your baby needs more milk than you can currently supply.
- Human milk fortifiers. These are powders or liquids added to your milk before it is given to the baby.
- Giving more "hind" milk to the baby. This is the last portion of milk pumped from the breast.
 It is richest in fat and calories.
It is richest in fat and calories.
As the baby gets older and no longer needs to be tube fed, his/her need for extra nutrients and calories also decreases. So, by the time the baby can completely breast feed, usually breast milk supplies all the calories that s/he needs. Your baby may still need additional vitamins and iron
Tips for Feeding Premature Babies – Children’s Health
Share:
When babies are born prematurely (before 37 weeks of pregnancy), they may have special feeding and nutritional needs. Preemies often need extra support to grow and continue developing, and parents may have questions about breastfeeding, bottles or feeding schedules.
Kikelomo Babata, M.D., a neonatologist at Children's Health℠ and Assistant Professor at UT Southwestern, answers these questions and shares advice for feeding your premature baby.
What are common feeding problems in premature infants?
Premature babies may face different feeding problems depending on their age and development.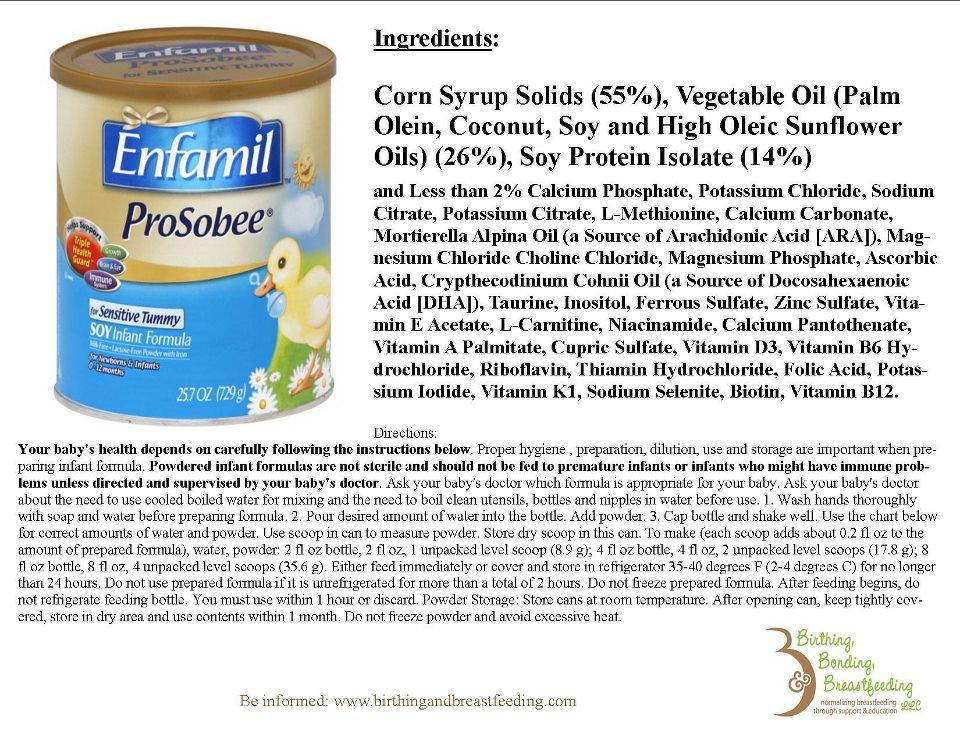 "Post-conceptual age is more important than chronological age for a baby's development," explains Dr. Babata. "A 4-week-old infant born at 32 weeks may not be as developmentally ready to feed as a 2-week-old infant born at 35 weeks. And every baby is different."
"Post-conceptual age is more important than chronological age for a baby's development," explains Dr. Babata. "A 4-week-old infant born at 32 weeks may not be as developmentally ready to feed as a 2-week-old infant born at 35 weeks. And every baby is different."
Some premature babies have difficulty breastfeeding or bottle-feeding for the first few weeks of their lives. This is because infants, both full-term and premature, continue developing their ability to suck, swallow and breathe after birth. This is a skill they need to feed, so they can coordinate how to suck, swallow then breathe through their nose. Additionally, premature babies may be sleepy and get tired during their feeds.
Premature infants might also have underdeveloped lungs. They might need to be on oxygen, which can make it difficult for them to eat.
Other common feeding problems in premature babies can include:
- Apnea (episodes where they stop breathing)
- Episodes of bradycardia (slow heartbeat that can cause oxygen levels to drop)
- Immature feeding pattern (sucking, swallowing and breathing incorrectly or out of order)
- Oral aversion (not taking a bottle or breast)
- Risk of aspiration (breathing in milk or formula)
If your baby experiences these feeding problems, they may need to be fed through a feeding tube. This tube is placed through the nose and down into the esophagus. If your baby has a feeding tube, they'll stay in the hospital until it is removed.
This tube is placed through the nose and down into the esophagus. If your baby has a feeding tube, they'll stay in the hospital until it is removed.
