Mothers feeding babies with breast videos
Breastfeeding & baby-led attachment | Raising Children Network
Renee Kam (lactation consultant): Baby-led attachment is where a baby uses their own instincts to find the mother’s breast on their own accord. Baby-led attachment really helps to lay down the foundation for breastfeeding. A baby who has had many opportunities, particularly in the early weeks, to do baby-led attachment becomes a lot more orientated towards the breast.
Adele (mother of Charlie, 5 years, Noah, 3 years, and Holly, 4 weeks): I did baby-led attachment because I had a lot of trouble feeding my first baby and getting him to attach and when I saw a video of baby-led attachment it just looked like a natural way to do it, so I thought I would try it to see if that meant that I didn’t have attachment issues with the children I had after my first one.
Miranda (mother of Mattie, 8 years, Tacy, 6 years, Sedna, 7 months): When I had my second baby, when she was born at home and she was lying on me, she all of a sudden attached by herself, which was a wonderful feeling but I never followed-up on it because I didn’t know anything about it. So then when we moved to Australia I so wanted to try it so we tried it with this one. It really started at home, so when we got home we started doing it. You don’t have to do it straight away – baby-led attachment – it’s something that they can do for quite a few weeks after they’re born. It’s imprinted in their being, I guess.
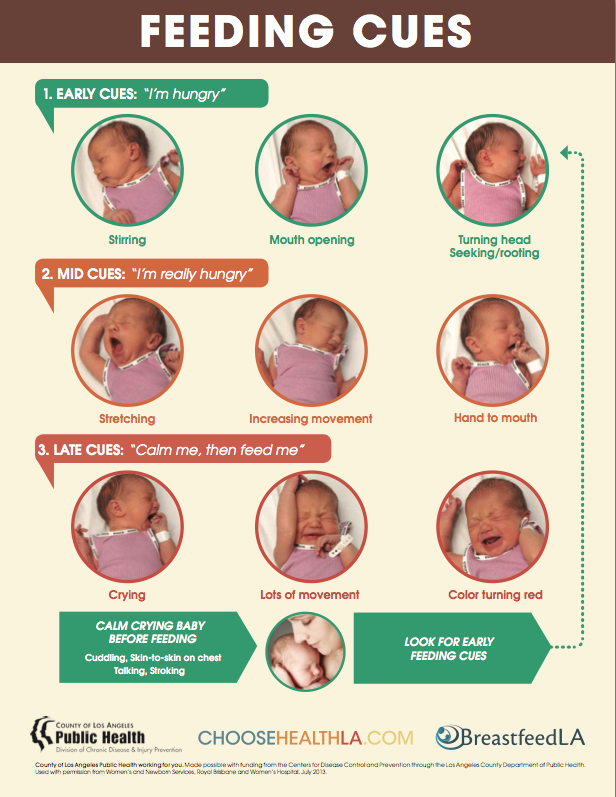
Renee Kam: If a mother wants to do baby-led attachment the tips that I would give her would be the timing of it. So a baby will be able to follow through on their instincts best when they’re calm. So it would be when the baby’s showing early feeding cues such as turning their head from side to side with mouth open, sticking their tongue out, sucking on their hands, or it might be as soon as their baby wakes up from a sleep. So in those situations baby is typically calm and then if the baby is then placed skin-to-skin contact with the mum and the mum, say, is in a semi-reclined position, then that will help a baby to follow through on their instincts to find their mother’s breast.
Narrator: Find a comfortable position. Many mothers find that a semi-reclined position with pillows behind them for support works well. A partially laid-back position allows gravity to assist the baby in moving to the breast. With as much skin-to-skin as possible between you and your baby, place your baby on your chest facing you between your breasts with her head just above your breasts. Start when your baby is calm, such as when she is showing early feeding cues like turning her head from side to side with her mouth open.
As your baby starts to instinctively move towards a breast, she will start to lift her head and bob it around. As she moves towards a breast, you may find it helpful to hug her bottom in close to you and to support her neck and shoulders with your hand and wrist. It is important to avoid putting pressure on her head as she needs her head free to instinctively move it into an extended position to help her attach and feed well.
When her head nears your nipple, she may nuzzle around to find your nipple and bring her tongue toward it. When she finds the right position, she will anchor with her chin, open her mouth wide, attach and begin sucking.
When she finds the right position, she will anchor with her chin, open her mouth wide, attach and begin sucking.
