8 month old baby choking on food
Babies Gagging vs. Choking When Starting Solids
Adie, 12 months, gags on a small piece of bread.What is gagging?
Gagging is a natural protective reflex that results in the contraction of the back of the throat to protect us from choking. Just like the reflexive kick that occurs when the doctor taps your knee in just the right spot, the gag happens automatically, initiating a rhythmic bottom-up contraction of your pharynx (the tube that leads to your stomach) to assist in bringing food up and to stop the swallowing reflex from making our bodies try to swallow.
>> Just starting solids? Check out our virtual course (includes videos on infant rescue) as well as our guides and recipes on for the best first foods for baby. And if you are struggling with the transition from spoon feeding / purees to self-feeding with table food, watch our Spoons to Fingers video.
This page has been created with typically developing infants and children in mind. The information here is generalized for a broad audience and is for informational purposes only. If your child has underlying medical or developmental differences, including but not limited to prematurity, developmental delay, hypotonia, airway differences, chromosomal abnormalities, craniofacial anomalies, gastrointestinal differences, cardiopulmonary disease, or neurological differences, we strongly recommend you discuss your child’s feeding plan with the child’s doctor, health care provider or therapy team. The opinions, advice, suggestions and information presented in this article on gagging are for informational purposes only and are not a substitute for professional advice from or consultation with your pediatric medical or health professional. If your child is having a health emergency, please call 911 or your emergency medical resource provider immediately.
Swallowing is a complex reflex with multiple lines of defense built in to prevent choking. These actions happen reflexively, meaning the brainstem tells our body to do them–they are involuntary. There are three important lines of defense that we have with every single swallow.
There are three important lines of defense that we have with every single swallow.
1. When we swallow, our vocal cords, which are like sliding doors inside the breathing tube, come together, closing off the airway and preventing food from entering the lungs.
2. The muscles of the throat pull the breathing tube slightly up and forward, tucking it safely out of the way of the food passing.
3. The epiglottis, a tiny flap of cartilage, tilts down to cover the airway forming a tight seal with the joints that help move the vocal cords.
Just like any good system, we have back up already built in. We even have back up for those back ups that are activated if needed. For example, if anything gets too close to the opening of the airway, even before it gets a chance to get in, the vocal cords immediately close (the technical name for this is the laryngeal adductor reflex), and our body immediately coughs to push the item away from the breathing tube. Our bodies are quite skilled at keeping us safe. 12
12
First, it is important to distinguish the difference between gagging and choking.
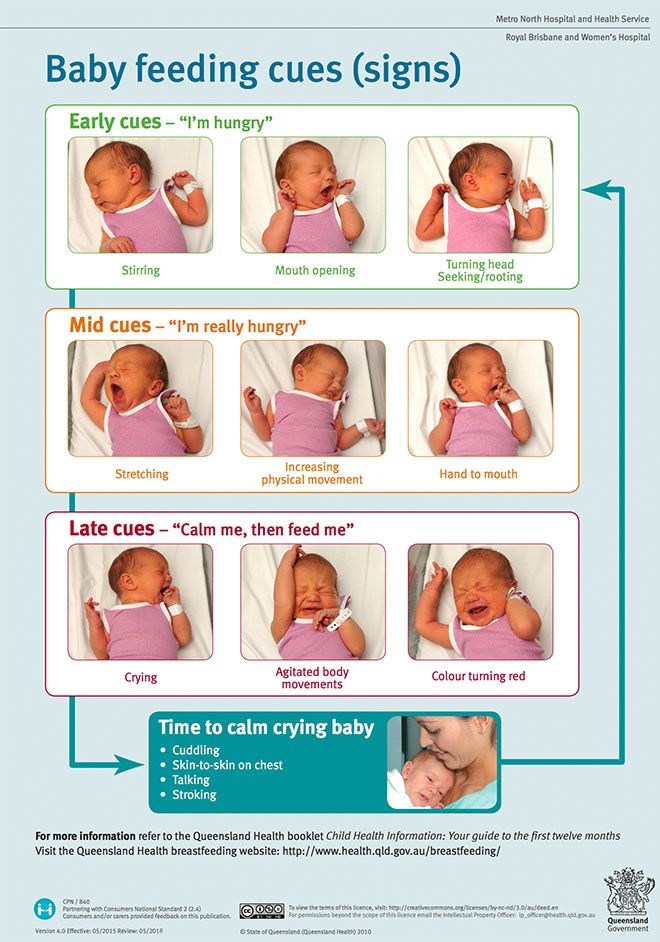
True choking is when the airway is obstructed, and the baby is having trouble breathing. Signs of a baby choking can include:
- inability to cry
- difficulty breathing
- skin tugging into the chest
- look of terror
- high-pitched sounds
- skin color changes (ranging from blue to purple to ashen-like)
If you suspect baby is choking, immediately administer infant choking first aid with alternating back blows and chest thrusts and call 9-1-1 or local emergency services on speakerphone so your hands are free. If another person is present, one person should immediately perform choking first aid while the other calls for help. Conduct age-appropriate CPR if you believe baby’s airway is open, but the child is not breathing.
On the other hand, gagging is a common protective reflex that results in the contraction of the back of the throat. It is a natural function and protects us from choking. When this happens, it’s important to let baby work the food forward on their own. Refrain from sticking your finger in baby’s mouth, which can push the object further down the throat, making the situation worse.
It is a natural function and protects us from choking. When this happens, it’s important to let baby work the food forward on their own. Refrain from sticking your finger in baby’s mouth, which can push the object further down the throat, making the situation worse.
We strongly recommend you take a CPR class online or at your local health facility and review safety procedures. Our choking, gagging & infant rescue video can also help you visualize the difference. Further resources:
- American Red Cross: Child & Baby CPR
- American Heart Association: Infant CPR Training Kits
- Harvard Health: Heimlich Maneuver on an Infant
Gagging is a completely normal reflex in infants, children and adults alike. Gagging is very common and will happen a lot in baby’s solid food journey. All babies gag in their eating journey—it’s one way they learn how to eat. The good news is that babies typically outgrow gagging after a couple of months of practice with various textured foods.
The good news is that babies typically outgrow gagging after a couple of months of practice with various textured foods.
Babies often gag well before they start solids, when breast or bottle feeding. This typically occurs when baby either isn’t properly latched, and the nipple triggers the reflex, or if the baby isn’t ready to swallow milk for whatever reason. Some babies gag when mom’s letdown is too fast. Others gag when they need to catch their breath instead of swallowing. Many babies will gag on a pacifier or certain bottle nipples if they aren’t familiar with them. All of these gags occur because the brain is trying to protect the baby from swallowing an “intruder,” or something the baby isn’t ready to swallow. This gag reflex typically lessens over the first few months of baby’s life when baby gets “desensitized” and learns to accept it (pacifier, nipple, or food texture) without gagging. This occasional gagging at a young age does not seem to bother most infants.
Interestingly, the gag reflex of a 6- to 10-month-old baby is much more sensitive and can be triggered more forward on the tongue than an adult.3 4 This is why babies gag easily: the more forward the gag trigger is on the tongue, the easier it is to trigger.5 It is not uncommon for babies to gag (and occasionally vomit) for the first few weeks of solids. If baby repeatedly gags and vomits past the first month of starting solids, consult your pediatrician, who may refer you to a swallowing specialist.
