2 day old baby sleeping and not feeding
Sleepy Baby – Why And What To Do
Nobody likes to disturb a sleeping baby, but sometimes a baby can be too sleepy for their own good. At times like this they may need you to take action.
Your newborn baby needs to nurse actively for one or both breast at each feed. Offer the second breast after they seem to have finished at the first, although they may not want both sides at every feed.
What makes a baby sleepy?
Recovering from birth: In the first few days, some babies are sleepy or uninterested in feeding. It’s especially true for small babies, after a difficult labour or birth, or if you received drugs for pain relief during labour.
Jaundice or an infection may make a baby sleepy. Newborn jaundice is normal but frequent breastfeeding helps prevent it becoming a problem.
Not enough milk: Your baby may sleep to conserve energy if they are not getting enough food. They may also sleep longer that is good for them if they are apart from you.
Is my baby too sleepy?
To gain weight and stimulate your milk production, expect your newborn to:
- Breastfeed effectively at least 8–12 times in 24 hours
- Feed actively from one or both breasts at each feed, swallowing regularly.
- Nurse at least every 2–3 hours from the start of one feed to the next, with one longer sleep of 4–5 hours.
- Have periods where they breastfeed on and off for several hours, usually in the evening.
- Gain weight from day 4 and regain birth weight by about two weeks.
Look at our page Beginning Breastfeeding for more information. If your baby is too sleepy to do all these things they may need your active help to ensure they are nursing effectively and getting enough milk.
Is my baby getting enough milk?
A baby may lose up to 7% of their birth weight during the first few days. From around day 3-4, expect them to start gaining, and to regain their birth weight by 10-14 days. Many breastfed babies gain around 200-235g (7-8oz) as week for the first 2-3 months. If you baby consistently gains less, or they haven’t regained their birthweight by 14 days, seek skilled help to assess whether they are getting enough milk. What comes out is a sign of what has gone in, so counting dirty nappies can be a useful guide between weighing sessions. For more information to help you know if your baby is getting enough milk in the first few days, you could read our article here about signs of effective feeding in the early days. And then after the first few days, this article will help you decide if your baby is getting enough milk.
If you baby consistently gains less, or they haven’t regained their birthweight by 14 days, seek skilled help to assess whether they are getting enough milk. What comes out is a sign of what has gone in, so counting dirty nappies can be a useful guide between weighing sessions. For more information to help you know if your baby is getting enough milk in the first few days, you could read our article here about signs of effective feeding in the early days. And then after the first few days, this article will help you decide if your baby is getting enough milk.
| Age | Dirty nappies per 24 hours |
|---|---|
| 1-2 Day | 1 or 2 greenish-black tarry meconium poos |
| 3-5 days | At least 3 green transitional poos |
| 5+ days | At least 3-5 yellow, loose unformed poos the size of a 2p coin or larger |
Remind your baby to nurse
If your baby is too sleepy or groggy to rouse themselves every few hours, you will need to wake them to feed to ensure they get enough milk. This will be easier if your baby is in a light sleep cycle: watch for rapid eye movements under their closed eyelids, arm and leg movements, sucking activity and changes in their facial expression.
This will be easier if your baby is in a light sleep cycle: watch for rapid eye movements under their closed eyelids, arm and leg movements, sucking activity and changes in their facial expression.
- Aim for your baby to feed at least 10 times in 24 hours, including at least once at night
- Encourage active nursing on the first breast, watching and listening for signs of swallowing.
- Use breast compression (see below) to keep your baby nursing actively.
- Offer the other side in the same way. You can switch back and forth several times if it helps your baby stay awake and feed.
- Encourage cluster nursing whenever your baby is more alert.
- Give expressed milk if they aren’t feeding well.
- Keep them close by—day and night—so they don’t sleep too long and you don’t miss their feeding cues.
Also try
- Dimming the lights and keeping your surroundings quiet and peaceful.
- Keeping the room temperature at around 18°C or undressing your baby a little if the room is warm.
 Being too hot can make a baby sleepy.
Being too hot can make a baby sleepy. - Unwrapping any blankets.
Newborn feeding cues
Signs of interest in feeding include:
- Mouth movements; smacking or licking his lips
- Sucking on lips, tongue, hands, fingers, toes, toys or clothing
- Rooting, head bobbing or nuzzling against whoever is holding them
- Fidgting and squirming a lot
- Fussing
- Crying – a late sign of hunger.
Do offer feed generously. A newborn won’t find it easy to feed well, if they have to wait and reached late hunger signs.
Helping your sleepy baby
Positioning and attachment
Getting a deep, comfortable latch is crucial. If your baby is not latched on well at the breast, they will have to work harder to get your milk. They may tire easily and fall asleep. Sometimes just a small adjustment to the way your baby comes to the breast can make a huge difference. An LLL Leader can provide individual suggestions tailored to your circumstances. If your breasts are engorged, gently hand express a little milk and/or ease swelling back with your fingertips to make it easier for your baby to latch on deeply and prevent you getting sore. See our longer article about Positioning and Attachment for more help on how to help your baby latch well, feed effectively and be comfortable for you.
If your breasts are engorged, gently hand express a little milk and/or ease swelling back with your fingertips to make it easier for your baby to latch on deeply and prevent you getting sore. See our longer article about Positioning and Attachment for more help on how to help your baby latch well, feed effectively and be comfortable for you.