Renee Kam: Straight after a baby is born for the first 1 to 2 hours after they’re born, they’re typically alert and eager and ready to receive their first breastfeed. So when placed into skin-to-skin contact with their mother straight after birth, then that can allow the baby to do baby-led attachment, find the mother’s breasts on their own accord and receive their first breastfeed.
Adele: I did skin-to-skin with all of my children in hospital. So with the baby it probably took a few minutes before like they would kind of just be laying there for a little while and it was a few minutes before they kind of started moving around. But they did the bopping around and choosing a side and finding the nipple and all of that themselves.
Renee Kam: The great news is even if you don’t get to do baby-led attachment straight after a baby is born, babies’ instincts to find a mother’s breasts are easily reproducible for at least the first few months. When a mother and baby are in skin-to-skin contact, there are many benefits of it such as the baby’s heart rate and temperature, blood sugar levels, breathing rate are all kept stable and also when a mother and baby are in skin-to-skin contact it also helps a mother to be able to learn her baby’s feeding cues.
When a mother and baby are in skin-to-skin contact, there are many benefits of it such as the baby’s heart rate and temperature, blood sugar levels, breathing rate are all kept stable and also when a mother and baby are in skin-to-skin contact it also helps a mother to be able to learn her baby’s feeding cues.
Miranda: As with the baby-led attachment, I also did try the mother-led attachment, attachment and feeding and it was quite painful. I went to see a lactation consultant a couple of times for her to help as well. Of course, they have told me to use the baby-led attachment, which was great.
Renee Kam: Even if the mother doesn’t have any breastfeeding problems, by using baby-led attachment frequently, particularly in the early weeks, it can help to reduce the risk of developing any breastfeeding problems such as the baby simply not attaching at all or sore nipples.
Miranda: Persevering with the baby-led attachment actually did help to heal the wounds and I think it was around 3 weeks that we had a happy breastfeeding relationship.
Renee Kam: A mother can do baby-led attachment whenever it’s right for her and her baby to do so. By having done baby-led attachment whenever she feels comfortable to do so, then it means that when she is breastfeeding in public, it makes it easier because baby knows what they’re doing and baby attaches easier to the mum’s breast.
Adele: So I think the baby-led attachment improved my confidence by I was able to see them feeding well, when I could look at them and I could see that they were attached really well and I could hear the swallowing and I knew we were having a good feed and so I didn’t have to really think about what I was doing with them.
Miranda: It helps to know about the fact that everyone is different. With baby-led attachment, it doesn’t matter because babies just go for the breast; they know what to look for.
Renee Kam: Baby-led attachment – it helps a mum and baby get breastfeeding off to a really good start. Then, it may help a mum to be able to breastfeed for as long as she wanted to and reach her own breastfeeding goals.
Then, it may help a mum to be able to breastfeed for as long as she wanted to and reach her own breastfeeding goals.
International BreastFeeding Centre | Breastfeeding videos
Breastfeeding Videos
REALLY GOOD DRINKING
The pause in the chin as the baby opens his mouth to the maximum, just before closing his mouth, indicates his mouth is filling up with milk; the longer the pause, the more milk the baby is taking in. Thus, it is obvious that the advice to feed the baby 20 minutes (10 minutes, 30 minutes, whatever) on each makes no sense. A baby who drinks as this baby drinks for 20 minutes on the first side could easily refuse to take the second side since he would be full. Even a shorter period of time drinking as he does could easily fill him up.
Compare this baby to the baby in the “nibbling” video. The baby in the “nibbling” video could easily spend hours on the breast and not get enough. The whole notion of feeding a baby by the clock makes no sense at all. The pause can also be seen in the first few days of life. See the videos of the 2 day old, 28 hour old and 10 hour old babies
The baby in the “nibbling” video could easily spend hours on the breast and not get enough. The whole notion of feeding a baby by the clock makes no sense at all. The pause can also be seen in the first few days of life. See the videos of the 2 day old, 28 hour old and 10 hour old babies
GOOD DRINKING
Note the position of the baby at the breast. Chin in the breast, nose not touching, baby’s lower lip covering more of the areola with the lower lip than the upper. An asymmetric latch.
The pause in the chin as the baby sucks means the baby just got a mouth full of milk. The longer the pause, the more milk he got.
A baby who drinks like this for 20 minutes straight (for example, we are not recommending feeding by the clock), might not take the other side, he would be full.