Watch our video on gagging and all of the other normal, sometimes nerve-wracking things babies do while starting solids.
Cooper, 6 months, gags on applesauce.Ronan, 7 months, gags on a flattened blueberry, spits up some, and carries on eating.Quentin, 8 months, gags and coughs on some bread with avocado. Bread is notorious for triggering gagging as it sticks to saliva on the tongue.Gagging helps prevent chokingWhen the gag reflex is triggered, it forces the back of the throat to close, essentially preventing swallowing. If food caused baby to gag, the reflex forces the food (or object) forward towards the front of the tongue. Young infants naturally open their lips when they gag, which means that typically, the food or object that caused the gag keeps moving out of the mouth.
Gagging is completely normal and incredibly important for baby’s safety, both at the table and away from it.
Gagging helps babies learn to eatFor babies to build the skills for chewing and managing all foods (not just easy-to-chew foods), we need to give them opportunities to make mistakes, like taking a too-big bite of food. When a baby bites off too much food and cannot properly move it around to chew, the gag reflex will kick in and help thrust the food forward. The experience teaches baby that the food was too big to swallow. These experiences are essential for learning and building confidence in biting and tearing. Over time, baby will learn to take smaller bites and become more adept at moving food around to chew properly.
Once baby is a few weeks into their solid food journey, you can use the gag reflex to your advantage. Offer foods that are not as easy to chew to help advance baby’s oral development more quickly. When poorly chewed food touches the tongue, the gag reflex will do its job, and baby will learn they need to chew the food more.
It’s important to challenge baby before they get too accustomed to mashes and soft foods. Babies quickly learn that chewing and swallowing mashes and other easy-to-chew foods easily satisfies their hunger with minimal work. Many babies won’t bother trying to improve their skills with tough consistencies that require more biting and tearing, and may refuse the challenging foods and wait for the easier foods.
Hillis, 6 months, gags on a vegetable purée.Addie, 9 months, gags and coughs on asparagus and successfully moves it forward out of her mouth.Ysabella, 8 months, gags on purple dragon fruitWhy is my baby gagging? Gagging is easily triggeredWhen it comes to young babies, the gag reflex is pretty easy to trigger. Touch the middle of the tongue, and many babies will gag. If you watch a 3- to 4-month-old baby mouthing their hands and fingers, you will see them gagging themselves frequently. This is common and normal. Babies are typically not bothered by it and will often keep doing it.
Our mouths are one of the most sensitive parts of our bodies. The human mouth has many sensory receptors to detect touch, taste, temperature, pressure, and other input types. Babies are driven to explore with their mouths to learn about their world simply because the mouth is sensitive. Mouthing exploration could be very unsafe if babies didn’t have gagging as a natural safety net.
Importantly, young infants have immature hand and finger coordination, which means they can’t easily remove something they put in their mouth. They also have immature oral motor (tongue and mouth) coordination. They can’t easily use their tongue to find an object in their mouth and spit it out. This is another reason the gag reflex is a safety reflex, as it allows a baby to put an object in their mouth and then push it back out again without letting it get close to the throat. As babies put things in their mouth, the gag reflex tells them when things are not supposed to be there and prevents it from moving too far back towards the throat.
The gag reflex moves further back in the mouth as babies ageFrom birth to around 7-9 months, the gag reflex is triggered close to the front of the mouth (around the middle of the tongue). At this age, the gag reflex is as sensitive as it will ever be.6 This is important for safety because objects (food or anything else) will quickly trigger the gag reflex and be pushed out of the mouth before they get past the middle of the tongue.
Sometime around 7-12 months of age, the gag reflex slowly desensitizes. The gag trigger moves from the middle of the tongue to the back of the tongue towards the throat.7 At this point, food or objects can get much closer to the throat before the body recognizes something is too big to swallow and tries to push it back out. This might sound scary, but remember, our bodies are amazing! The gag reflex remains active and strong, so if something (food, barbie shoe, bug, etc.) hits the back of the tongue, the back of the palate (roof of the mouth), or even the back of the throat, the gag still kicks in.
Mahalia, 10 months, gags on some orange stuck to her tongue. If you look closely, you can see the orange isn’t actually all that far back in her mouth, but more on the middle of her tongue. She recovers nicely and carries on eating.Adie, 12 months, gags and coughs on a piece of bread. Bread sticks to the saliva on our tongues easily and can trigger the gag reflex a lot. As you see here, Adie recovers nicely and carries on eating.Babies gag on puréed food and jarred baby food, too
She recovers nicely and carries on eating.Adie, 12 months, gags and coughs on a piece of bread. Bread sticks to the saliva on our tongues easily and can trigger the gag reflex a lot. As you see here, Adie recovers nicely and carries on eating.Babies gag on puréed food and jarred baby food, tooThe threshold for what triggers a gag and the gag’s intensity is different in every baby, but most infants will go through a period where anything in their mouth thicker than breast milk or formula will cause a gag. The brain says: “Wait, this isn’t right! I shouldn’t swallow this! GAG!” Many will gag with spoon-feeding experiences even with runny, watery bland purées.
Until the special day you decide to start solids, baby hasn’t had to manage anything but a watery-thin, fast-moving liquid. Enter something slightly thicker, slippery, and a different flavor — baby’s brain will kick in with protective mechanisms to gag and prevent swallowing this invading purée. This is usually short-lived because thin purées are quite similar to liquids and the texture won’t trigger a gag for very long.
Enter something slightly thicker, slippery, and a different flavor — baby’s brain will kick in with protective mechanisms to gag and prevent swallowing this invading purée. This is usually short-lived because thin purées are quite similar to liquids and the texture won’t trigger a gag for very long.
Babies know to push the tongue against a breast or bottle nipple to initiate suction and move the liquid backward to their throat. Spoon-feeding can present unique oral-motor challenges. With a spoonful of purée dropped on the middle of the tongue, baby has nothing to suck or push against and doesn’t yet know the skills to help move that food backward. Because they can’t move the purée backward quickly, it either continues to sit on the middle of the tongue or will start spreading around the mouth, which can lead to gagging. Many wise babies will suck on the spoon to help them quickly move the purée back to swallow, just like they do from a bottle or breast. Those babies, who now have a way to control the purée, will often easily swallow with minimal or no gagging.
While not all babies who are spoon-fed gag, many do. Not surprisingly, when a baby is exclusively spoon-fed for a prolonged period of time (past 8 months of age, for example), that child may gag more when they start finger foods due to the lack of texture exposure.