Copyright Suzanne Tobin
Seek skilled help early on if you are finding breastfeeding difficult or uncomfortable.
Laid back breastfeeding
Try letting your baby lie on your body with their chest and tummy against you as you recline at about 45 degrees. If they can snuggle up close to your chest for periods of time, even when sleepy or during light sleep, they will often instinctively seek the breast and attach deeply and comfotably even during light sleep. This can be done skin-to-skin or with you and your baby lightly clothed. Watch for signs your baby is stirring and gently encourage feeding.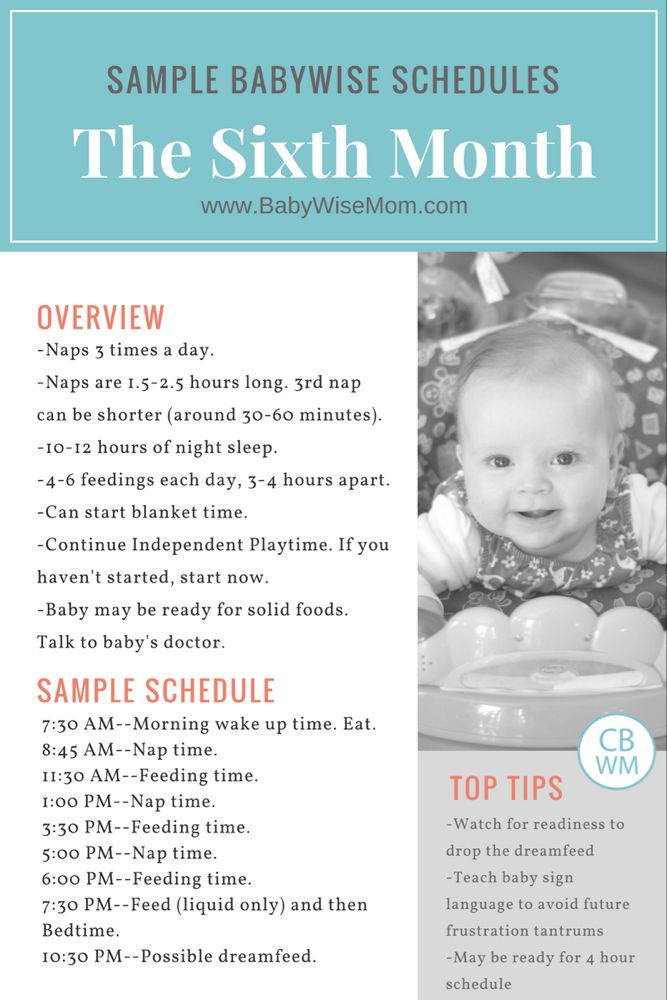 Spending time relaxing like this can make a real difference to how well your baby feeds and how much milk you make. Our page on Comfortable Breastfeeding has more ideas.
Spending time relaxing like this can make a real difference to how well your baby feeds and how much milk you make. Our page on Comfortable Breastfeeding has more ideas.
Breast compression
If your baby starts to doze at the breast, this technique will help him breastfeed actively and take more milk.
- Cup your breast with your hand, near your chest wall, thumb opposite fingers in a C shape. Keep your hand well back from the nipple area.
- Wait while your baby breastfeeds actively, with their jaw moving all the way to his ear. When they stop swallowing, compress your breast firmly. They probably start swallowing again. Hold it squeezed until they stop nursing actively, then release your hand.
- Rotate your hand around your breast and repeat step 2 on different areas of the breast as needed. Go gently—this should not hurt.
Try switching breasts at least two or three times during each feed—when your baby comes off the first breast on their own or when breast compression no longer keeps them breastfeeding actively.
Express milk for your baby
Until your baby gets the hang of feeding you may need to do some work for your baby. If they aren’t latching at all, or is not feeding well and gaining weight, then expressing your milk will help establish milk production. The earlier you start, the sooner you’ll produce plenty of milk. Hand expression is often easiest at first but when your milk comes in combining hand expression with pumping can be most effective.
Giving expressed milk
First, encourage your baby to nurse at both breasts. Watch for swallowing and use breast compression an switch nursing until they stop drinking and start to doze.
Next, give your baby expressed milk until they have had enough. (For more on how to give additional milk, our article here). Giving your baby your expressed milk after breastfeeding can help them overcome sleepiness and feed more effectively next time.
Then, once your baby has settled, express from both breasts switching back and forth and using compressions and hand expression to get the available milk. Store this milk in the fridge ready for the next feed.
Store this milk in the fridge ready for the next feed.
Aim to complete this process within about an hour.
Avoid bottles and dummies
You can give small amounts of expressed milk using a spoon, flexible feeding cup or syringe. If you decid to use bottles for larger amounts, you can give the bottle in a way that helps protect breastfeeding. For more information on ways to give your baby milk and bottles see our article on Bottles and other tools. An alternative is to use a nursing supplement: this acts like a straw to deliver extra milk through a tube along your breast as your baby nurses, avoiding the need for bottles. Our article Nursing Supplementers explains more.