Timing feedings makes no sense.
NIBBLING
This baby is eight weeks old and is doing almost no drinking, though very occasionally one sees a short pause in the baby’s chin. A baby who breastfeeds only with this type of sucking could stay on the breast for hours and still not get enough milk. Something needs to be done here and if achieving a better latch, using compression doesn’t help, the baby almost certainly needs to be supplemented. The best way to supplement the baby is with a lactation aid at the breast. Why?
1. Babies learn to breastfeed by breastfeeding
2. Mothers learn to breastfeed by breastfeeding
3. The baby continues breastfeeding and thus continues getting milk from the breast and thus increases the mother’s milk production
4. The baby is not likely to refuse to latch on
5. There is much more to breastfeeding than breastmilk, as important as the breastmilk is
See the video clip “Inserting a Lactation Aid”
2 DAY OLD/COMPRESSIONS
The baby in this video is only 40 hours old.
Baby has a pretty good latch. Notice his chin is in the breast, his nose is away from the breast and he covers more of the areola with his lower lip than the upper lip.
During the first part of the video, the baby has an occasional pause in the chin, but is mostly “nibbling” without drinking.
Mother is using compressions, but not always as we recommend. She should compress while the baby sucks, but does not drink and not while he’s not sucking at all.
Compressions at this age (before milk “comes in”), often work only after several series of compressions, unlike later, when the milk supply is greater, when compression usually works immediately.
Around 1 minute into the video, the baby starts pulling a little at the breast, becoming impatient with the slow flow.
Then, about 1 minute and 14 seconds, the baby starts to drink vigorously, and you can see several pausing type sucks in a row.
The mother maintains compression until baby no longer drinks, then releases (at 1 minute 30 seconds).
The baby starts sucking again at about 1 minute 37 seconds. Babies who are latched on and hungry will start sucking on their own. No need to tickle their feet or put cold cloths on their foreheads.
Babies do not fall asleep at breast because they are tired, but rather because the flow is slow. How to maintain the flow?
1. A good latch
2. Compressions when the baby is sucking but not drinking
See the how the baby in the video clip Introducing a lactation aid wakes up and drinks vigorously when the flow of milk increases again. Notice around two minute mark, the compression once again works well.
NOT YET LATCHING, FINGER FEED TO LATCH
Finger feeding is to be used primarily to prepare a baby who does not latch on to take the breast.
Note that finger feeding is done only long enough to calm the baby and to get the baby sucking well. This rarely takes more than 60 seconds.
It should not be used as a method of supplementation when the baby does take the breast. In such a case supplementation, if necessary, should be given at the breast with a lactation aid.
We filmed this baby because he had already latched on after being finger fed.
Why did he not latch on to the right side in this video?
• Because he already had fed on the right side, the flow of milk from the breast was slower: babies like fast flow and even if the lactation aid would provide him with more flow, it wasn’t enough
Why did he latch on to the left side?
• Because he hadn’t yet fed on the left side, the breast was “fuller” and the flow was rapid: babies like fast flow
Note that we do not try to force a baby to stay at the breast. If the baby struggles, allows the breast into his mouth but doesn’t suck, or cries, then we let him come away from the breast and try again.
• If the baby latches on, there is no need to try to force him to stay, he’s latched on
• If the baby does not latch on, trying to force him to stay at the breast is futile and likely to make him angrier or “go limp”
INSERTING A LACTATION AID
This baby needs to receive supplementation. It is best that the baby receive this via lactation aid because:
1. The baby is still on the breast and breastfeeding.
2. Babies learn to breastfeed by breastfeeding.
3. Mothers learn to breastfeed by breastfeeding.
4. The baby is still getting milk from the breast thus helping increase the mother’s milk production.
5. The baby is not likely to reject the breast as he would if he were supplemented by bottle or by any method not on the breast.
6. There is more to breastfeeding than breastmilk; the baby and mother are in close physical contact.
One way to introduce the tube is to insert it while the baby is at the breast as in this video clip. The other is to line up the tube with the nipple and latch the baby on the breast and lactation aid tube at the same time.
Note the position of the baby:
1. The baby’s chin touches the breast but nose does not touch.
2. The baby covers more of the areola with his lower lip than his upper lip.
3. The baby is slightly tilted up towards the mother.
The baby has now fed from both breasts and is not getting much milk flow (mostly nibbling at the breast—see video clips of babies drinking or not drinking). It is time to supplement.
