Baby getting tired while feeding
Baby Falling Asleep at the Breast? These 5 Tips Can Help!
Most newborn babies will wake regularly and frequently to breastfeed. However, there may be times when your newborn baby needs to be awakened to breastfeed.
For example, there may be medically indicated reasons why a baby may need to be woken to feed such as Jaundice, congenital heart disease, illness or your baby may not be gaining adequate weight...
Share this content
Is Falling Asleep at the Breast Normal?
Babies are biologically programmed to fall asleep at the breast. Falling asleep at the breast is a normal behaviour and is mostly due to a hormone called cholecystokinin or CCK. CCK makes your baby feel full and sleepy and it is released in your babies gut as soon as they start sucking.
Younger babies generally have higher concentrations of CCK which can make it harder to keep them awake during a feed. This is a perfect system if your baby is waking frequently and feeding well but for the baby who is needing to be woken or to be encouraged to feed it can be a challenge.
So how do you keep a sleepy baby awake at the breast? There are some simple but effective things that you can do to help
Try Skin-to-Skin Contact
Keeping your baby in the skin-to-skin position can help ignite your baby’s natural feeding instinct and encourage them to feed. After all, if you are in the kitchen, you want to eat! Babies can easily find the breast in this position and may spontaneously feed.
Skin-to-skin contact also allows you to notice subtle feeding cues that otherwise may be missed. Your baby may only make a slight wiggle to signal to you that they are ready to feed and if you are holding them closely on your chest you are more likely to notice.
Learn Your Baby’s Early Feeding Cues
Understanding your babies feeding signals and feeding them when they are showing early ready to feed signs can help them to feed better. Check out the Australian Breastfeeding associations Feeding cues article for pictures of early and late feeding cues.
Check out the Australian Breastfeeding associations Feeding cues article for pictures of early and late feeding cues.
Compress Your Breasts
While your milk is flowing your baby will be actively sucking but once the flow of milk slows down your baby may slow down or stop sucking altogether. By gently compressing your breasts you will be encouraging your milk flow to continue… and this can help your baby to begin sucking and swallowing again. Read more tips on helping your breast milk flow.
Dr Jack Newman demonstrates breast compressions in this YouTube clip:
Switch Sides
Your breasts work simultaneously, so, when you are feeding on one breast, the other side is also experiencing a letdown.
Once your baby begins to fall asleep, switch sides so that there is a fresh supply waiting for them. You can repeat this several times (switch back and forth between breasts) because you have more than one letdown per feed.
Changing breasts can make it easier for a baby to fill their tummy when breastfeeding. You can also mix it up by switching sides and use breast compressions together
Use Gentle Stimulation
If your baby falls asleep and stops feeding (it's possible for babies to continue feeding while they are sleeping), gently stroking their hands and feet can stimulate them to stay awake for longer.
Sitting your baby up and giving them a gentle back rub can also help to wake them up and it gives them the opportunity to expel any trapped wind that they may have. If that fails, changing your babies nappy mid feed can rouse them enough to feed some more.
Babies are all different and all feed in different ways so what is “normal” for one baby may be different from another. If you are concerned about any aspect of feeding it is essential that you seek help early and it is always important that you follow your health practitioner’s advice.
As a general rule, if your baby is having at least six very wet cloth nappies or at least five very wet disposable nappies of pale urine, 3 or runnier bowel actions in 24 hours then you can be assured that your baby is getting enough milk.
For more information contact:
- Your General Practitioner
- An International Board-Certified Lactation Consultant
- Your Maternal Child Health Nurse
- The Australian Breastfeeding Association
Have you ever had a baby that always seemed to fall asleep at the breast? What did you do to improve the situation? Let’s have a chat and support each other here or on the Medela Australia Facebook page.
What to Do If Your Baby Falls Asleep While Nursing
When you have a new baby, you often get a lot of warnings about how your little one — and you! — will sleep. But you may be surprised to find that in the first few weeks of your baby’s life, they do almost nothing but sleep. In fact, many newborns will spend the majority of their 24 hours snoozing.
This may seem like a good thing, and in most cases, it is. Enjoy these sleepy days while they last! But sometimes your baby ends up sleeping so much that they can’t seem to get in a good feed. This is especially true for breastfeeding or chestfeeding babies, who have to actively work to extract milk than their bottle-fed counterparts.