Once your baby goes home, your pediatrician can offer tips on feeding your baby and the importance of good nutrition. If needed, they can refer you to speech therapist for more support.
Can I breastfeed my premature baby?
Yes, you can breastfeed a premature baby. Your breastfeeding experience may depend on your baby's development and nutritional needs.
Breastmilk offers many benefits for premature babies, such as:
- Boosting digestion
- Helping baby’s immune system fight infection
- Promoting eye and brain development
- Providing bonding opportunities
"Breastmilk is linked to a lower risk of necrotizing enterocolitis, an illness that can be devastating for preterm infants," says Dr. Babata. Necrotizing enterocolitis is inflammation that can seriously damage or destroy intestinal tissue in babies. It can increase their risk of death or neurodevelopmental problems.
It can increase their risk of death or neurodevelopmental problems.
Breastfed infants also have a lower risk of ear infections, respiratory infections like respiratory syncytial virus (RSV) and bronchiolitis, rashes and gastroenteritis. Breastfeeding can have long-lasting benefits as well – lowering your child's risk for chronic illnesses in the future.
Advice for breastfeeding a premature baby
It's important to know that breastfeeding a premature infant might look different than breastfeeding a full-term infant. Breastfeeding may take more coordination for a preemie than bottle feeding, and depending on how premature your baby is, they may have difficulty latching. You may need to use bottles for a few weeks if your baby is having difficulty nursing. You can still choose to pump and provide breastmilk in a bottle. See tips for increasing your milk supply while pumping and how to safely store your breast milk.
If your premature baby can breastfeed, they still might need bottles of supplemental formula. Often, premature babies cannot exclusively breastfeed because they have higher caloric needs to support growth. Special high-calorie formula or human milk fortifiers can help your child grow while still getting the benefits of breastmilk.
Often, premature babies cannot exclusively breastfeed because they have higher caloric needs to support growth. Special high-calorie formula or human milk fortifiers can help your child grow while still getting the benefits of breastmilk.
If your premature baby is on a feeding tube, talk to your care team to learn what you can do and whether you should pump your breastmilk.
What type of bottle and formula is best for my premature infant?
Whether you give breastmilk or formula in a bottle, you should use a slow flow bottle nipple designed for premature infants. These bottle nipples help prevent your baby from getting more liquid than they can handle at once.
Most premature babies will use a special formula designed for preterm babies. Your pediatrician or neonatologist can recommend the right formula for your baby's needs. Depending on your baby's diet, they can also advise if any other nutritional supplements are needed, such as vitamin D or iron.
How much should I feed my premature baby and how often?
How much your baby needs to eat will change as they grow. Premature babies need 150 to 160 milliliters per kilogram of body weight each day. Your lactation consultant or pediatrician can help you determine how much this is for your baby.
No matter how much they eat per feeding, preemies need to eat at least every 3 to 4 hours.
When can my premature baby eat solids?
A premature baby can start eating solid foods when their adjusted or conceptual age is 4 to 6 months. A conceptual or adjusted age means that instead of counting your baby’s age from their date of birth, it's calculated from their due date. For instance, if your baby is born 10 weeks before their due date, their age at 10 weeks past their due date is 10 weeks (even though they were born 20 weeks ago).
Around the adjusted age of 4 to 6 months, premature babies should be able to support their head and have lost their tongue-thrust reflex. This reflex causes them to spit out anything put in their mouth that's not milk or formula. This is a good time to introduce solids.
This reflex causes them to spit out anything put in their mouth that's not milk or formula. This is a good time to introduce solids.
Taking care of a baby is a challenging job. While these special feeding needs can add extra stress to those early days of your child's life, parents should remember that patience is key.
"Most babies will eventually learn to feed orally," says Dr. Babata. "Just take it one step at a time and be sure to notice and enjoy progress as it occurs."
Learn more
With the only nationally ranked Level IV NICU in North Texas, Children's Health provides expert multidisciplinary care for a wide variety of complex neonatal conditions. Learn more about our top-ranking Neonatology program.
Thank you!
You are now subscribed to the Children's Health Family Newsletter.
Children's Health will not sell, share or rent your information to third parties. Please read our privacy policy.
Children's Health Family Newsletter
Get health tips and parenting advice from Children's Health experts sent straight to your inbox twice a month.
Please enter a valid email address
Feeding premature babies | Breastfeeding premature babies
Premature babies have a special need for breast milk, but it can be difficult to breastfeed them directly. Our expert advice will help you provide your premature baby with healthy breast milk.
Share this information
Professor Katsumi Mizuno, Department of Pediatrics, Showa University Koto Toyosu Hospital:
Katsumi is a Certified Breastfeeding Consultant, Professor of Pediatrics at Showa Medical University, and one of Japan's leading pediatric neonatologists. His research focuses on neonatal suckling skills, breast milk banking, and the use of breast milk for feeding premature babies in neonatal intensive care units.
Babies born before the 37th week of pregnancy are considered premature. 1 The causes of preterm birth are not always obvious, but certain factors increase the likelihood of such an event. These include: twin or multiple pregnancy, certain diseases of the mother or fetus, as well as a history of premature birth.