Note the following:
1. The breast tissue is eased out of the way so that the corner of the baby’s mouth is visible.
2. The fact that the baby is tilted slightly upwards makes it easier to find the corner of the baby’s mouth and insert the tube.
3. The tube is inserted in the corner of the baby’s mouth.
4. The tube is pushed almost straight back towards the back of the baby’s throat but also slightly upward toward the roof of the baby’s mouth.
5. The milk moves down the tube to the baby’s mouth, but the baby does not drink (see video clips of babies drinking or not drinking). Something is not working.
6. The mother is attempting compression, but compression should be done when the baby is sucking and not drinking, not when the baby is not sucking at all. Moreover, compression while the baby is being supplemented at the breast with a lactation aid is not necessary.
7. At 21 seconds into the video, I fiddle with the tube placement, and now it starts working. The baby is drinking.
8. Notice the baby pops his eyes open when he starts getting milk again. Babies are not “lazy”; they respond to milk flow. Young babies such as this one tend to fall asleep when the flow of milk is slow, not necessarily if they have had enough.
9. More fiddling with the tube at about 35 seconds. If the baby is well latched on and tube is well placed, supplementing using the lactation aid takes no more time than giving the baby the bottle or finger feeding. Using finger feeding to supplement when the baby takes the breast is not the best approach either.
10. At about 1 minute into the video, I pull the baby’s chin down a bit. Remember, good latch and good placement of the tube make this system work best. Pulling down the chin gets more of the breast into the baby’s mouth.
11. At about 1 minute and 18 seconds, we bring the baby around even more asymmetrically by having the mother push the baby’s bottom in with her forearm.
12. At about 1 minute and 55 seconds, milk comes out of the baby’s mouth means something is not right. Baby has slipped off the breast or the tube has moved. Fiddling with the tube again makes it work properly again.
10 HOUR OLD BABY
This baby is only 10 hours old. Notice the asymmetric latch: chin touches the breast, but not the nose and the baby covers more of the areola with his lower lip than his upper lip. He is also tilted up somewhat towards the mother.
He is drinking milk from the breast. You can tell because of the pause in the chin just as he opens his mouth to its widest before closing again. The pause is subtle here because the baby is getting only small amounts of colostrum—as nature intended! If necessary, compression can help the baby get more milk (see the video clip of the 2 day old baby at this site). The very large amounts of formula an artificially fed baby gets in the first few days is not physiologic or natural or normal or ever been proved to be safe.
BABY 28 HOURS OLD ASSISTED LATCHING
Shows latching on. Not perfect, but good enough. The mother had no pain. It did take two tries to get the baby to latch on, but that’s okay; there’s no point in trying to force a baby who does not take the breast to stay on the breast. It won’t work. Note the baby has an “asymmetric” latch, with the chin touching the breast, the nose not touching the breast, and he covers more of the areola with his lower lip than the upper.
Compressions help the baby get more milk.
BABY 28 HOURS OLD – BABY-LED MOTHER-GUIDED LATCHING
The baby starts searching for the breast. The mother guides him towards the nipple. The baby opens up fairly wide, but the mother does not bring the baby on as well as she could and the baby has a shallow latch. He should have more of the breast in his mouth.
The baby is mostly nibbling at first though there is an occasional pause in the movement of the chin (see other videos showing good drinking).
The mother starts compressing around 1 minute and 10 seconds, and the baby responds by starting to have pausing-types of sucks that indicate he is getting milk well.
BABY-LED MOTHER-GUIDED STARTED UPRIGHT LEFT BREAST, LATCHES
When the baby does not yet take the breast or refuses it completely, this technique can help to put the baby in a state where he can accept the breast. The baby is skin to skin with the mother and indicates when he is ready to search for the breast. When he starts searching, the mother helps him, guiding him toward the breast, supporting his back and neck. The mother is careful not to hold his head. Babies need to have their necks supported but not their heads. See the information sheets The Importance of Skin to Skin Contact and When the Baby Does Not Yet Latch.
4 DAY OLD AFTER TONGUE-TIE RELEASE WITH COMPRESSIONS
The baby just had a tongue tie release.
The mother is doing compressions appropriately. She waits to see if the baby is drinking or not (pause in the chin). If the baby is not drinking, she compresses, holds the compression until the baby stops sucking or stops drinking and then releases. She waits for the baby to start sucking and if the baby starts sucking but does not drink, she repeats the process.