Don’t give up too soon
If your baby doesn’t respond quickly to your efforts to get him to breastfeed more often and more effectively, don’t give up. Keep your baby fed, Keep your supply protected and Keep your baby close. You may find our article on Getting breastfeeding back on track after a tricky start helpful. Check with your doctor to eliminate any medical reasons and contact your local LLL Leader to find one-to-one breastfeeding help. You can find support and encouragement from breastfeeding mothers in your local LLL Group too.
Check with your doctor to eliminate any medical reasons and contact your local LLL Leader to find one-to-one breastfeeding help. You can find support and encouragement from breastfeeding mothers in your local LLL Group too.
Written by mothers of LLLGB. Photos courtesy of Ellen Mateer and Suzanne Tobin.
Further Reading
Comfortable Breastfeeding
Positioning and attachment
Engorged Breasts – Avoiding & Treating
Hand Expression of Breastmilk
Is my baby getting enough milk?
My Baby Needs More Milk
Nursing supplementers
Jaundice in Healthy Newborns
Getting back on track after a tricky start – the Three Keeps
My baby won’t breastfeed
Bottles and other tools
Other websites
Biological Nurturing™: www.biologicalnurturing.com/video/bn3clip.html
Natural Breastfeeding Position video, Nancy Mohrbacher:
Benefits of skin-to-skin contact: www.kangaroomothercare.com
Books
The Womanly Art Of Breastfeeding. LLLI, London: Pinter & Martin, 2010
LLLI, London: Pinter & Martin, 2010
This information is available to buy in printed form from our shop.
Copyright LLLGB 2020
Updated June 2022
Signs of effective feeding in the early days
Most babies are keen to feed in the first 90 minutes after they are born especially if they are in skin-to-skin contact with their mum.
If your baby is too sleepy to take this first feed or needs medical attention, it’s a good idea to ask your healthcare team to show you how to hand express and give the colostrum by teaspoon or syringe. He may sleep for a few hours after this first feed – feel free to cuddle him and wake him if you want to feed. He may feed four to five more times in the first 24 hours.
After that first 24 hours we know that babies who are getting adequate amounts of milk will wake to feed at least eight times over a 24-hour period (10 to 12 times being more likely) so it is valuable to keep an eye on numbers and offer feeds even if the baby does not seem to be actively asking.
Babies need to feed frequently; this encourages your milk to increase in volume. Once your milk is coming in, after about 48 hours or so, you may hear your baby swallowing. You may also notice that your breasts feel fuller and that after your baby has fed they soften a little.
Babies who are excessively sleepy, reluctant to wake or who only wake briefly and suckle for very short times will need some extra milk, and your colostrum is best. Learn how to hand express and give your expressed colostrum frequently, until your baby is waking, keen to latch and is doing active sucking and swallowing, with pauses.
Your baby will be content and satisfied after most feeds and will come off the breast on his own. A period of cluster feeding each day (or night) is common. When a baby is cluster feeding he may be very keen to breastfeed a lot and not want to settle to sleep for three or four hours.
However, if you feel he is never really satisfied after feeds, trust your instincts: some expressed milk might help. Seek help with positioning and attachment so that your baby can learn to extract milk efficiently himself.
Seek help with positioning and attachment so that your baby can learn to extract milk efficiently himself.
You can get support from LLL here.
These videos may help with positioning and attachment:
https://www.youtube.com/watch?v=wjt-Ashodw8
https://vimeo.com/11692547
There are more videos along with images and descriptions in our post: Positioning & Attachment
Keeping an eye on his nappies can help you know if he is getting enough milk
Poos
At first poo is sticky, black, and almost tar like. This will become greenish, less sticky, and wipe off your baby’s skin easier! By day three/four you will notice the poo change colour to mustard yellow, and it will be soft and seedy. Two or more of these poos every 24 hours are a sign your baby is getting enough milk in the early days. After three full days (72 hours) your baby should produce at least three poos per day.
By five to six weeks your baby will develop his own pattern and may go days without a poo. Providing he is gaining weight ok, poos are no longer as important for being confident he is getting enough milk.
Providing he is gaining weight ok, poos are no longer as important for being confident he is getting enough milk.
Wees
At first your baby may not pass much urine but this increases each day. If you have had extra fluids during labour and birth your baby may produce extra urine for the first 24 hours or so. By day two look for two wet nappies over 24 hours, days three and four look for three or more wet nappies each 24 hours. By the time your baby is five days old, wet nappies should be more frequent, usually six or more over 24 hours. If your baby’s urine output is less than this or you see red/orange specks in your baby’s nappy, (these are called urates) your baby could do with some more milk.
It can be tricky to tell if disposable nappies are wet – after five full days, when copious milk comes in, they should be heavy.
Many disposable nappies have a faint line down the middle of the nappy which changes colour when wet.
If you are worried your baby isn’t getting enough milk, consider hand expressing your milk. You can feed the expressed milk by teaspoon, cup or directly into his mouth. With some extra milk your baby will generally start to wake more and feed more actively. If you are concerned that your baby isn’t well contact your midwife or GP.
You can feed the expressed milk by teaspoon, cup or directly into his mouth. With some extra milk your baby will generally start to wake more and feed more actively. If you are concerned that your baby isn’t well contact your midwife or GP.
There is more information in these posts:
Is my baby getting enough milk?