Max, 4 months, gags on rice cereal.Levi, 6 months, gags on a vegetable purée. Jai, 6 months old, gags on a squash purée and mom (rightfully) asks her partner not to intervene. Spoon-fed babies gag less at first but gag more later
Spoon-fed babies gag less at first but gag more laterWhen a baby is started on solids with thin, watery purées and pouches, the baby’s tongue receives less sensory input. While babies gag on purées too, they acclimate to the smooth texture or figure out how to use the spoon to suck back and swallow, which reduces gagging. However, all babies will frequently go through gagging periods when introduced to finger foods — whether 6-month-olds or older spoon-fed babies. When baby is first offered finger foods, the brain engages the safety call: “This doesn’t seem right! I don’t know how to move this! We shouldn’t swallow this food!” Often, this period of gagging will last longer with babies who started with spoon-feeding.8
In 2016, the “BLISS” study found that babies who follow a spoon-feeding approach to solids (spoon feeding smooth purées > lumpy purées > finger foods) tend to gag less at 6 months but more at 8 months and later.9 Remember: around 8 months, a baby’s gag reflex becomes less sensitive and moves further in the back of the mouth. This means that food is closer to the throat before the body reacts and tries to push it out.10 In other words, waiting to introduce finger foods until after baby is 8 or 9 months old may increase the choking risk as the gag reflex is less sensitive, further back in the mouth, and baby is not accustomed to textures other than soft foods from a spoon.
This means that food is closer to the throat before the body reacts and tries to push it out.10 In other words, waiting to introduce finger foods until after baby is 8 or 9 months old may increase the choking risk as the gag reflex is less sensitive, further back in the mouth, and baby is not accustomed to textures other than soft foods from a spoon.
By 8-9 months old, a spoon-fed baby has been practicing a very specific skill to eat. “Purées come into my mouth. I suck or lift my tongue to move that puréed food backward, and I swallow it.” Babies will always start with the skill they know and try to use that same pattern on solid foods. They try to move that solid food straight back without the necessary step of moving the food laterally to their gums to chew. This motor pattern often leads to even more gagging.
The older the baby, the more aware they are of gagging and its unpleasantness. A 9-month-old baby is more aware of gagging than a 6-month-old baby. “Hebbian plasticity”—a fancy term that brain specialists use—tells us that neurons that fire together wire together. This means that when one part of the brain lights up simultaneously as another part of the brain, the brain starts to build a connection between those two areas. So, frequently gagging as the baby gets older and more aware of their body may be problematic for some babies who seem to draw a connection between real food and gagging. These babies seem to learn quickly that real food will make them gag and can lead to refusal of any food that is not a purée or mash. By contrast, younger infants don’t seem affected as much as older babies and toddlers.
At 6 months old, the gag reflex is necessary to exploring food. It’s what allows a young baby with almost zero chewing skills to put a piece of food in their mouth and, if it is too big to swallow, get that food safely back out.
Infants learn how to do amazing things—sitting, crawling, walking, and running—by using reflexes, fumbling around, and making lots of mistakes while slowly building strength and adding one movement on top of another. The same applies when learning to chew—babies use reflexes coupled with fumbling as they learn.
The same applies when learning to chew—babies use reflexes coupled with fumbling as they learn.
Amazingly, babies have two other key reflexes—the biting reflex and the tongue lateralization reflex— which help them learn to chew right away at 6 months. For foods to be properly chewed, baby needs to:
- Take a bite.
- Move that food to the side (tongue lateralization).
- Munch up and down to break down the food down.
- Move the food back to the tongue for swallowing.
When babies first start finger food, they will struggle to use their biting and lateralization reflexes in any coordinated way. Simply put, they fumble around! As babies learn to eat, they won’t break down food enough to safely swallow, which requires the gag reflex to push the unchewed food back out. But every time baby does that, they are learning where the food is in their mouth. Slowly and incrementally, babies learn how to move food to different parts of their mouth. They learn their tongue can help push food around the mouth in lots of directions. They learn their palate, tongue, gums, and saliva will break the food down as it moves around their mouth. All of these actions turn a solid food into something like a mash!
They learn their tongue can help push food around the mouth in lots of directions. They learn their palate, tongue, gums, and saliva will break the food down as it moves around their mouth. All of these actions turn a solid food into something like a mash!
Some experts suggest that purees teach babies to swallow correctly, and gives practice swallowing solids before you introduce the idea of chewing. Most babies do not need to be taught how to swallow. Swallowing is a deep brainstem reflex present by 15 weeks gestation2 and well established by full term birth. Babies already know how to swallow; there is no need to practice! Interestingly enough, thicker textures are actually easier for babies to swallow (think purees), and our feeding therapists explain that babies who have swallowing difficulty are actually prescribed thickened milk to drink! But purees do teach baby a motor pattern: bring food in, move it back, swallow. This is a dangerous pattern because most solid foods require chewing before you move them back and can safely swallow. We believe that exclusive purees are time wasted because baby isn’t practicing chewing and is practicing a dangerous motor pattern that must be unlearned.
We believe that exclusive purees are time wasted because baby isn’t practicing chewing and is practicing a dangerous motor pattern that must be unlearned.
Interestingly, the BLISS study also demonstrated that infants who started solids with finger foods experienced more gagging at 6 months, but less gagging at 8-9 months as they developed more control and coordination in moving food around their mouth.11 This demonstrates that babies who are given the opportunity to work with finger foods early on in their solids journey—well before 8 months of age—develop the oral-motor skills required for mature eating more quickly than spoon-fed babies.
After a couple of months, most babies who start with finger foods at 6 months of age develop the skill and coordination to chew and move well-chewed food backward to swallow safely. The baby feels comfortable with their skills and is accustomed to food moving in this way. The body won’t initiate a gag so readily.
By contrast, babies who start solids with purées have had little chewing practice from 6-8 months. It’s likely they are less coordinated with moving food around their mouth, less able to break down the food, and less safe in the instance that the food gets pushed back further in the mouth than they can handle.
It’s likely they are less coordinated with moving food around their mouth, less able to break down the food, and less safe in the instance that the food gets pushed back further in the mouth than they can handle.
 How to help baby move past gagging by building skill
How to help baby move past gagging by building skillSuccessful eating is not just about chewing but about feeling where the food is in the mouth and knowing if it’s chewed “enough” to swallow safely. As adults, most of us can identify and discretely spit out a tiny piece of bone or eggshell from a bite of food. Because this is happening inside the mouth, we aren’t using our eyes; our brains visualize what’s going on inside our mouth, even though we don’t frequently see what’s going on in there. We have a mental image of our mouth and where everything is in relation to other parts. Babies don’t have this “mental map” of their mouth at first.
To help you understand the necessity of a mental map, think about babies learning to stand. Before they can do this, they need to develop “body awareness” or, essentially, a mental “map” of where all their body parts are in relation to each other. Baby lays on the floor and slowly learns to roll around before they ever sit up. Rolling and touching their whole body—from head to toe—while their muscles push and pull helps form the mental “map” of their body. They need deep input all over their body to add all the details to that map. A small touch to one part of their body or a light brush of your hand over their body helps a little but isn’t really enough. It’s the floor’s firm input to the whole body while moving the muscles that really seems to form a clear map.
Rolling and touching their whole body—from head to toe—while their muscles push and pull helps form the mental “map” of their body. They need deep input all over their body to add all the details to that map. A small touch to one part of their body or a light brush of your hand over their body helps a little but isn’t really enough. It’s the floor’s firm input to the whole body while moving the muscles that really seems to form a clear map.
The same goes for the inside the mouth. When things touch the inside of our mouth, a map slowly “draws” in our brain. As babies develops the map inside their mouth, they gain more control, figuring out how to move food around appropriately. They also become more confident in their skill to move food around. This control seems to help quiet the gag response and move it further back in the mouth over time. The baby does not need the gag reflex to eat once they have a clear map and strong coordination. They now have active control to chew the food, know if it’s chewed enough, move it back to swallow, or spit it out and try again.