SQUEEZING NIPPLE DEMONSTRATING DIFFERENCE BETWEEN POOR LATCH
When the baby latches on to the nipple only, he gets very little milk.
When the baby latches on where he should, the milk flows rapidly.
CUP FEEDING
A good alternative to the bottle. Particularly useful for the baby who is refusing the breast.
Note that the baby laps the milk up with his tongue. One does not pour the milk down his throat.
JIGGLING AND PULLING
This is an older baby, about 3 or 4 months of age, whose mother’s production has decreased. See the information sheet Slow Weight Gain Following Early Good Weight Gain for some reasons this decrease in milk production might occur. Some of the reasons that may result in a decreased milk production include the mother’s using a hormonal birth control method (including hormone releasing intrauterine devices or intravaginal hormone releasing rings), the mother’s feeding one breast at a feeding “as a rule” instead of “finishing” one side and then offering the other. But the most common reason is the one discussed in the paragraph “This reason (number 11) requires more explanation”.
The baby is jiggling and unsettled at the breast because the flow of milk is slow. Note that he hardly drinks at the breast (very few pauses, see the videos Really Good Drinking, and Good Drinking), though his chin is a little bit difficult to see.
This sort of behaviour is often said to be due to an over rapid milk flow but by watching the chin one can see that this behaviour in this case is due to too slow milk flow. However, babies pull at the breast more frequently because the flow of milk is slow rather than because the flow of milk is “too rapid”.
Note that giving such babies bottles, may quickly result in their refusing to latch on.
TONGUE–TIE RELEASE
A simple and quick procedure that can make a significant difference in breastfeeding success. The research supporting tongue-tie release is compelling.
VASOSPASM TURNS PINK
This mother’s nipples turn white after baby has finished feeding. They turn white for some time and then eventually turn pink again. This change in colour is sometimes accompanied by throbbing and burning in the nipples. This is often due to poor latching and/or a yeast infection.
If our free resources have been helpful, make a donation today!Support ibc!
Lactation support is not funded by any level of Canadian government. Your support helps us continue to offer the services for which it has become renowned – helping and supporting families to achieve their own breastfeeding goals. It also helps us to provide free support and resources via our website to families and health care providers unable to visit us in person.
Individual donations represent the single largest source of support for ibc. Thank you!
Donations can be made at canadianbreastfeedingfoundation.org. Please direct your donation (Fund/Designation) to ibc – The International Breastfeeding Centre.
Charitable tax receipts are available.
Breastfeeding for beginners | Philips Avent
search support iconSearch Keywords
feeding, because it will take a long time during the first few months of a child's life. In this article, we will discuss all of its main aspects, from the basic principles of breastfeeding to the best tips for effective newborn feeding.
As always, if you have any questions or concerns, seek the opinion of another specialist.
Basic principles of breastfeeding
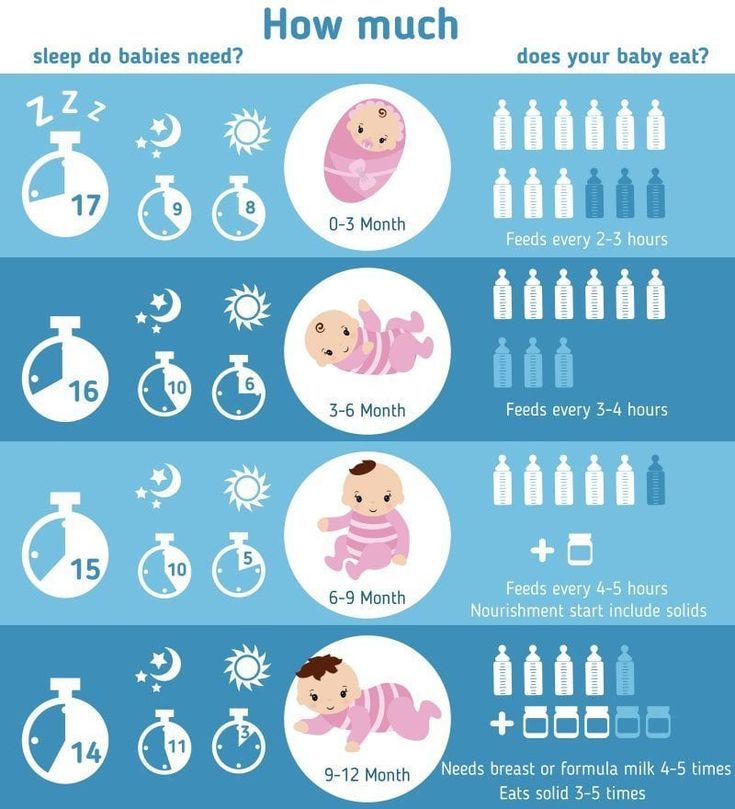
Although every baby is different, newborns usually eat every two to three hours, for a total of 8 to 12 times a day. In the first one or two days after birth, babies usually drink 25-50 ml of milk per feeding. This volume will gradually increase to 50-75 ml when the baby is about two weeks old.