My baby needs more milk
Breastfeeding concerns
Occasionally there is reason to be concerned about a baby’s weight gain or the way he is breastfeeding. Here are some signs that your baby may not be getting enough milk at the breast:
- If your baby has not regained his birth weight by two weeks of age
- If baby is passing less urine and pooing less frequently than described above, or his poos remain dark, then seek additional support and give more milk. Older babies may have bowel movements less frequently
- If baby is nursing fewer than eight to twelve times in 24 hours in the early weeks
- If baby is not waking to nurse at night
- Your baby is never satisfied after feeds
- Breastfeeding is very painful all the way through a feed
- You don’t feel signs of your milk coming in after day three
If you are concerned about your baby or s/he shows any of these signs, seek help with breastfeeding from your healthcare team and La Leche League.
Find LLL support here or call our national helpline on 0345 120 2918.
Any of the following are signs of dehydration and the need to seek medical help immediately:
- less than two wet nappies in 24 hours from the third day
- listlessness
- lethargy
- weak cry
- skin loses its resilience (when pinched it stays pinched looking)
- dry mouth, dry eyes
- the fontanel (soft spot) on the head is sunken or depressed
- fever
This list is not exhaustive and we stress that you should consult your Doctor, Midwife, Health Visitor, or other healthcare provider if you have any concerns about the health of your baby. Breastfeeding support can continue alongside any necessary medical treatment. A La Leche League Leader (breastfeeding counsellor) can provide further information on breastfeeding management. Get LLL support here.
A newborn sleeps a lot and eats little - A newborn sleeps a lot and eats a lot
Almost every woman at the stage of pregnancy imagines how her life will change, what her baby will be like and how their joint days will be organized.
And conceived, the expectant mother builds in her imagination a certain “ideal” picture, supported by media images and commercials - a constantly smiling or sweetly sleeping baby.
Undoubtedly, babies really sleep sweetly and smile with the most sincere smile. But this is not always the case.
THE FIRST MONTH OF LIFE - DONATION
The first month, and even the first three months of a child's life is called the period of "carrying out" - the stage of adaptation of the baby to the outside world, as well as the young mother getting used to new living conditions, to her new role, to the changed rules of life associated with the birth of a baby.
Many young mothers prepared for the birth of a baby already know a lot thanks to the availability of information about the psychophysiology of the newborn.
And, of course, when a mother has information about how much a small child should sleep, she somehow expects this from her baby too.
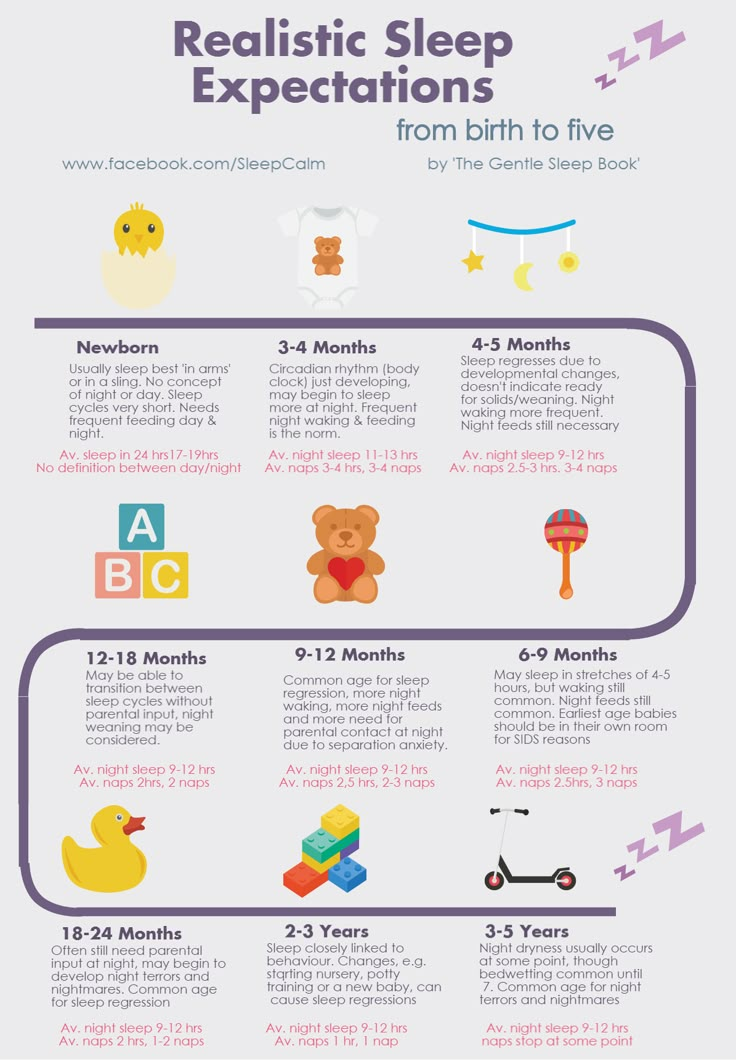
Let us remind you that a healthy full-term baby of the first year of life sleeps about 15-18 hours a day. Of these, 8-10 occur at night and 6-9 during the day. In fact, a newborn baby sleeps a lot of the time - most of the day.
Of these, 8-10 occur at night and 6-9 during the day. In fact, a newborn baby sleeps a lot of the time - most of the day.