Because premature babies spend less time in the womb, they are not mature enough and may be more susceptible to infection and disease. They often require hospitalization in the neonatal intensive care unit.
Why is breast milk so important for premature babies?
Breast milk is essential for optimal growth and development of term babies, but it is even more important for premature babies.
During pregnancy, the fetus receives important substances from the mother through the placenta, such as DHA (a fatty acid essential for brain and eye development) and immunoglobulin G (an antibody). 2.3 A premature infant did not receive all of these substances. However, the milk produced by a premature mother contains more fat and secretory immunoglobulin than mothers of full-term babies. 4
However, the milk produced by a premature mother contains more fat and secretory immunoglobulin than mothers of full-term babies. 4
In addition, premature babies have an underdeveloped gastrointestinal tract, which can make digestion and absorption of nutrients difficult, so they need food that their sensitive stomach and intestines can easily digest. Breast milk contains enzymes that make it easier for the baby to digest, 5 as well as epidermal growth factor, which accelerates the development of the gastrointestinal tract 6 . Premature infants who are predominantly breastfed have much lower intestinal permeability than formula-fed infants, meaning fewer potentially harmful particles from the stomach and intestines enter their bloodstream. 7
Breast milk is so important for premature babies that if the baby's mother does not produce enough breast milk at first for any reason, it is recommended that the deficiency be replenished with donor milk rather than formula.
Does breast milk improve the condition of premature babies?
Breast milk contains protective substances that can prevent serious diseases that preterm infants are susceptible to, 8 such as severe infections, 9 retinopathy of prematurity (which can cause vision loss) 10 and bronchopulmonary dysplasia (chronic lung disease). 11
The more milk your baby gets, the lower the risk of developing diseases. 12 Every additional 10 ml of milk per kilogram of body weight per day reduces the risk of sepsis by 19%. 9 The risk of developing necrotizing enterocolitis (a potentially fatal bowel disease) in premature infants who are breastfed is ten times lower than those who are formula fed. 13 That's why every drop counts!
Most importantly, premature infants who are breastfed are typically discharged an average of two weeks earlier than formula-fed infants. 14 They also have a 6% lower risk of readmission in the first year of life. 15
15
Breast milk has been proven to have a beneficial effect on mental and physical development in the long term. Studies show that low-birth-weight babies who are breastfed in the neonatal intensive care unit have an average IQ of up to five points higher than those who are not breastfed. 15 In addition, their cardiovascular system works better during their lifetime. 17
Will milk be produced if the baby is born prematurely?
Yes, the mother's body is ready to produce milk by the middle of pregnancy. After the baby is born and the placenta is born, the level of progesterone, the pregnancy hormone, drops, and the production of colostrum, the first milk, starts in the breast. This usually happens after the newborn is put to the breast and begins to suckle rhythmically, but if the baby was born prematurely, he most likely will not be able to latch on at first.
To replicate the sensations that trigger milk production, you can manually stimulate the breasts and nipples, or use a breast pump to express nutrient-rich colostrum for your baby. 18 Read below for more information on what to do if your premature baby is not yet able to breastfeed.
18 Read below for more information on what to do if your premature baby is not yet able to breastfeed.
Breast milk usually comes in two to four days after birth, but if it was premature, the milk supply may be delayed. However, a recent study shows that moms who started pumping within one hour of giving birth had milk coming in as expected. 19 This is why it is important to start expressing breast milk as early as possible.
How to prepare if the baby is expected prematurely?
Visit the neonatal intensive care unit to see how it works and how premature babies are cared for. In addition, it will be useful to learn how breast milk is produced and secreted and why it is not only a healthy food, but also an important medicine for premature babies. Read more about this in our free e-book Surprising Breast Milk Facts .
What if a premature baby cannot breastfeed?
Many babies born before 34 weeks have difficulty coordinating sucking, swallowing and breathing. Until the baby masters these skills, nurses will feed him through a tube that is inserted into the nose or mouth and provides food directly into the stomach. In this way, the baby can be fed continuously until he is ready to breastfeed.
Until the baby masters these skills, nurses will feed him through a tube that is inserted into the nose or mouth and provides food directly into the stomach. In this way, the baby can be fed continuously until he is ready to breastfeed.
If your baby is too weak to latch on and suckle milk, you can use a breast pump* available at the hospital or maternity hospital to “do the job for the baby”. Breast stimulation with research-based technology, 20 mimics the rhythm of the baby's suckling, plays an important role in starting and maintaining milk production in the first hours after birth 21 .
Milk should be expressed at the same frequency as term infants are usually fed every two to three hours, i.e. 8 to 12 times a day.
You can try putting a small amount of expressed breast milk into the baby's mouth with a syringe, or putting milk-soaked cotton swabs in the baby's mouth. 22 This is how your baby learns the taste of your milk, which will facilitate the transition to breastfeeding in the future. In addition, the protective substances that make up breast milk will help strengthen the local immunity of the baby's oral cavity. You can be involved in the care of your premature baby in a variety of ways - check with your healthcare provider for details.