More information on how much a newborn should eat can be found here.
How long does one feeding last?
Again, every baby is different, so there is no set time frame for every newborn. But in general, breastfeeding a newborn takes five minutes to one hour. This time depends on the size, age of the baby and the frequency and duration of feeding the newborn.
How to start breastfeeding?
In the very first minutes of a child's life, his mother should put the baby on her chest and ensure body contact. This time is called the "golden hour": it is at this hour that a connection is established between mother and child and the newborn's natural instinct to seek the breast manifests itself. As soon as the child begins to show signs of hunger, you need to give him a breast.
Mothers who are just learning to breastfeed their newborns should remember that comfort is key. There is no better way to ensure breastfeeding success than by creating a comfortable and relaxing environment for the mother. For starters, mom can sit comfortably on the couch, on the bed, or in a chair with pillows to support her back while feeding. Breastfeeding moms can get creative with breastfeeding and choose specific lighting, soothing music, or anything else that helps them relax.
Bring your baby to your breast, not the other way around. If you want to make breastfeeding a newborn easier, then do not lean towards the baby, but bring it to your chest. The baby's mouth should be opposite the nipple, the neck should be straight, and the shoulders and hips should be in line. Mom can also lightly touch her nipple to her baby's nose and mouth to encourage him to latch on.
Support your chest. Holding the newborn with one hand, the mother can place the other hand directly under the breast to support it. When learning to breastfeed, some mothers prefer to leave one hand free; in this case, a rolled towel can be used.
Breastfeeding can be done in different positions; experiment with them to find the one that works best for you and your baby. We list the most common breastfeeding techniques below:
- Cradle. In this position, the baby lies on the mother's hand from the side of the breast, which he sucks. The baby's head lies on the mother's elbow during feeding.
- Cross cradle. With a cross cradle, the mother holds the baby with the hand opposite to the mammary gland that the baby sucks. With the other hand, mom can support her breasts.
- Underhand or Football. In this position, the mother holds the child next to her, putting her back on her arm.
With the other hand, she supports the baby's head, facing the mammary gland, with which she feeds the baby.
- Lying on your side. In this position, the mother lies on her side, and the child lies next to her, facing her chest. Mom can support the child under the back with the hand that is on top, or put a folded towel under the back of the child.
Newborn Breastfeeding Tips
After looking at breastfeeding techniques, here are some tips for new mothers:
A good grip is important for both mother and baby. With a good grip, the baby will suck out milk correctly, and the mother's nipples will not hurt. To achieve a good latch, the mother needs to find a position that makes it easier for the newborn to latch onto the breast, and to do this, she should experiment with different positions. If a mother is having difficulty feeding, she should contact a lactation consultant.
2. Maintain milk supply. Sometimes a nursing mother cannot be constantly with her child during feedings. In such cases, it is very important to maintain milk production. An excellent solution for maintaining milk production when mother and baby are not together is pumping milk.
Take a look at this double breast pump: it reduces pumping time and features a massage petal attachment to gently stimulate milk flow.
3. Breastfeeding everywhere. One of the many benefits of breast milk is that mom always has it with her. But some moms feel awkward at first when they have to breastfeed their baby in public. For such mothers, we recommend that you first practice breastfeeding your newborn in front of a mirror and choose clothes that allow you to cover your breasts during feeding. A shawl or scarf can help with this - with them, the mother will feel more comfortable when feeding the baby outside the home.
And to keep clothes dry and clean while breastfeeding, we recommend that mums use these disposable bra pads with a porous and breathable structure: they do not leak and let air through.