We know that many types of sensory input in the mouth help babies form the “mental map,” but that bigger inputs are more effective than light sensory inputs. (Think about the difference between a tight hug versus a tickle on the shoulder.)
There are two types of input that feeding therapists know are most effective for sensory-motor learning:
- Touch or tactile input – when food touches a part or many parts of the mouth
- Messages from the muscles and joints or proprioceptive input – when the mouth gnaws on firm or resistive foods that don’t break when chewing.
The simultaneous combination of tactile and proprioceptive input is most effective for forming the map. This is why feeding therapists frequently recommend giving resistive, flavorful foods like a rib bone for baby to chew.
Foods like a rib bone accomplish the trifecta:
- Baby can hold the food, easily put it in their mouth, and pull it back out with their hands, which gives them control to keep the food at the front of their mouth even if they don’t have oral motor control.

- Baby gets big input to their mouth (touch input and muscle feedback as they bite on the bone), which maps the mouth and leads to better control in the future.
- Baby triggers two key reflexes (biting reflex and the tongue lateralization reflex), which mimic chewing and help baby build strength and coordination for future eating.
Are these experiences for eating? No. These are “exercises” to help build a stronger connection between the mouth and the brain. Drawing a detailed map of the mouth contributes to decreasing the sensitivity of the gag. As this map develops, the baby also develops more confidence in their skill, further decreasing the gag’s sensitivity.
Zuri, 9 months, munches on a mango pit. Mango pits are fantastic for working oral-motor skills and low risk as babies cannot bite through them. Quentin, 11 months, works on a spare rib. Spare ribs and even just the bone itself without any meat on it are terrific for helping to map the mouth.Amelia, 10 months, works on a chicken drumstick. For information on how to safely introduce drumsticks, see our Chicken page.Kary Rappaport, a Solid Starts feeding therapist, coaches Reza, 7 months, through a gag on a roasted beet.
Quentin, 11 months, works on a spare rib. Spare ribs and even just the bone itself without any meat on it are terrific for helping to map the mouth.Amelia, 10 months, works on a chicken drumstick. For information on how to safely introduce drumsticks, see our Chicken page.Kary Rappaport, a Solid Starts feeding therapist, coaches Reza, 7 months, through a gag on a roasted beet. Baby gagging on food and throwing up
Baby gagging on food and throwing upGagging with vomit is so hard to watch, though it is pretty normal for some babies just starting solids. Some babies have a stronger or more sensitive gag reflex than others, bringing food up when they gag. This is even more common in babies with a history of reflux. To minimize this reaction, consider these three things:
1. Make sure your baby has at least an hour between a milk feed and table food to let the stomach digest a bit. A super full belly can make a gag turn into vomit much more easily. For example, we often see vomiting with gagging at breakfast, as the belly is super full from a big morning breast/chest feed or bottle.
2. Avoid the foods that tend to trigger the biggest gags for a while. Often, foods that produce lots of gagging are soft, mushy semi-solids like banana and avocado, or fruits and vegetables with skins. These foods can easily stick to the roof of the mouth or tongue and cause strong gagging that leads to throwing up (which often clears the food from the mouth).
3. Offer tons of opportunities for practice with long, resistive, teether type foods (like a mango pit, a spare rib or other thick rib with all lose bits and gristle removed and most of the meat cut off, or a thick pineapple core that does not taper and won’t easily snap or break apart). These foods aren’t for eating, but for helping the brain learn about and desensitize the inside of the mouth. Gagging is the brain’s way of saying “something isn’t right here,” and mouthing these hard, resistive foods that baby can easily pull back out of the mouth helps the brain learn that food isn’t an “intruder.” Mouthing fingers, toys, and infant spoons as teethers outside of mealtimes can also help dampen that gag reflex a bit.
If you try these tips and your baby continues to forcefully gag and vomit at most meals, you may want to mention it to your child’s medical provider.
When to seek helpWe recommend you speak with your child’s pediatrician regarding a referral to a feeding therapist if:
- Baby continues to gag at most meals after an initial learning period (one to two months of finger foods).

- Baby is frequently becoming upset after gagging (crying, tantrums, vomiting).
- Baby is vomiting at most meals, even on an empty stomach.
While it can be disturbing—and nerve-wracking to watch—gagging is a completely normal reflex in infants, children, and adults. Bottom line:
- Babies will likely gag when they first start solids, regardless of starting on purées or finger food.
- Babies who are spoon-fed thin purées are likely to gag less initially but gag more later on when they start finger foods.
- Babies who start with finger foods tend to gag more in the beginning and less later on as their oral-motor skills develop more rapidly.
- All babies gag in their eating journey—it’s one way they learn how to eat. The good news is that babies typically outgrow gagging after a couple of months of practice with various textured finger foods.
Infant CPR & First Aid Resources
One of the most important things you can do to protect baby is take a CPR class online or at your local health facility and review safety procedures. Some resources:
Some resources:
- American Red Cross: Child & Baby CPR
- American Heart Association: Infant CPR Training Kits
- MedlinePlus: Choking First Aid for Infants Under 1
Remember, you are responsible for supervising your child’s health care and for evaluating the appropriateness of the information in this article for your child. Only you know your child and how your child will react to foods and feeding procedures. Although the information presented in this article is based on well-documented research by medical and nutritional professionals, it is up to you to review and consider the information and how it will work with your child.
Always seek the advice of your pediatric doctor, nutritionist or health care provider with any questions you may have regarding a medical condition or feeding issue. You should refer to our Terms of Use for further information.
Reviewed by:
K. Rappaport, OTR/L, MS, SCFES, IBCLC
K. Grenawitzke, OTD, OTR/L, SCFES, IBCLC, CNT
- Matsuo K, Palmer JB.
 Anatomy and physiology of feeding and swallowing: normal and abnormal. Phys Med Rehabil Clin N Am. 2008 Nov;19(4):691-707, vii.
Anatomy and physiology of feeding and swallowing: normal and abnormal. Phys Med Rehabil Clin N Am. 2008 Nov;19(4):691-707, vii. - Nishino T. The swallowing reflex and its significance as an airway defensive reflex. Front Physiol. 2012;3:489.
- Rapley, G., & Murkett, T. (2010). Baby-Led Weaning. The Essential Guide to Introducing Solid Foods.
- Naylor, A. J., & Marrow, A. L. (2001). Infant Oral Motor Development in Relation to the Duration of Exclusive Breastfeeding. Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods, 21–25.
- Isaac, N., & Choi, E. (2018). Infant anatomy and physiology for feeding. In S. H. Campbell, J. Lauwers, R., Mannel, & B. Spencer (Eds.), Core curriculum for interdisciplinary lactation care (pp. 37-55). Burlington, MA: Jones & Bartlett Learning.
- Naylor, A. J., & Marrow, A. L. (2001). Infant Oral Motor Development in Relation to the Duration of Exclusive Breastfeeding.
 Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods, 21–25.
Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods, 21–25. - Naylor, A. J., & Marrow, A. L. (2001). Infant Oral Motor Development in Relation to the Duration of Exclusive Breastfeeding. Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods, 21–25.