The period of wakefulness in a baby from birth is quite short - 20 minutes, increasing by the end of the first month of life to 45 minutes (maximum - up to an hour).
Most of the waking time, especially in the first weeks of life, the child spends with the mother in the process of feeding - when he is awake, he eats.
Breastfed babies need to be fed every 1.5 hours during the day (max 3) and every 3 hours at night (max 5). Such time intervals are due to the small volume of the newborn's stomach and the rapid digestibility of breast milk, the child needs to eat often.
Lack of food for more than 3 hours during the day and more than 5 hours at night is dangerous and fraught with dehydration of the child, and besides, if a small child sleeps without waking up for so long, this is an occasion to more closely monitor his condition and tell the pediatrician about it.

All this information is in the public domain, and after reading it, young mothers experience a whole range of feelings - from surprise to fear and confusion at the slightest deviation from the "norm" if her baby does not fit into them, for example, he is awake a lot and eat a lot or, conversely, eat little.
WHAT IT MEANS "LESS SLEEPING"
Let's take a closer look, because often the concepts of "little" and "constantly" are quite subjective criteria.
- It is important to know that the baby on the breast can sleep while sucking - in this case the baby can sleep, although the mother may identify this period as being awake.
- Hour count. In this case, it is better not to focus on subjective feelings. It often seems to tired and sleep-deprived parents that “the child did not sleep at all,” although if you count the hours objectively, you can find out that this is not the case.
 To calculate sleep time, you can use programs for smartphones, for example, Baby Tracker or any other adapted for these tasks. Recording the baby's sleep hours will help the mother know for sure how many hours he sleeps.
To calculate sleep time, you can use programs for smartphones, for example, Baby Tracker or any other adapted for these tasks. Recording the baby's sleep hours will help the mother know for sure how many hours he sleeps.
VIDEO LESSON
Baby sleep from 0 to 3 months
More
HOW TO KNOW IF YOUR BABY EATS MUCH?
A bit of theory about the physiology of breastfeeding. In the first three months of life, lactation is established in a breastfeeding mother. Milk comes on the 3rd-5th day of a baby's life. During this period, the colostrum that the baby ate immediately after birth changes its composition and becomes early (transitional) milk. During this period, the arrival of milk is still completely controlled by physiology - the endocrine system of the woman's body, it will remain even if the mother does not feed. And it is this period that is extremely important for establishing lactation - it is very important to put the baby to the breast as often as possible so that he eats, and that, thanks to sucking, receptors sensitive to prolactin are established in the mammary gland. On the second or third week (6-13 days after birth), milk becomes late transitional and only by 14-23 days - mature. Thus, lactation gradually shifts from endocrine control to autocrine control (controlled by the frequency of suckling). This means that the more the baby will breastfeed and eat, the more milk he will receive and vice versa - the less often he eats, the greater the likelihood of lactostasis and a decrease in milk in the breast.
On the second or third week (6-13 days after birth), milk becomes late transitional and only by 14-23 days - mature. Thus, lactation gradually shifts from endocrine control to autocrine control (controlled by the frequency of suckling). This means that the more the baby will breastfeed and eat, the more milk he will receive and vice versa - the less often he eats, the greater the likelihood of lactostasis and a decrease in milk in the breast.
Thus, the baby, by frequent sucking, stimulates the mammary gland to produce milk - this is the most important process that is absolutely normal and correct from the point of view of the physiology of the postpartum period of both the mother and the newborn.
WHAT SHOULD I DO IF THE BABY IS ABOVE THE RATE?
What to do if, using observations and time-counting programs, it turns out that the baby is awake more than normal and does not stop breastfeeding.
First of all, it is important to consult with the attending pediatrician and possibly a neurologist to make sure that the baby does not have neurological and physiological health problems.
Many children sleep restlessly and stay awake more than the norm if they had some difficulties during childbirth (entanglement, hypoxia), separation from their mother in the postpartum period, and so on. In this case, they especially need constant contact with their mother in order to sleep peacefully.
It is also important to make sure that the sleeping conditions are organized correctly - the sleeping room is sufficiently ventilated, not hot (no more than 22 degrees), humid enough (50-60%), the baby does not overheat during sleep (comfortable pajamas for the season, no cap ).
HOW CAN YOU HELP YOUR CHILD?
- Recreating the conditions of the uterus - tightness (sleep in a cradle, in a sleeping bag or in a sling), darkness, motion sickness.
- Feeding on demand. At this age, the baby can be fed as often as desired, without adhering to the feeding regimen. He can eat quite often.

- Maximum contact of the baby with the mother (sling helps the mother to have some freedom of action)
- Sleeping next to mum in side crib with side down promotes closeness between mum and baby and is safe.
Tips for worried moms:
Many new mothers often worry about the “norm” and get scared when things don't go the way they should.
- The first recommendation to all new mothers is to ignore the norms, especially those norms that are inherent in the children of girlfriends. Every baby, like every mother-baby couple, every family is unique and what is normal for her is not necessarily normal for you. You will have your own rules. Sleep standards are a guideline. The main criterion is the well-being of your baby. It is important to help him fall asleep not when "it's time", but when you notice his signs of fatigue. Time limits are just a guideline.