Be prepared for difficulties. It is important for moms not to panic or get upset when faced with a common breastfeeding problem, such as insufficient milk production, breast engorgement, clogged milk ducts, mastitis, or sore nipples. To feel calm and confident during all stages of breastfeeding a baby, mothers need a circle of support: family members, friends, and healthcare professionals. The main thing is to stay calm, but if a mother is concerned about any aspect of breast health, she should definitely see a doctor. Learn more about breastfeeding difficulties and how to overcome them.
Articles and tips from Philips Avent
Baby+ app
Download the app and track your baby's development and growth with trackers and keep those special moments forever.
Download app:
Pregnancy+ app
Download one of the world's best pregnancy tracking apps for weekly helpful information, articles and tips about pregnancy and baby development.
Download app:
You are leaving the Philips Healthcare (“Philips”) official website. Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
I understand
You are about to visit a Philips global content page
Continue
How to apply the baby while breastfeeding
Desired position
First of all, you need to correctly position the baby at the chest. Take him in your arms so that he is turned to his mother with his whole body, the child's face should be close to the chest, his mouth is wide open. In case of an incorrect position, the baby's body is deviated from the mother's, the chin does not touch the chest, the lips are extended forward. This is an important point, because if the baby starts sucking the breast incorrectly, he will not receive enough milk, the baby will begin to throw and grab the breast again, and sometimes even refuse it.
Correct grip
Now you need to correctly insert the breast into the baby's mouth. In general, every healthy newborn has reflexes that help him eat. But the baby does not have a reflex that would help him keep his mother's breast in his mouth, and the baby cannot properly grasp the nipple himself. Therefore, the child needs help - put the breast into the crumbs' mouth so that it captures not only the nipple, but also the areola. If the baby grabs only the nipple, then the pressure on the ducts of the mammary gland will be weak and the milk will flow poorly from the breast. In addition, if a child suckles only the nipple, his skin is often damaged and cracks appear on the nipple. Sometimes, in order to give a breast to a child, a mother pinches the nipple and areola with her fingers and tries to push them into the baby's mouth. You don’t need to do this, it’s much easier to just touch the nipple to the baby’s lips (stimulate the capture reflex), wait until the baby opens her mouth wide, and quickly give him the breast.
simple postures
Immediately after delivery, especially if there was a caesarean section or episiotomy (or just want to lie down), you can feed the baby lying on its side . You lie in bed, put the baby next to you, bend your lower arm at the elbow, and support the back of the child with your upper palm. The baby should lie on the bed parallel to your body, his mouth should be at the same level and very close to your nipple.
The second easiest position for feeding - sitting position . To do this, take the baby in your arms, bend your arm at the elbow from the side of the breast with which you will feed the baby. At the same time, the baby's head lies on a bent arm. To make it more convenient for you, put a pillow under your elbow (regular or special for feeding), you can also put something under your legs.
For variety
We have mastered simple poses - now you can try to feed the baby from other positions, for example, in position "jack" : mother and baby lie on their sides parallel to each other, but now their legs and head look in different directions. There is also such a pose - "chest on top" : the baby lies on its side, and the mother, as it were, hangs over him. In this position, it is easier for milk to go down the ducts, and it is easier for the child to get it. To make everyone comfortable, the baby should be put on some kind of elevation (for example, on a pillow).
Prevention of lactostasis
Laxtostasis, or stagnation of milk, is a very unpleasant thing. It occurs when any lobule of the mammary gland is not emptied of milk to the end. To prevent it or if it has already occurred, you need to feed the baby from under hands (from under the arm). In general, if you feed in this position at least once a day, then the lower and lateral lobes of the breast (the most frequent places of lactostasis) will be better emptied.
In this position, you put the baby on the pillow, the baby's head is located at your chest, and the body and legs are behind you (facing towards your armpit). Here's the important thing: the baby's mouth should be at the level of the nipple, then your back will not get tired during feeding.
The child likes it
If your milk flows out too quickly and the baby does not have time to swallow it, then you can also feed the baby in position "baby on top" . You lie on your back (with your head on the pillow), and the baby is applied from above. Grown up children still love this pose because it is more convenient for them to observe the world around them “from above”.
The second favorite position of older children is that the baby sits or stands while feeding . Children like that they can eat and look at their mother, and at any time they can kiss the breast on their own.
So learn how to properly breastfeed your baby, master different positions, and then you can feed for a long time and with pleasure!
When the baby suckles the breast incorrectly, the skin in some areas of the nipple is constantly irritated and rubbed, cracks appear. With each feeding, the condition worsens, the cracks become deeper and longer, and the pain intensifies.