- Fangupo, L. J., Heath, A.-L. M., Williams, S. M., Erickson Williams, L. W., Morison, B. J., Fleming, E. A., Taylor, B. J., Wheeler, B. J., & Taylor, R. W. (2016). A Baby-Led Approach to Eating Solids and Risk of Choking. PEDIATRICS, 138(4).
- Fangupo, L. J., Heath, A.-L. M., Williams, S. M., Erickson Williams, L. W., Morison, B. J., Fleming, E. A., Taylor, B. J., Wheeler, B. J., & Taylor, R. W. (2016). A Baby-Led Approach to Eating Solids and Risk of Choking. PEDIATRICS, 138(4).
- Naylor, A.
 J., & Marrow, A. L. (2001). Infant Oral Motor Development in Relation to the Duration of Exclusive Breastfeeding. Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods, 21–25.
J., & Marrow, A. L. (2001). Infant Oral Motor Development in Relation to the Duration of Exclusive Breastfeeding. Developmental Readiness of Normal Full Term Infants to Progress from Exclusive Breastfeeding to the Introduction of Complementary Foods, 21–25. - Fangupo, L. J., Heath, A.-L. M., Williams, S. M., Erickson Williams, L. W., Morison, B. J., Fleming, E. A., Taylor, B. J., Wheeler, B. J., & Taylor, R. W. (2016). A Baby-Led Approach to Eating Solids and Risk of Choking. PEDIATRICS, 138(4).
What You Need to Know
Terrified that baby-led weaning or feeding will cause your child to choke on solid foods? Here’s 8 tips to prevent choking when baby-led weaning, plus a list of foods to avoid.
Want to read this post in a visual way? Check out my Google web story on Top Tips to Prevent Choking when Baby Led Weaning.
Baby-led weaning is a very popular–and now almost mainstream–way to introduce your baby to solids. Essentially, baby-led weaning is skipping purees and spoon feeding altogether and allowing your baby feed herself with finger foods. Your baby eats with you during family meal times–and often even family foods–right from the start, around six months of age.
Essentially, baby-led weaning is skipping purees and spoon feeding altogether and allowing your baby feed herself with finger foods. Your baby eats with you during family meal times–and often even family foods–right from the start, around six months of age.
The potential benefits of baby-led weaning are:
There are many benefits to baby-led weaning listed in my comprehensive guide.
But, won’t my baby choke?
A common concern is that baby will choke on solid foods. Now, choking is serious business, and although it’s very rare, it’s important that you’re aware of common choking hazards and that you are prepared (ie. take infant CPR and First Aid) just in case. But choking gets confused with gagging—which is completely different. Gagging is extremely common when babies are starting solids. The gag reflex keeps larger food pieces out of the wind pipe and near the front of the mouth, only allowing very well-chewed foods to the back to be swallowed. It’s a safety mechanism to prevent choking! And it happens A LOT if you choose the Baby Led Weaning route, especially in the beginning. It’s not a bad thing!
It’s not a bad thing!
Here’s what you’ll find in this post:
- The difference between gagging and choking
- Why it’s important to let baby self-feed
- Why it’s important to always watch your baby while they’re eating
- Why it’s important to use a proper highchair
- List of common choking hazards
- Month-by-month list of appropriate foods (size, texture, shape)
- Avoiding distractions at mealtimes
- Why you should take infant First Aid and CPR
- This is the number one choking hazard (and might surprise you!)
Yet I hear from many moms who want to try baby-led weaning, but are too terrified that their baby will choke on solid foods. Some good news recently came from a new study of 206 babies, called “A Baby-led Approach to Eating Solids & Risk of Choking.” The study compared a group of baby-led weaners (whose parents were given extra education on how to safely practice baby-led Weaning) to a “control” group.
The control group babies mostly started solids using the standard puree method. While the baby-led weaners did gag more at six months than spoon-fed babies, they gagged less by eight months of age. Because by this time, the baby-led weaners had gotten used to eating solids, and the pureed feeders were just starting! And there was no difference in the number of actual choking episodes reported between the two groups.
Gagging – why it’s nothing to be concerned about
Your baby will gag. A lot! Especially in those first few weeks of solid foods and if you’re letting your baby self-feed with finger foods. The best thing to do is to remain calm and cool and encourage your baby to work it out by staying positive, smiling, and NOT PANICKING. This is hard, but really important. If your baby sees you freak out, they might too, and it may possibly turn a normal experience into a scary one.
One common misconception is that gagging is the same thing as choking. Gagging is extremely common when babies are starting solids. In fact, as mentioned above, gagging is a safety mechanism to prevent choking when baby led weaning. Gagging doesn’t usually bother babies; but it does often bother parents! A potential benefit of introducing real foods sooner, is that the gag reflex is further forward in your baby’s mouth. This reflex moves farther back on your baby’s tongue as he ages.
In fact, as mentioned above, gagging is a safety mechanism to prevent choking when baby led weaning. Gagging doesn’t usually bother babies; but it does often bother parents! A potential benefit of introducing real foods sooner, is that the gag reflex is further forward in your baby’s mouth. This reflex moves farther back on your baby’s tongue as he ages.
In contrast to gagging, choking occurs when the air tube is blocked. If your baby bites off a perfectly round shaped piece of hard food, it is possible they will choke. But there’s a lot you can do to prevent it…
Here are my top eight tips to prevent choking when baby-led weaning:
1. Let your baby self-feed
If you put food into your baby’s mouth, it may immediately fall to the back of your baby’s throat, without having a chance to control it with their tongue and chew it. In the study quoted above, a total of three out of 206 babies choked to the degree they required emergency health care assistance. Of these three babies, two choked on milk and the third choked when food was placed in its mouth. Moral of the story? Never put a piece of food into your baby’s mouth.
Moral of the story? Never put a piece of food into your baby’s mouth.
Your baby might enjoy experimenting with a self-feeding spoon. It’s also going to be a messy learning experience, so you may want to stock up on bibs!
2. Watch your baby while they eat
While you can hear your baby gagging, you can’t hear them choking. Choking is often silent, which is why it’s so important that you sit down and eat with your baby. Don’t continue preparing food, do the dishes or go put a load of laundry in. I know that it’s tempting to multitask (I really do!), but when baby is learning how to eat, it’s important to be there to supervise and facilitate a positive and safe experience.
3. Use a proper high chair
It’s important to make sure that your baby is comfortable and secure in their highchair (I love this feeding highchair!). Their feet should ideally be resting on a firm surface and their legs should be bent at a 90 degree angle. This helps to make sure that baby is focusing more on eating and less on keeping their bodies upright and balanced (and prevents a very wiggle baby!). And unless there’s a risk of your baby falling or climbing out, I preferred not to buckle the high chair with my babies. That way you can get them out quickly, if needed. Make sure baby is sitting upright, and not in a reclining position.
And unless there’s a risk of your baby falling or climbing out, I preferred not to buckle the high chair with my babies. That way you can get them out quickly, if needed. Make sure baby is sitting upright, and not in a reclining position.