This is especially true for breastfeeding or chestfeeding babies, who have to actively work to extract milk than their bottle-fed counterparts.
If your baby can’t seem to stay awake to get a full feeding session in, you likely have concerns. You may be wondering what you can do to keep them awake, if there’s anything wrong with your baby, or if all the sleeping is a sign that feeding isn’t going well.
Let’s take a look.
It’s common for newborns to have days or even weeks when they’re very sleepy and hard to keep awake. Your baby is adjusting to life outside the womb, and this adjustment can be tiring. Plus, your baby may still have their days and nights mixed up, causing them to sleep a lot during the day when you’re ready to feed them.
Luckily, in most cases, “sleepy at the breast” babies don’t stay that way for many feeding sessions in a row or for that long. Most sleepy babies will usually get in enough feeding sessions during a day, even if they have a few sleepy feedings sometimes.
In general, if your baby has enough dirty and wet diapers (usually four to six wet diapers and three to four poopy diapers per day) and is putting on weight at a healthy pace, there’s nothing wrong with them having a couple of sleepy, less vigorous nursing sessions every now and then.
Even falling asleep at the breast is usually fine. In fact, many babies will fall asleep after getting in a good feed. A full tummy makes babies tired, and falling asleep is a natural reaction.
Some babies empty the breast in just a few minutes and fall asleep satisfied. You can usually tell that your baby has had enough when:
- you’ve heard gulping or swallowing while nursing
- your breast feels less full after your baby has detached
- your baby goes from actively sucking to sucking lightly and falling asleep
You may also notice that their body is tense — their hands in tight fists — at the beginning of the feed. But when they’re done, they have unwound and seem more relaxed.
If your baby shows signs of not getting enough milk (fewer wet or dirty diapers and slowed weight gain), then waking them up for those feedings is definitely something you’ll want to focus on.
If you’re not sure if your baby is getting enough milk, visit your pediatrician for a wellness visit and weight check. Again, if your baby is healthy and growing well, falling asleep while nursing isn’t something to stress out too much about. Having your doctor examine your baby can help you sort out what’s going on.
There are some cases in which a “sleepy at the breast” baby may not exhibit typical newborn behavior. In those instances, extra sleepiness is a sign of a medical condition.
The most common newborn condition that tends to make babies extra sleepy is jaundice. In addition to lethargy and poor feeding, babies with jaundice may have yellowish skin, fewer wet or dirty diapers, and may be extra fussy.
Babies with jaundice should see a pediatrician to make sure there are no serious health concerns.
Rarely, babies who are sleepy during feeds may have underlying medical conditions such as a cardiac or respiratory condition. They may also be battling a virus or bacterial infection.
If your baby is having difficulty breathing, has a fever, is vomiting, or is difficult to rouse, speak with your doctor or seek emergency medical attention.
Luckily, there are many things you can try if your baby keeps falling asleep while breastfeeding or chestfeeding. Here are a few favorites.
Tip 1: Switch sides
If your baby falls asleep frequently while nursing, you can try a technique called switch nursing. This is as simple as it sounds.
As soon as your baby starts falling asleep (you may notice that their sucking becomes less frequent or fluttery), you can try switching them to the other side. This may wake them up, and they may find that the other side has milk more readily available.
Tip 2: Compression
Your baby may become sleepy when milk flow slows down. It’s normal for there to be times during a nursing session when the milk flows faster — this is usually during letdown — and times when it slows. But some babies get frustrated when this happens and tend to zonk out.
It’s normal for there to be times during a nursing session when the milk flows faster — this is usually during letdown — and times when it slows. But some babies get frustrated when this happens and tend to zonk out.
You can help get milk flowing again by doing something called breast compression. Using your free hand, cup the side of your breast, making a C shape with your hand. Then gently squeeze. You should feel your baby’s suckling become more active as the milk starts to flow.
Tip 3: Strip your baby down to their diaper
Babies that are too warm tend to get sleepy. So strip your baby down to their diaper and try nursing them. You can also apply cool washcloths to their skin to keep them awake.
If you’re concerned that your baby is too cold, you can drape a breathable blanket over them. But don’t worry too much: When they’re skin to skin with you, they’ll stay warm enough.