In addition, the protective substances that make up breast milk will help strengthen the local immunity of the baby's oral cavity. You can be involved in the care of your premature baby in a variety of ways - check with your healthcare provider for details.
Very low birth weight babies - less than 1.5 kg - usually need extra protein, calcium and phosphorus, so they are given fortified breast milk. In some countries, such additives are made on human milk, and, for example, in Japan, on cow's milk.
Recommendations for pumping milk
If the baby will be in the neonatal intensive care unit for a long time, neonatologists recommend using a double breast pump for pumping. I always recommend Medela Symphony*. Double pumping not only speeds up the process, but also produces an average of 18% more milk than pumping from each breast in turn. 23
In addition, I advise you to create the most comfortable conditions for pumping. It is generally agreed that it is best to express milk during or after prolonged skin-to-skin contact with the baby (more on this "kangaroo method" below). Another good option is to sit next to the crib and watch your baby while he pumps. Oxytocin (the hormone that stimulates milk flow) is released when you look at your baby, touch him, smell him and think about him, 24 Therefore, comfortable and calm conditions must be created for this in the neonatal intensive care unit.
Another good option is to sit next to the crib and watch your baby while he pumps. Oxytocin (the hormone that stimulates milk flow) is released when you look at your baby, touch him, smell him and think about him, 24 Therefore, comfortable and calm conditions must be created for this in the neonatal intensive care unit.
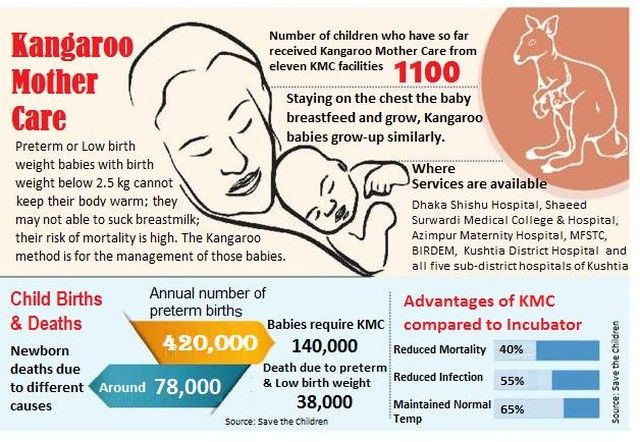
What is kangaroo care for premature babies?
The so-called kangaroo method involves prolonged skin-to-skin contact between parents and infant. This is extremely beneficial for you and your baby, as well as for milk production. Skin-to-skin contact normalizes the baby's breathing and heartbeat, keeps him warm and allows him to be as close to the parent as possible. Kangaroo care is believed to have a beneficial effect on the health of premature babies, 25 and it helps mothers express more milk 26 and breastfeed longer. 27 Skin-to-skin contact 30-60 minutes before feeding gives baby time to wake up and be hungry so he can eat without being forced.
What if the neonatal intensive care unit offers formula feeding?
Feel free to state that you want to breastfeed your baby instead of formula. If you don't have enough breast milk to feed your baby, ask the ward for help to increase your milk supply.
It is natural for mothers whose babies are in the neonatal intensive care unit to experience anxiety and stress. Sometimes these experiences interfere with milk production, so it's important to ask for any help you may need. Remember that you have the right to seek support. Your healthcare provider may be able to recommend a suitable lactation specialist, such as a lactation consultant, for you.
How to switch from pumping to breastfeeding?
At whatever gestational age a baby is born, if the baby is stable enough for skin-to-skin contact, it can seek the breast for sedative suckling. This is the perfect way for your baby to learn sucking skills before they learn to coordinate sucking, swallowing and breathing.
Babies love the smell of breastmilk, so you can put some milk on the nipple before putting your baby to the breast to make him want to suckle. He might even be able to suck some milk. Don't worry if your baby seems to suck very little - he learns every time. He can start with one or two sips and gradually move on to full breastfeeding. Until then, the baby can be fed through a tube, pressed to the breast, so that the taste of milk and touching the breast is associated with a feeling of satiety.
You can put your baby to the breast for sedative suckling as soon as you are ready for kangaroo care, unless your baby is suffering from bradycardia (slow heartbeat) or low oxygen levels in the blood. You can switch to breastfeeding as soon as the baby is ready for it. Gradually, he will gain enough strength to suckle longer and suck out more milk.
Literature
1 World Health Organization. Geneva, Switzerland; 2018. Media Centre: Preterm birth fact sheet; November 2017 [03/26/2018]. Available from : http://www.who.int/mediacentre/factsheets/fs363/en/ - World Health Organization. Geneva, Switzerland; 2018. "Media Center: Prematurity Fact Sheet"; November 2017 [3/26/2018]. Article at: http://www.who.int/mediacentre/factsheets/fs363/en/
Available from : http://www.who.int/mediacentre/factsheets/fs363/en/ - World Health Organization. Geneva, Switzerland; 2018. "Media Center: Prematurity Fact Sheet"; November 2017 [3/26/2018]. Article at: http://www.who.int/mediacentre/factsheets/fs363/en/
2 Duttaroy AK. Transport of fatty acids across the human placenta: a review. Prog Lipid Res . 2009;48(1):52-61. - Duttaroy A.K., "Transfer of fatty acids across the human placenta: a review". Prog Lipid Res. 2009;48(1):52-61.