4. Don’t offer food in choking-hazard size
Your baby’s air pipe is about the width of one of their finger nails, so it’s important to serve thinly sliced foods. Avoid round items like whole grapes, cherries, nuts, berries, cherry tomatoes and wieners. Instead, slice them in halves or quarters.
Things like big gobs of peanut butter, popcorn and stringy fruits and vegetables are also choking hazards. For harder fruits and veggies, I like to cut them in the shape of a potato chips: long enough for a beginner to grasp, but thin so that choking isn’t likely.
Here’s a full list of potential choking hazards:
- Hard vegetables raw, such as cut baby carrots or raw beets
- Firm fruit with and without peels
- Chunks of firm meat or cheese
- Fruits with pits or seeds (that haven’t been removed), like a whole plum or peach
- Whole grapes
- Popcorn
- Marshmallows
- Whole nuts
- Fibrous and stringy foods like celery, pineapple, or asparagus
- Hard candies, mints, or cough drops
- Fish with bones
- Snacks with toothpicks or skewers
- Whole hotdogs or sausages
Alternative ways of serving:
- Steam vegetables and fruit.

- Peel and grate hard vegetables and fruit like carrots, parsnips, apples, and zucchini.
- Grate cheese.
- Always remove pits and seeds from fruit.
- Slice grapes into lengthwise halves or quarters.
- Thinly spread peanut butter or any other nut or seed butter on toast.
- Debone fish.
- Serve fresh, frozen, or canned (rinsed) corn instead of popcorn.
5. Offer appropriate size, texture and shape of food
Through the ages of 6 to 12 months, you can expand the textures and sizes of foods that are suitable to serve. As babies grow, they slowly develop more mature chewing and swallowing skills, as well as better finger dexterity and fine motor skills. This helps them handle firmer, smaller pieces of food. As you watch your baby eat, you will notice changes in the size of pieces that they can pick up.
In terms of texture, it’s important to steam fruits and veggies and test the foods to make sure you can mash them with your tongue on the roof of your mouth, especially in the beginning. It’s much easier to cough up a piece of soft food, than hard food!
It’s much easier to cough up a piece of soft food, than hard food!
Every baby develops at a slightly different rate, and that’s okay! While one baby might be ready to pick up small peas and blueberries by 9 months, another might not be ready until 11 months. These suggestions are just a loose guideline of which textures and sizes of food to offer at each age and stage. Of course, pay close attention to your own baby to know what’s right for them.
As your baby becomes a more confident feeder, move to the next stage. By the time they turn one, your baby will be self-feeding like a pro—you got this!
6 TO 7 MONTHS
Protein/iron-rich:
- Meat and poultry: Minced; pureed; slow-cooked and shredded; or meatballs or patties
- Low-mercury fish: Deboned, then soft-cooked or pureed fish
- Eggs: Hard-boiled and mashed; omelets cut into strips; or scrambled
- Legumes: Cooked and mashed or pureed beans, lentils and chickpeas.
 Silken or mashed firm tofu
Silken or mashed firm tofu - Cheese: Thinly sliced or grated
- Nut butter: thinly spread on toast strips; or stirred into infant cereal
Fruits and vegetables:
- Soft fruits: Peeled and cut into large strips – try avocado or ripe pear.
- Bananas: Leave half the peel on to help baby’s grip
- Hard fruits and vegetables: peeled and steamed until soft, then mashed or pureed, or cut in large strips as finger food. Try green beans, carrots, zucchini or apples
Grains:
- Whole grains: Cooked and spoon-fed quinoa or oats.
- Whole grain bread: Toasted and cut into strips.
- Iron-fortified infant cereals: Mashed with breastmilk or formula .
8 TO 9 MONTHS
Continue to serve any of the foods from 6-7 months, and progress to these textures when your baby seems ready:
Protein/iron-rich:
- Meat, poultry and fish: Medium-sized, soft-cooked pieces.

- Legumes: Lentil or bean patties (see my homemade lentil patties here).
Fruits and vegetables:
- Soft fruits: Medium pieces of soft or steamed options such as raspberries , kiwi, or peach
- Raw vegetables and fruits: peeled and grated apple or carrot
Grains:
- Large-flake or steel-cut oats: Thicker than baby’s first iron-fortified baby cereals
- Pasta: Bite-size cooked shapes, such as penne or macaroni
- Firmer grains: Farro or barley
10 TO 12 MONTHS
Continue to serve the foods above, and progress to these textures when your baby seems ready. Now that baby has better dexterity, pieces can be smaller.
Protein/iron-rich:
- Meat, poultry and fish: Smaller pieces of pulled roast chicken
- Legumes: Cooked whole beans or lentils and cubed firm tofu.
- Dairy: Cheese cubes.
Fruits and vegetables:
- Hard vegetables: smaller pieces of raw peeled cucumber or steamed carrot coins
- Dried fruit: Cut apricots or whole raisins.

- Fruits: Raw small pieces, such as sliced grapes and small whole blueberries
Grains:
- Pasta: Offer as part of mixed meals, such as ravioli, spaghetti and meatballs, or soup.
6. Don’t let your baby play with toys or watch TV during meals
Your baby needs to focus on learning the new skill of eating. And a distracted baby is more likely to choke! Remove all distractions, including toys and screens.
7. Take an infant CPR class
Chances are, your baby will be fine and not have a choking episode, especially if you’re following the tips above! Despite this, before anything else, this is priority number one. Make sure you take a baby first aid and CPR training course. Find one through your local hospital, public health center, or community center. It’s so important to be confident and knowledgeable about how to react in an emergency like choking way, you are confident in dealing with choking if it does happen.
8. Be careful with this one food, in particular
The #1 most common food that Baby-led Weaners choke on is full apples. I suggest serving apples peeled, sliced thinly and steamed for beginners. Once your baby is older, you can use a cheese grater to grate hard foods like apples. Here’s a great Flourless Oatmeal Apple Muffin recipe to try too!
I hope that these tips to prevent choking help you feel more confident in using Baby led Weaning!
Commonly Asked Questions About Choking and Baby-Led Weaning
How can I help a choking baby?
Prepare yourself by taking an infant CPR and first aid training course. Find one through your local hospital, public health center, or community center.
What are the benefits of baby-led weaning?
It’s important to know that there is no single “right way” to introduce solids to your baby, whether you want to start with traditional spoon-feeding or try baby-led weaning). There are many potential benefits to baby-led weaning, including improved dexterity, early oral-motor skill development, self-regulation, ease for parents, decreased picky eating and more.
There are many potential benefits to baby-led weaning, including improved dexterity, early oral-motor skill development, self-regulation, ease for parents, decreased picky eating and more.
What are the best baby-led weaning foods?
Safe finger foods include: pieces of soft-cooked vegetables and fruits; soft, ripe fruit such as banana; finely minced, ground or mashed cooked meat, deboned fish, and poultry; grated cheese; and whole grain toast strips with a thin layer of butter or nut butter. More baby-led weaning tips.
Food to Grow On
Food to Grow On is the definitive guide to childhood nutrition, packed with practical advice to support you through pregnancy, and up until your little one starts school.
Laid out in an easy-to-navigate question and answer style, this book provides practical advice and support from Sarah Remmer and Cara Rosenbloom, two trusted registered dietitians (and moms). Food to Grow On is packed with hard-earned parenting wisdom and the very latest research in pediatric nutrition, so you will feel supported, understood, and ready to help your child thrive.