- The same goes for feeding.
 There is not and cannot be “too much breastfeeding” in the first month of life. The baby can eat as much as he needs. Establishing lactation is now one of the main tasks. Let nature and the baby make it happen.
There is not and cannot be “too much breastfeeding” in the first month of life. The baby can eat as much as he needs. Establishing lactation is now one of the main tasks. Let nature and the baby make it happen.
- Rest and rejuvenate whenever possible. Fall asleep with the baby, involve relatives, spouse to help.
- Record in memory and on paper your thoughts, emotions, discoveries, impressions The first month of a baby's life will fly by very quickly, even if sometimes it seems that time is slow. Take pictures of the baby, watch his changes, because they happen every day!
If you slightly change the angle of perception of the situation, the newborn period will pass easily and naturally, and the calmer and more relaxed the mother is, the calmer the baby’s sleep will be =)
Food and Sleep Breastfeeding NormsSleep Newborn Sleep
Wakefulness and Sleep
Euromed Clinic pediatric neurologist answers questions
A neurologist is one of the main specialists for children from birth. For the first time, your baby meets with a pediatric neurologist while still in the maternity hospital, then scheduled examinations by this doctor are carried out every month, at three, at half a year, at 9months (if indicated), per year. We talked with the pediatric neurologist of EuroMed Clinic Natalia Petrovna Isaenko about why a child is so often shown to a specialist, what are the most common neurological diseases in babies, and what needs to be done to ensure that your child grows up healthy and calm.
For the first time, your baby meets with a pediatric neurologist while still in the maternity hospital, then scheduled examinations by this doctor are carried out every month, at three, at half a year, at 9months (if indicated), per year. We talked with the pediatric neurologist of EuroMed Clinic Natalia Petrovna Isaenko about why a child is so often shown to a specialist, what are the most common neurological diseases in babies, and what needs to be done to ensure that your child grows up healthy and calm.
— Natalya Petrovna, what does a neurologist pay attention to during routine examinations of babies?
- First of all, the neurologist reveals gross congenital anomalies. Next, we look at how the pre-speech, motor, emotional development of the child goes.
In each age period, the child should have certain skills. Parents, unlike a neurologist, most often cannot objectively assess how the development of their child fits into age norms.
- But after all, all children are different, and their development may not correspond to the tables and the established framework?
— Yes, it happens. Here it is necessary to approach very individually. Indeed, despite the fact that we are guided by existing norms, we have certain tables, painted schemes of what a child should do at what age, there is a possibility of deviations from them, and this is not scary. Some child may begin to perform certain actions a little earlier, some - a little later. Much depends on the conditions in which the child lives, what parents do in relation to the child, etc.
Here it is necessary to approach very individually. Indeed, despite the fact that we are guided by existing norms, we have certain tables, painted schemes of what a child should do at what age, there is a possibility of deviations from them, and this is not scary. Some child may begin to perform certain actions a little earlier, some - a little later. Much depends on the conditions in which the child lives, what parents do in relation to the child, etc.
But that is why it is important to consult a neurologist in order to professionally assess whether the child is developing normally or there are frightening moments that may indicate certain health problems.
Is it normal for a small child to cry often?
- Recently, it is believed that a healthy child, when he is full, who has enough day and night sleep, should not cry. If the child cries often and for no reason, then there is a problem. These can be headaches, neck problems (subluxations, infringement), neurological problems. In the first months of life - problems with the gastrointestinal tract: colic, increased gas formation, etc. In connection with this, there may be crying during meals, refusal of the breast, of the bottle. During eating, intestinal motility increases, and therefore the child experiences discomfort.
In the first months of life - problems with the gastrointestinal tract: colic, increased gas formation, etc. In connection with this, there may be crying during meals, refusal of the breast, of the bottle. During eating, intestinal motility increases, and therefore the child experiences discomfort.
Young children are usually very weather dependent and react to the weather - this can also be a reason for crying.
It seems to me that many children cry because they are bored, they require parental attention so much. Now there is a psychological acceleration in children and, accordingly, they need more attention. This is usually clearly visible. Many parents themselves provoke this fixation: the child began to cry, the mother took him in her arms, shook him, put him to her chest. Of course, the baby in his mother's arms and, moreover, at the breast is fine, and he will repeat crying, demanding repetition. It is not necessary to apply it to the chest every time the child has cried. It is better to try to switch: distract, rattle a rattle, stroke ...
It is better to try to switch: distract, rattle a rattle, stroke ...
Another reason for crying is overwork. Parents often do not believe that the baby can overwork, they do not understand why. Babies have an immature nervous system, plus they receive a huge amount of new information and impressions every day - for them, everything in the world is new and unfamiliar! Therefore, a good sleep is so important, when the child can take a break from impressions.
If the child screams before going to bed, sleeps little, nervously, often wakes up, it is necessary to move the mode, improve sleep, monitor the quality of sleep.
- When we talk about a full sleep, what do we mean, how should a child sleep?