3 Palmeira P et al. IgG placental transfer in healthy and pathological pregnancies. Clin Dev Immunol. 2012;2012: 985646. - Palmeira P. et al., Placental transfer of immunoglobulin G through the placenta in healthy and abnormal pregnancy. Klin Dev Immunol.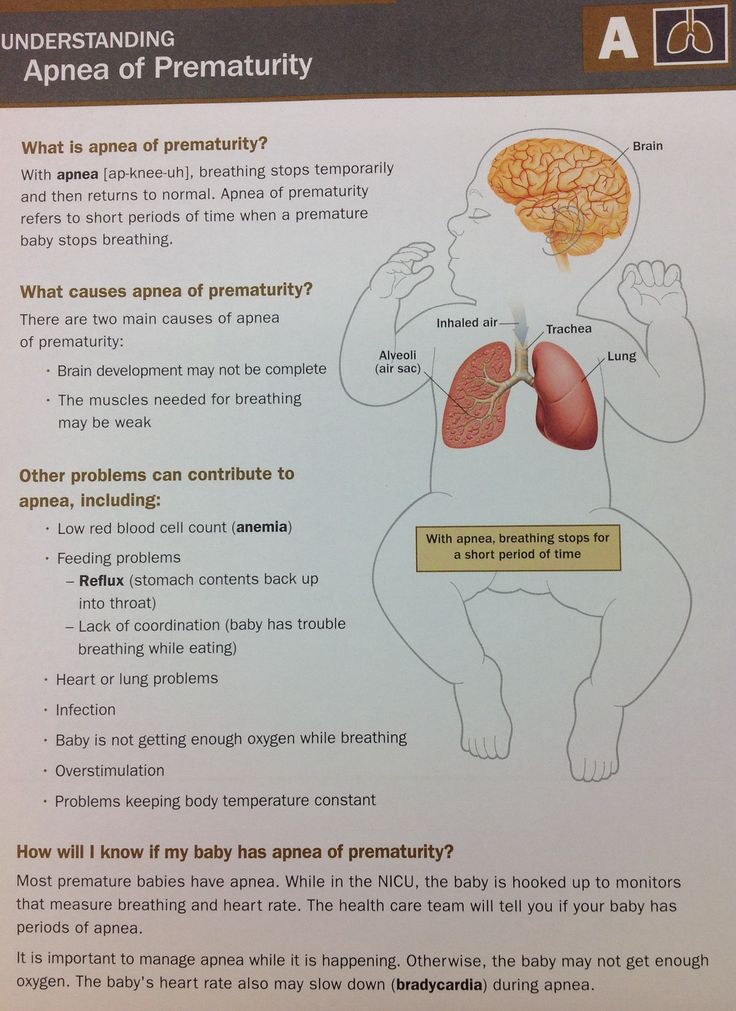 2012;2012: 985646. 5 Clin North Am . 2013;60(1):189-207. - Underwood, M.A., "Breast milk for the premature baby." 1):189-207.
2012;2012: 985646. 5 Clin North Am . 2013;60(1):189-207. - Underwood, M.A., "Breast milk for the premature baby." 1):189-207.
5 Pamblanco M et al. Bile salt - stimulated lipase activity in human colostrum from mothers of infants of different gestational age and birthweight. Acta Paediatr. 1987;76(2):328-331. - Pamblanco M. et al., "Bile salt-activated lipase and its activity in colostrum of mothers of infants of various gestational ages and birth weights." Akta Pediatr. 1987;76(2):328-331.
6 Dvorak B. Milk epidermal growth factor and gut protection. J Pediatr. 2010;156(2): S 31-35. - Dvorak B., "Epidermal growth factor in milk and gut protection". F Pediatrician (Journal of Pediatrics). 2010;156(2):S31-35.
7 Taylor SN et al. Intestinal permeability in preterm infants by feeding type: mother's milk versus formula. Breastfeed Med . 2009;4(1):11-15.- Theilon S.N. et al., "Intestinal permeability in preterm infants and its association with type of feeding: breast milk or formula." Brestfeed Med (Breastfeeding Medicine). 2009;4(1):11-15.
Breastfeed Med . 2009;4(1):11-15.- Theilon S.N. et al., "Intestinal permeability in preterm infants and its association with type of feeding: breast milk or formula." Brestfeed Med (Breastfeeding Medicine). 2009;4(1):11-15.
8 Newburg DS. Innate immunity and human milk. J Nutr . 2005;135(5):1308-1312. — Newburgh, D.S., "Natural Immunity and Breast Milk." F Int. 2005;135(5):1308-1312.
9 Patel AL et al. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J Perinatol . 2013;33(7):514-519.- Patel A.L. et al., "Impact of early breast milk on sepsis and health care costs in extremely low birth weight infants". Zh Perinatol (Journal of Perinatology). 2013;33(7):514-519.