Buy Food to Grow On!
Did you know that we offer personalized nutrition counselling for kids and families? If this is something you’d like to learn more about, please visit The Centre for Family Nutrition.
*This is a guest post was originally written by guest dietitian and writer Jennifer House, RD and then revised by Sarah Remmer, RD
What to do if a child chokes
It is impossible to control 100% of all the actions of the baby, therefore, cases when children get something into the respiratory tract or they choke on something often occur. Most often, parents do not need to take any action, because. the child's body is able to independently get rid of a foreign object with the help of a cough. A sign that the airway is not blocked is that the child may cry and/or call for help. Then you just calm the baby and keep the situation under control.
Signs that intervention is needed?
- eyes wide open in panic
- he cannot utter words, cry and scream, or does it quietly and wheezing
- there is increased salivation
- baby opens mouth wide
- skin turns red and then turns blue
- older children may hold their throats
- loss of consciousness
The first thing to do is to call an ambulance. It is advisable to have someone else do this so that you can immediately begin to provide first aid.
It is advisable to have someone else do this so that you can immediately begin to provide first aid.
First aid for children under one year old
As a rule, infants choke while eating or drinking due to incorrect posture.
Your possible actions:
1. Raise the baby's hands up. Despite its unusualness and simplicity, this method helps to normalize the breathing process by expanding the airways.
2. Put the child on your hand with your stomach down and make five pats between the shoulder blades with the edge of your palm.
3. In the case when the baby choked on a small object, it is necessary by the child's legs so that the head is down and also pat between the shoulder blades
4. Tilt the body of the child down, press on the root of the tongue, thereby causing vomiting.
5. If the baby choked on the liquid and began to cough, choke with a cough, breathe noisily, and also in case of a solid object getting stuck, it is necessary to turn it with its back to you, hug your hand while pressing it on the stomach area, tilt the child forward and pat on the back, as described in the first paragraph.
If there are no signs of improvement, lay him on his back so that his head is lower than his torso. Place your middle and index fingers under your baby's breastbone. Do five pressures to a depth of 1-2 cm, making sure that after each of them the baby's sternum straightens without removing the fingers. You should alternate pressure and pats on the back until the doctors arrive. After each pop, check to see if the airway blockage has been cleared.
Attention! All pressing and patting should be gentle but sharp!
You can find on the Internet a recommendation to check the child's larynx with your finger and, if possible, remove the stuck object. Such advice is useful if the foreign object is something soft, such as cotton wool. In other cases, there is a great risk of aggravating the situation by accidentally moving the subject even further.
First aid for a child older than one year
Remain calm so as not to aggravate the child's panic.
You can use the above methods for older children as well. 5 point will differ by the posture of the child. See picture below:
Also for children aged from a year (in no case for children younger!) The Helmich method is effective. The sequence of your actions will be as follows:
- stand behind the baby, you can kneel if his height is still small
- clench the hand of one hand into a fist and place the thumb inside between the ribs and the navel of the child
- clasp the fist with the palm of the other hand
- spread your elbows to the sides and press on the child's stomach from the bottom up
- continue until the foreign object is out of the respiratory tract
If the child's breathing has stopped
If the child's breathing stops during removal of the foreign body and does not resume after removal, this may be the result of a spasm in the throat due to stress. Breathing resumption method:
Breathing resumption method:
- lay the child on its side on a flat hard surface
- tilt head back a little
- lift chin
If the attempt was unsuccessful, it is urgent to start performing artificial respiration and chest compressions. How to do this can be read, for example, here.
Even if you managed to solve the problem on your own, you should definitely consult a doctor to check if the baby has damaged the airways.
What should I do if my child chokes?
What to do if the baby is choking? Everyone needs to know this. And if this happened, it is dangerous to waste time, every second counts here. But let's start with what you don't need to do.
Useful and useless measures
The potential danger for the baby is often formed by his mother and father. Teeth are cut, and the baby strives to gnaw on all the objects that it can reach. What is the point of giving foreign objects to gnaw - it is much more logical to give the baby something edible, useful. For example, a piece of banana, apple or cucumber. This is the point of view of some parents. The child is under supervision - what can threaten him? But trouble can happen in the blink of an eye.
For example, a piece of banana, apple or cucumber. This is the point of view of some parents. The child is under supervision - what can threaten him? But trouble can happen in the blink of an eye.
If at least the top of a milk tooth has hatched in a baby, he will certainly bite off at least a small crumb from the fruit. He was delighted, frightened, inhaled sharply - and now the fool choked on food.
Slightly older babies can be harmed by small fragments of toys - because they need to taste everything. Yes, and during a normal meal, a child can form and make a voice, laugh, whimper - and choke. A typical situation is when an ordinary candy becomes the cause of such an incident.
- In other words, in no case do not neglect the age restrictions indicated on the toys;
- the baby should not touch things from which a small part or detail can be separated;
- as early as possible wean him to give voice during meals;
- do not let the baby play or fall asleep with candy in his mouth.
Despite any preventive measures, one should never relax and one must constantly be vigilant. If the baby choked and it became difficult for him to breathe, you can’t hesitate, we begin a set of urgent measures.
Procedure for choking a baby under one year of age:
- you should raise the handles up - thereby expanding the airways a little, it will become easier for the child to inhale and exhale;
- if breathing is not restored, we put the baby face in the palm, lifting his ass a little higher than his head. Slightly patting on the back, successively directing these claps from the pelvic region to the back of the head. Then the child needs to be turned over, and the butt is still above the level of his head, and lightly press on the sternum 4-6 times, trying to force the fluid out of the lungs. These techniques should be repeated until free breathing is fully restored.
- if the reason that the baby choked was food, you should gently lift him up, holding his legs or stimulate the child to vomit by pressing a finger on the root section of his tongue.
If a foreign object is in the airways, preventing the child from crying and raising a voice, if he waves his arms and pulls in his tummy, immediately call the emergency medical service, before she arrives, you need to do this:
- When the liquid became the cause, the baby has a cough and shortness of breath, take the child with his back to you, hugging and pressing on the tummy near the stomach, tilting the baby, pat him on the back.
- If this does not work, put the baby on the back with his head below the body. Place your middle and index fingers under the baby's breastbone and apply pressure five times. Make sure your chest expands after each press.
- If the cause of the accident was a small solid object (bead, part from the designer), lay the child on his tummy over your arm, placing his head below the torso. With the palm of your other hand, lightly tap on the back. You can also lift the child by the legs to also pat on the back.
- Combine the above techniques, controlling whether the foreign object came out. If you did everything right and this object appeared in your mouth, carefully remove it from there.
If you did everything right and this object appeared in your mouth, carefully remove it from there.
- If these techniques do not give the desired result, artificial respiration should be started. For babies up to 8 months of age, it is done immediately both in the nose and in the mouth. Here you do not need to tilt your head back, just slightly raise the child's chin.
Exhale 3-5 times and make sure the baby's chest expands. If this happens, then the baby can breathe. Take a few more breaths to help the child return to a normal breathing rhythm.
All movements must be done in no way abruptly, without effort. Overdone, you can injure the baby and harm him even more.