- For very young children, the norm is to sleep for at least an hour and a half on daytime sleep, six hours in a row - at night. During the adaptation period, in the first months of life, the baby may wake up at night more often, but still, the intervals should be at least 3 hours. Sleeping for 30-40 minutes is not enough, the child does not have enough time to rest. Here such a moment is important: the phase of sleep in a child is just these 30-40 minutes. But the child must be able to move from phase to phase independently. What happens in practice? The child was brought in, opened his eyes, his mother immediately takes him in her arms, begins to feed him. He gets used to it and no longer falls asleep on his own. Therefore, it is important to teach the child to move from phase to phase without waking up: do not touch him if he wakes up, do not disturb him; if he cried, was capricious - pump him up, stroke him, but try so that the child continues to sleep without a break for food.
Sleeping for 30-40 minutes is not enough, the child does not have enough time to rest. Here such a moment is important: the phase of sleep in a child is just these 30-40 minutes. But the child must be able to move from phase to phase independently. What happens in practice? The child was brought in, opened his eyes, his mother immediately takes him in her arms, begins to feed him. He gets used to it and no longer falls asleep on his own. Therefore, it is important to teach the child to move from phase to phase without waking up: do not touch him if he wakes up, do not disturb him; if he cried, was capricious - pump him up, stroke him, but try so that the child continues to sleep without a break for food.
Older children who sleep once a day should have 2-3 hours of naps during the day. If you sleep more, that's good.
To improve sleep, the regime is important. I recommend directly writing down in a notebook (or in an application on a smartphone) how much the child sleeps, the time when he fell asleep and woke up, when he screams before going to bed, what his mood is after sleep . .. So we can track the quantity and quality of sleep. Look at what days the child slept well, fell asleep easily - and focus on the daily routine.
.. So we can track the quantity and quality of sleep. Look at what days the child slept well, fell asleep easily - and focus on the daily routine.
- One of the most common diagnoses that many children are given in the hospital is "neurogenic torticollis." How serious is this problem?
- Neurogenic torticollis - asymmetry of muscle tone. A child is often born with asymmetric muscle tone. A small child does not yet have voluntary movements, they are chaotic. And at the moment of relaxation, sleep, the child is drawn to where the tone is increased. That is, the child lies with a certain turn of the head. If you do not deal with this problem, do not correct it, there is a deformation of the neck and skull. The child constantly looks in one direction, lies on one side, as a result, the head flattens, its shape changes.
You can work with this, the main thing is to do it. What is being done to correct torticollis and its consequences? We change position, we shift the child so that he lies on different sides alternately, and not on one, on his back. Lay on the stomach. Also, therapeutic exercises, massage, swimming pool are recommended for the correction of torticollis.
Lay on the stomach. Also, therapeutic exercises, massage, swimming pool are recommended for the correction of torticollis.
Torticollis returns to normal between 3 and 6 months of a child's life. During this period, the child becomes more active, turns his head, arms, begins to roll over, tries to crawl, sit down.
It is important not to confuse neurogenic torticollis, which is treated by neurologists, with congenital muscular torticollis, a gross pathology treated by orthopedic doctors.
Is headaches in children a reason to visit a neurologist?
Yes, definitely. Children under 5-6 years of age should not have headaches - they are not yet ripe for this. In young children, headaches can be caused by somatic causes: parasitosis, anemia, allergies, some problems from the gastrointestinal tract ...
In older children, headaches can be triggered by problems with the spine of the neck. In the pubertal period, various autonomic dysfunctions are often encountered. This is a common problem in teenagers.
This is a common problem in teenagers.
In any case, it is necessary to be examined. There is a good chance that we will not find anything, and the headaches will eventually go away on their own. But it can be a symptom of some serious diseases that should not be left to chance.
Is nocturnal enuresis (urinary incontinence) common? When do we talk about this diagnosis?
Yes, this is also a common disease. As a diagnosis, enuresis is made after 3-4 years.
If we talk about the norms in development, by the age of one and a half years the child should learn not to urinate at night. A modern child spends some time in disposable diapers. Then they are removed. The first time of the night will be "wet". But by the age of two, “dry nights” should already be formed.
After that, some time passes - and the child begins to urinate again at night, say, at 4 years old. This is secondary enuresis.
If the diaper is removed, and the child continues to urinate at night, this is primary enuresis.
There are many reasons for enuresis: these are infectious diseases, malformations, dysfunction of the genitourinary system, immaturity of the nervous system, stress, neurosis, etc. In any case, this problem cannot be ignored, but you need to contact a neurologist as soon as possible for correction this disease.
- Young children have convulsions when the temperature rises. How dangerous is it?
Febrile convulsions (that is, convulsions with an increase in body temperature) is a paradoxical reaction of the nervous system, the cerebral cortex to such an irritant as high temperature. Against this background, there is a splash. Febrile seizures may occur only once, or they may recur with each episode of fever. Most often, they occur in emotional and active children. Special treatment is not required, the main thing is not to allow the body temperature to rise above 37.5 ° C, to bring it down immediately with antipyretic drugs so that episodes of convulsions do not recur. If necessary, the neurologist will recommend sedatives. Such children are observed by a neurologist, it is recommended to see a doctor every six months.
If necessary, the neurologist will recommend sedatives. Such children are observed by a neurologist, it is recommended to see a doctor every six months.
- Can't febrile convulsions be a sign of incipient epilepsy?
As a rule, febrile convulsions do not have a way out into epilepsy. There are isolated cases when convulsions can really be the debut of epilepsy. Therefore, in any case, it is necessary to show the child to a neurologist so that the doctor can see in which direction it develops.