10 Zhou J et al . Human milk feeding as a protective factor for retinopathy of prematurity: a meta-analysis. Pediatrics. 2015;136(6): e 1576-1586. - Zhou Q. et al., "Breastfeeding as a protective factor against retinopathy of prematurity: a meta-analysis." Pediatrix (Pediatrics). 2015;136(6):e1576-1586.
Human milk feeding as a protective factor for retinopathy of prematurity: a meta-analysis. Pediatrics. 2015;136(6): e 1576-1586. - Zhou Q. et al., "Breastfeeding as a protective factor against retinopathy of prematurity: a meta-analysis." Pediatrix (Pediatrics). 2015;136(6):e1576-1586.
11 Patel AL et al. Influence of own mother's milk on bronchopulmonary dysplasia and costs. Arch Dis Child Fetal . 2017;102(3): F 256- F 261. - Patel A.L. et al., "Effect of breast milk on bronchopulmonary dysplasia and health care costs." Arch Dis Child Fetal Neonate Ed. 2017;102(3): F 256- F 261.
12 et al . Improving the use of human milk during and after the NICU stay. Clin Perinatol. 2010;37(1):217-245. - Meyer P.P. et al., "Optimizing the use of breast milk during and after a stay in the neonatal intensive care unit." Perinatol wedge. (Clinical perinatology). 2010;37(1):217-245.
Clin Perinatol. 2010;37(1):217-245. - Meyer P.P. et al., "Optimizing the use of breast milk during and after a stay in the neonatal intensive care unit." Perinatol wedge. (Clinical perinatology). 2010;37(1):217-245.
13 Lucas A, Cole TJ. Breast milk and neonatal necrotising enterocolitis. Lancet. 1990;336(8730-8731):1519-1523. — Lucas A, Cole TJ, "Breast milk and neonatal necrotizing enterocolitis." Lancet 1990;336(8730-8731):1519-1523.
14 Schanler RJ et al. Randomized trial of donor human milk versus preterm formula as substitutes for mothers' own milk in the feeding of extremely premature infants. Pediatrics. 2005;116(2):400-406. - Chanler R.J. et al., "Randomized Trial of Donor Human Milk Versus Prematurity Formula as a Breast Milk Substitute in Severely Preterm Infants". Pediatrix (Pediatrics). 2005;116(2):400-406.
15 Vohr BR et al. Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birth weight infants at 18 months of age. Pediatrics. 2006;118(1): e 115-123. - Thief B.R. et al., Developmental Beneficial Effects of Breast Milk in the Intensive Care Unit on Extremely Low Birth Weight Infants by 18 Months of Age. Pediatrix (Pediatrics). 2006;118(1):e115-123.
Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birth weight infants at 18 months of age. Pediatrics. 2006;118(1): e 115-123. - Thief B.R. et al., Developmental Beneficial Effects of Breast Milk in the Intensive Care Unit on Extremely Low Birth Weight Infants by 18 Months of Age. Pediatrix (Pediatrics). 2006;118(1):e115-123.
16 Victora CG et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475-490. - Victor S.J. et al., "Breastfeeding in the 21st century: epidemiology, mechanisms and long-term effects". Lancet (Lancet). 2016;387(10017):475-490.
17 Lewandowski AJ et al. Breast milk consumption in preterm neonates and cardiac shape in adulthood. Pediatrics. 2016;138(1): pii : e 20160050. - Lewandowski, A.J. et al., "Breastfeeding in preterm infants and cardiovascular health in adulthood." Pediatrix (Pediatrics). 2016;138(1):pii:e20160050.
- Lewandowski, A.J. et al., "Breastfeeding in preterm infants and cardiovascular health in adulthood." Pediatrix (Pediatrics). 2016;138(1):pii:e20160050.
18 Meier PP et al. Which breast pump for which mother: an evidence-based approach to individualizing breast pump technology. J. Perinatol. 2016;36(7):493-499. - Meyer P.P. et al., Breastpump Selection: A Scientific Approach to Customizing Pumping Technology. J Perinatol (Journal of Perinatology). 2016;36(7):493-499.
19 Parker LA et al. Effect of early breast milk expression on milk volume and timing of lactogenesis stage II among mothers of very low birth weight infants: a pilot study. J Perinatol. 2012;32(3):205-209. - Parker L.A. et al., "Effect of early pumping on milk supply and timing of the second stage of lactogenesis in mothers of extremely low birth weight infants: a pilot study." J Perinatol (Journal of Perinatology). 2012;32(3):205-209.
2012;32(3):205-209.
20 Meier PP et al. Breast pump suction patterns that mimic the human infant during breastfeeding: greater milk output in less time spent pumping for breast pump-dependent mothers with premature infants. J Perinatol. 2012;32(2):103-110. - Meyer P.P. et al., "Pumping patterns that mimic breastfeeding behavior: more milk and less time for constantly pumping mothers of preterm infants." J Perinatol (Journal of Perinatology). 2012;32(2):103-110.