What NOT to do when the baby is choking
If this happens, then the most important thing is not to lose your cool and determine whether you need to call emergency medical care. Mom's commotion will frighten the child much more.
For example, choking, the baby retains the ability to breathe in and out. He cries, screams. In this case, you do not need to tap him on the back: let him clear his throat, after which the child needs to be reassured.
He cries, screams. In this case, you do not need to tap him on the back: let him clear his throat, after which the child needs to be reassured.
If a foreign object is in the airways, it is strictly forbidden to pat the child on the back when he is in a vertical position. In this case, it can be harmed by involuntarily pushing a foreign object much deeper. In such a situation, it is necessary to tilt the head and body of the baby.
Remember the strict requirement: in any case, do not try to remove the stuck object on your own! You can make the child much worse, and his breathing can be completely blocked. In this case, you need to call the "ambulance".
Measures to help babies over one year of age
You need to start with one thing: no panic! One-year-old children and older are already well aware and perceive the emotions of their parents. And with your unbridled panic, you can alarm the child too much.
In essence, the measures of immediate assistance to infants of this age category approximately coincide with the methods of assistance to infants. If a foreign object or food crumbs gets into the larynx, lift the baby, firmly grasping the legs, or stimulate his gag reflex. However, in most cases, the child manages to cough without outside help.
If a foreign object or food crumbs gets into the larynx, lift the baby, firmly grasping the legs, or stimulate his gag reflex. However, in most cases, the child manages to cough without outside help.
But if the situation turned out to be more complicated and the above measures did not give the desired result, then the procedure is as follows. You need to put the baby face up on the crib. Press under the ribs into the upper abdomen, pushing up slightly, repeat several times. These movements stimulate the movement of a foreign object back into the oral cavity.
Often another method is used. The child is in front of you, with his back to you. Place your palm on his chest so that the baby rests on your arm. His body should be slightly tilted forward. With the other hand, tap on the back between the shoulder blades 4-5 times.
In the event that a foreign object has become the cause of the accident, it is also recommended to use the direct aid method for suffocation, developed by the American surgeon Henry Heimlich. This technique includes two different ways of helping, depending on whether the patient is conscious or not.
This technique includes two different ways of helping, depending on whether the patient is conscious or not.
First way
Standing behind, clench your right hand into a fist, on top - the left. Press vigorously with the fist of your right hand on the area under the ribs above the navel, directing the movement from the bottom up, towards the sternum, while the arms are bent at the elbows. Continue until then. Until the subject exits and breathes back. This method is suitable for babies from the age of one.
Second way
Lay the child face up and place the hands in the same way as in the first example. With vigorous movements, push up towards the diaphragm until the victim resumes independent inhalations and exhalations. If these efforts fail, artificial respiration and chest compressions may be necessary.
These exercises should be done until the foreign object returns to the oral cavity. This method does not apply to babies under 1 year old.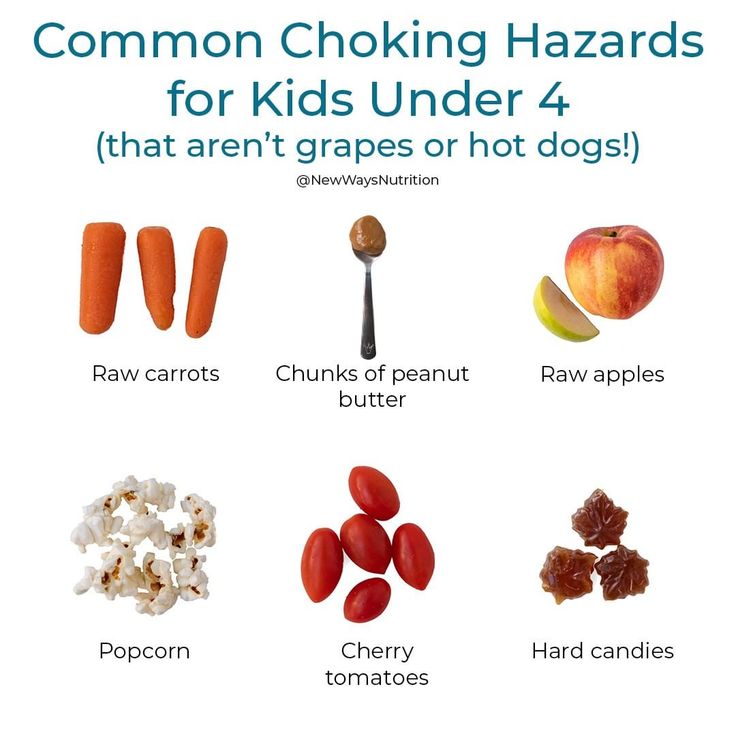
Baby is choking and not breathing: what to do
When the child chokes, it is likely that breathing stops due to spasms in the larynx. The most common cause of them is a stressful situation for the child.
The order of urgent action in such a situation is as follows:
- you need to lay the child sideways on the table;
- slightly tilt your head back;
- slightly raise your head by the chin.
If breathing is not restored, begin artificial respiration immediately:
- in the same way, put the baby on the table;
- take the head back and open your mouth;
- make sure there are no foreign objects in the oral cavity;
- exhale into the child's mouth for a long time;
- repeat 3-4 times. If the chest expands, then you have achieved the desired result, the air enters the lungs of the child. If the baby's chest is immobile, then take urgent measures to eliminate obstructions to breathing;
- after this, we place one palm on top of the other on the child's chest and press sharply - the chest should straighten out each time;
- alternate this massage and exhalation into the mouth at least 16 times.
What to do when the baby chokes
This can happen in various circumstances: bathing in a bathtub, splashing in a summer inflatable pool or in a pond, falling into a pond, or accidentally inhaling liquid while drinking. Measures to save a choked baby must also be taken as quickly as possible:
- Place the baby on your thigh prone, lowering his head below the body, and press on his back. By doing this, you will help eliminate water from his respiratory tract.
- Make sure that there are no foreign objects or vomit in the child's mouth.
- Following this, it is necessary to take measures, according to the basic requirements:
- Respiratory patency should be achieved. The baby lies prone, his neck is not bent, the lower jaw is advanced, the tip of the tongue is retracted. We massage the heart, do artificial respiration.
If we do everything as it should be, then we observe the rhythmic movement of the breathing baby's chest. If these regular movements are absent, but the abdomen is swollen, then breathing does not occur.
If these regular movements are absent, but the abdomen is swollen, then breathing does not occur.
For every couple of exhalations, press the chest 15 times. Toddlers up to one year of age should do these movements with two fingers, and only starting from a year old can you use your palm. Pressing forces should be applied on the sternum in the area between the nipples.
Having brought the baby to consciousness, in no case do not refuse his examination in a medical institution. Such an incident may have further undesirable consequences - for example, pulmonary edema within 3 days after the water has entered the respiratory tract.
When your baby accidentally chokes or chokes, you will not have the opportunity to study the advice of professional pediatricians on the Internet for your situation. There won't be a second to lose. Not only health, but often the life of the child will depend on the speed and effectiveness of your measures. And the best thing you can do now for your child is to learn the most important first aid skills in advance so that when faced with an unexpected incident, you do not panic.