Is epilepsy generally common?
Yes, epilepsy is a common disease. We, in Novosibirsk, even have a special center where epileptologists work - this is a very narrow specialization in neurology. When we confirm epilepsy in a child, I usually refer the patient to an observation center. So there they will be able to help the baby as efficiently as possible, correctly select the drugs and prescribe the correct treatment.
What symptoms should parents pay attention to in order not to miss the onset of epilepsy in a child?
- As a rule, when an attack occurs, it is clearly visible. The child has convulsive twitches, the corner of the mouth twitches, the muscles may pull, saliva flows, foam may come from the mouth, he may urinate. But it happens that a child simply freezes during an attack, and, for example, rubs his hands or makes chewing movements for some time. And then everything passes. After an attack, headache, nausea, impaired coordination and speech can be observed.
The child has convulsive twitches, the corner of the mouth twitches, the muscles may pull, saliva flows, foam may come from the mouth, he may urinate. But it happens that a child simply freezes during an attack, and, for example, rubs his hands or makes chewing movements for some time. And then everything passes. After an attack, headache, nausea, impaired coordination and speech can be observed.
Sometimes the first signs of epilepsy appear even before the attack. For example, a child twitches while sleeping. Or he simply changes his usual behavior, becomes obsessive, whiny, asks the same questions in a circle, etc. This is due to the neurological changes that occur with epilepsy.
Thus, if you notice changes in the child's behavior, he behaves unusually, strangely, be sure to show the child to a neurologist!
If possible, I recommend filming the attack on video - it will be much easier for the doctor to understand what is happening with the child.
- Are there sedatives that can be given to children?
- Hardly ever. Available drugs can be prescribed and given only in hospitals. This is not practiced in outpatient treatment in neurological pediatrics.
Available drugs can be prescribed and given only in hospitals. This is not practiced in outpatient treatment in neurological pediatrics.
With increased excitability and emotionality of the child, I usually suggest starting from afar - to establish a daily routine, give the child the opportunity to actively move and fully relax, walk in the fresh air, etc.
All drugs (vascular, nootropics, etc.) are prescribed strictly according to indications and cannot be taken without a doctor's recommendation. The consequences of uncontrolled medication may be neurological and behavioral problems in the future: hyperactivity, disinhibition, restlessness, attention deficit hyperactivity disorder (ADHD).
How common is attention deficit hyperactivity disorder (ADHD) in children?
Now this diagnosis is made very often. Although, it seems to me, we often attribute to ADHD what it is not: the characteristics of the temperament and character of the child, his activity or even pedagogical neglect . ..
..
There are many pathological hyperactivity, but there are still more stories with problems in the family and in the interaction of parents with the child.
— Another common disease is nervous tics. How are they treated?
Yes, tics are very common. We treat both with medication, and - most importantly - with the normalization of the regimen. For a "ticking" child, a good sleep, rest, minimizing the TV, phone, computer is very important. It is very useful to send such children to sports clubs. As a rule, children suffering from a nervous tic are very emotional, temperamental, read a lot and sit at the computer. They are emotionally and informationally overloaded. And the nervous system relieves tension, manifesting itself in tics.
— Speaking of information overload, how do you feel about early development, which is so popular now?
- Badly. Any neurologist, I think, will agree with me. If a child is given a load that is inadequate for his age and development, this can result in quite serious problems in the future, up to psychiatric disorders. A child does not need all this early reading from two years old, English from three and mathematics from five. The child should calmly explore the world, it is important to stimulate his cognitive activity, but do not stuff him with a huge amount of knowledge beyond his age.
A child does not need all this early reading from two years old, English from three and mathematics from five. The child should calmly explore the world, it is important to stimulate his cognitive activity, but do not stuff him with a huge amount of knowledge beyond his age.
— What are the examinations for the diagnosis of neurological diseases?
- Electroencephalogram (EEG). Invented and created to record epi-activity - to confirm or exclude epilepsy, this is the main focus of this examination.
I also refer children with speech and mental disorders to the EEG to see how all cortical rhythms are formed - by age or not. This is corrected by age, over time. Classes with neuropsychologists, defectologists, the Tomatis method (a program for neuro-sensory stimulation) also help.
Magnetic resonance imaging (MRI). This is one of the most informative surveys.
Be sure to send for an MRI to understand the cause of headaches, especially if the child complains of a headache when moving, when he starts to jump, run, move actively.
Also, MRI is informative in epilepsy, the attacks of which are not treatable. Then we look at the MRI to see if there is a vascular malformation (deviation from normal development) or another vascular defect. This can cause seizures, and the problem is solved surgically. As a rule, after the operation, the seizures in the child stop.
MRI allows you to see the structure of the brain and blood vessels, assess the state of the structure, the presence of cysts, etc.
Computed tomography (CT). Typically, a CT scan is ordered after an injury to look for blood in the injured area.
Ultrasound of the vessels of the neck. Headaches, disinhibition, attention deficit, speech delays can be caused by impaired blood flow through the vessels. Ultrasound allows you to diagnose this, as well as to see anatomical defects (C-shaped, S-shaped course of vessels), anatomically incorrectly formed vessels, improper discharge of vessels into the spinal column, vasoconstriction.