21 Parker LA et al. Association of timing of initiation of breastmilk expression on milk volume and timing of lactogenesis stage II among mothers of very low-birth-weight infants. Breastfeed Med . 2015;10(2):84-91. - Parker L.A. et al., "Effect of early pumping on milk supply and timing of the second stage of lactogenesis in mothers of extremely low birth weight infants: a pilot study." Brestfeed Med (Breastfeeding Medicine). 2015;10(2):84-91.
2015;10(2):84-91.
22 Lee J et al. Oropharyngeal colostrum administration in extremely premature infants: an RCT. Pediatrics. 2015;135(2): e 357-366. - Lee J. et al., "Oropharyngeal colostrum ingestion in very preterm infants: a randomized controlled clinical trial." Pediatrix (Pediatrics). 2015;135(2):e357-366.
23 Prime PK et al. Simultaneous breast expression in breastfeeding women is more efficacious than sequential breast expression. Breastfeed Med 2012; 7(6):442–447. - Prime D.K. and co-authors. "During the period of breastfeeding, simultaneous pumping of both breasts is more productive than sequential pumping." Brestfeed Med (Breastfeeding Medicine). 2012;7(6):442-447.
24 Uvn 9 ä s Moberg K . Oxytocin effects in mothers and infants during breastfeeding.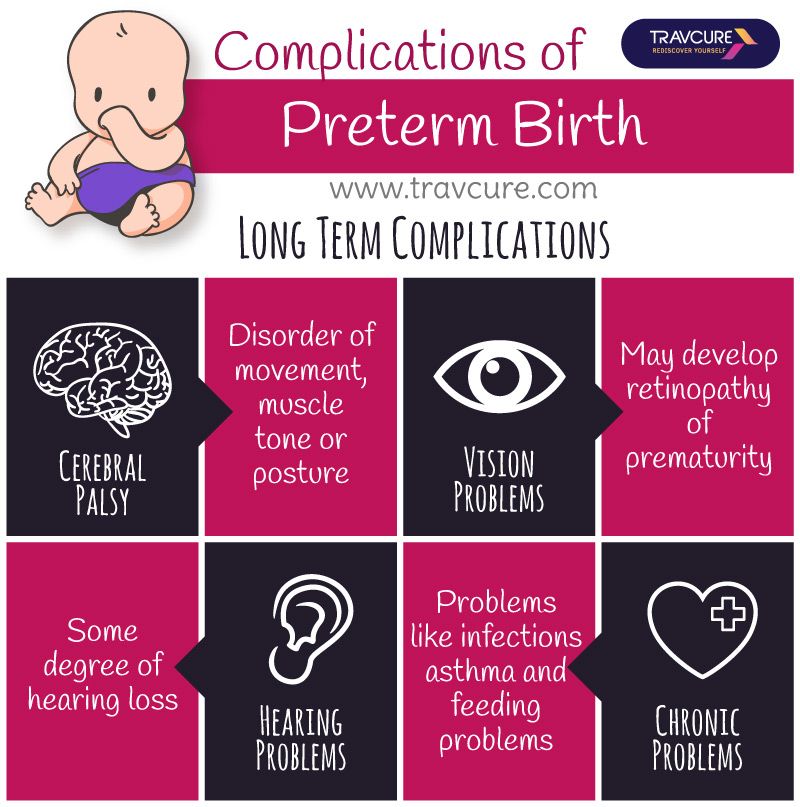 Infant 2013; 9(6):201–206. - Uvenas-Moberg K, Prime DK, "Oxytocin effects on mother and child during breastfeeding". Infant. 2013;9(6):201-206.
Infant 2013; 9(6):201–206. - Uvenas-Moberg K, Prime DK, "Oxytocin effects on mother and child during breastfeeding". Infant. 2013;9(6):201-206.
25 Boundy EO et al. Kangaroo mother care and neonatal outcomes: a meta-analysis. Pediatrics. 2015;137(1): e 20152238. - Boundi I.O. and co-authors, "The Kangaroo Method and Its Impact on Newborns: A Meta-Analysis". Pediatrix (Pediatrics). 2015;137(1): e20152238.
26 Acuña-Muga J et al. Volume of milk obtained in relation to location and circumstances of expression in mothers of very low birth weight infants. J Hum Lact . 2014;30(1):41-46 - Akunya-Muga, J. et al., "The amount of milk expressed by location and circumstances of pumping in mothers of extremely low birth weight infants." F Hum Lakt. 2014;30(1):41-46
27 Nyqvist KH et al. Towards universal kangaroo mother care: recommendations and report from the first European conference and seventh international workshop on kangaroo mother care. Acta Paediatr . 2010;99(6):820-826.- Nukvist K.H. et al., "On the Universality of the Kangaroo Method: Recommendations and Report from the First European Conference and the Seventh International Kangaroo Method Workshop". Akta Pediatr. 2010;99(6):820-826.
Towards universal kangaroo mother care: recommendations and report from the first European conference and seventh international workshop on kangaroo mother care. Acta Paediatr . 2010;99(6):820-826.- Nukvist K.H. et al., "On the Universality of the Kangaroo Method: Recommendations and Report from the First European Conference and the Seventh International Kangaroo Method Workshop". Akta Pediatr. 2010;99(6):820-826.
28 American Academy of Pediatrics - Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics . 2012;129(3): e 827-841.- American Academy of Pediatrics - Section "Breastfeeding", "Breastfeeding and the use of breast milk". Pediatrix (Pediatrics). 2012;129(3): e 827-841.
Read instructions before use. Consult a specialist about possible contraindications.
*RU No. ФСЗ 2010/06525 dated 03/17/2021
Peculiarities of feeding premature babies
Successful nursing of premature newborns, in addition to therapeutic measures, largely depends on the creation of optimal external conditions and adequate nutrition. According to modern theory of nutrition programming the quantity and quality of nutrients supplied during the prenatal period and the first months of a child's life determines the nature of metabolism and, as a result, affects a person's health throughout later life.
According to modern theory of nutrition programming the quantity and quality of nutrients supplied during the prenatal period and the first months of a child's life determines the nature of metabolism and, as a result, affects a person's health throughout later life.
Proper and nutritious nutrition in the early stages of life affects the overall development of the child, and also contributes in direct proportion to the reduction of the development of chronic diseases in adulthood (such as diabetes and arterial hypertension).
The purpose of enteral nutrition is to provide the body with the nutrients it needs to grow and develop.
Providing a premature newborn with an optimal amount of nutrients is quite difficult, given the morphofunctional immaturity of the digestive system and the lability of metabolic processes. The relatively high need of premature infants for nutrients is in conflict with the limited ability to assimilate them.
Feeding methods for premature babies are determined by the severity of their condition and depend on the body weight and gestational age of the baby at birth.
Successful feeding of a newborn is possible when sucking, swallowing and breathing become well coordinated.
The swallowing reflex is well developed already by 28-30 weeks of gestational age, but it is very quickly depleted. Fully matures by 34 weeks of gestation. When does sucking and swallowing coordinate? Already at 28 weeks of gestational age, all the components of sucking and swallowing take place, but the child is not yet able to coordinate them. Partially, this occurs by 32-34 weeks of gestation. Coordination of sucking and swallowing fully matures around 36-38 weeks of gestational age. From 37 to 38 weeks of gestational age, newborns are able to coordinate sucking, swallowing, and breathing without difficulty.
When feeding premature babies, you should pay attention to four points: when, with what, in what volume, by what method to feed.
The first feeding should be started as soon as it becomes clinically possible. Earlier introduction of breast milk helps to reduce the frequency of infections, maturation of the gastrointestinal tract, immune functions, and improved calcium metabolism.
Newborns weighing more than 2000 g and gestational age more than 33 weeks, who do not have other diseases, can be attached to the mother's breast as early as the first day of life. In this case, you should carefully monitor the appearance of signs of fatigue (cyanosis of the nasolabial triangle, shortness of breath, etc.). Their appearance is an indication for the transition to feeding expressed breast milk from a bottle. Efforts should be aimed at preserving breast milk as much as possible, taking into account the special biological value of mother's native milk for an immature child and the important role of mother-child contact during feeding. For premature babies, free feeding is unacceptable due to their inability to regulate the amount of sucked milk and the high incidence of perinatal pathology.
Babies born before 33 weeks' gestation are usually tube-fed to avoid the risk of aspiration resulting from a lack of coordination between sucking and swallowing. With a non-severe condition of the child and a body weight approaching 2000 g, a trial feeding from a bottle can be carried out, with unsatisfactory sucking activity, tube feeding is prescribed in full or in part. In order to maintain and maintain lactation in the mother, regular expression of breast milk is necessary.
Enteral feeding of very preterm infants (weighing less than 1500 g and less than 30 weeks' gestation) is carried out through a tube.
The caloric method is used to calculate the required amount of feeding for premature babies. The calorie content of the diet of a prematurely born child increases gradually and daily.
Caution and Graduality Feeding Guidelines for Premature Babies Less Than 33 Weeks Gestational Age Less Than 2000g
For a premature baby, the best bioavailability is the milk of a woman who has given birth prematurely, then formulas for premature babies, and then the milk of a woman who has given birth at term.
Women's milk after preterm birth has a special composition, it contains more protein, less lactose with the same total level of carbohydrates. In addition, it has a higher content of a number of protective factors, in particular lysozyme and secretory IgA. Despite the special composition, the milk of women who gave birth prematurely can satisfy the nutritional needs of only premature babies with a relatively large body weight - more than 1800-2000 g. Premature babies with a lower body weight are deficient in a number of nutrients. For them, breast milk must be further enriched with protein, calcium, phosphorus, iron, and vitamins. This can be achieved by replacing part of the required amount of breast milk with a specialized formula for premature babies or by adding breast milk enhancers. When enrichers (enhancers) are used, the main advantages of breastfeeding are preserved and at the same time the high nutritional requirements of the premature baby are ensured. With artificial feeding, specialized mixtures intended for feeding premature babies should be used.