Tip 4: Tickle those toes!
Gentle stimulation of your baby’s senses can wake them up. Try tickling their toes, walking your fingers up and down their arms, or swirling your finger around the top of their head.
Try tickling their toes, walking your fingers up and down their arms, or swirling your finger around the top of their head.
Tip 5: Check the latch
If your baby isn’t latching well, they may not be able to get enough milk, and not getting enough milk can make your baby sleepy.
A good latch means that your baby’s mouth is wide open and they’re taking in a good portion of the areola. If you aren’t sure that your baby has a good latch, consider contacting a lactation consultant for assistance.
Tip 6: Get to skin-to-skin
Having skin-to-skin time with your baby is a great way to wake them up to feed. Dress your baby in their diaper only and place them belly to belly with you. This allows them to tap into their newborn instincts, which include searching for and locating the breast.
See if your baby wants to smell, lick, and explore. They may latch onto the breast themselves without any coaxing!
What if nothing is working and your baby just simply can’t stay awake while breastfeeding or chestfeeding? This is definitely an instance where you want to seek out professional lactation help or medical attention, if you haven’t already.
If your baby has gotten to the point where they’re not taking in milk while feeding, supplementing may be necessary.
Supplementing — when done mindfully, and with your own expressed milk when possible — might be just the thing that perks your baby up so that they can have the energy to nurse well. Working on latching, positioning, and other possible issues may also be vital in helping you solve this concern.
Most of all, don’t give up. So many nursing parents have been in this situation at one time or another and have gotten to the other side. You’ll get through this, too.
The baby gets tired quickly when feeding and breathes often: symptoms, diagnosis
With the advent of the baby, all the mother's attention is focused on feeding the baby. After all, I really want the baby to gain weight well. But often during feeding, a woman notices that the baby gets tired quickly. In such a situation, the baby's breathing quickens, which prevents him from eating the prescribed norm. If such a picture is observed with frightening frequency, it is necessary to find out the cause of the problem.
If such a picture is observed with frightening frequency, it is necessary to find out the cause of the problem.
In pediatric cardiology, there are several important signs that indicate heart problems in a young patient. The children's cardiologist of the multidisciplinary center "Edkarik" will be able to figure out what caused the difficulties in feeding. At the first negative symptoms in the baby, parents should contact us to exclude the presence of a serious heart pathology in the crumbs. nine0003
Features of breathing in infants
It should be noted right away that difficulty breathing during feeding is not always an indicator of an existing heart pathology. Such a symptom is typical for respiratory diseases, breathing difficulties may be associated with structural features of the nasal septum. This problem is often observed in the first weeks due to undeveloped breasts in the mother. The child has to make every effort to get the right portion of food. Therefore, he quickly gets tired, and his breathing goes astray from the normal rhythm. nine0003
nine0003
The breathing of children in the first months of life has its own characteristics. Babies need twice the amount of oxygen, but their respiratory system is not yet completely formed. Certain difficulties in the respiratory function are imposed by narrow nasal passages and weakness of the pectoral muscles. Therefore, breathing in children up to a year is uneven. The child often takes quick breaths, so his breathing is shallow and intermittent.
The norm of respiratory movements in babies of the first month of life is 40-60, from the end of the fourth week and up to 3 months - up to 45, in the period of 4-6 months - 35-40. By the year, the baby is already taking about 30-35 breaths per minute, which is considered the norm. nine0003
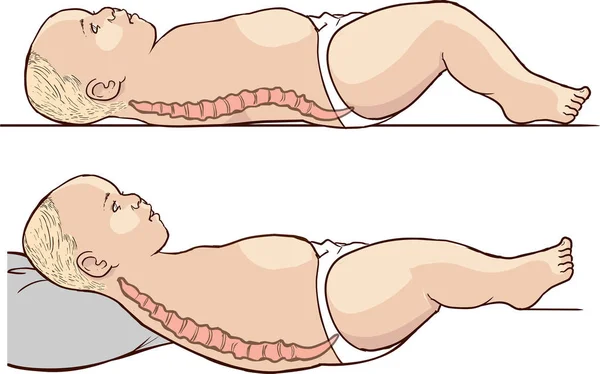
Mom can determine the respiratory rate on her own. To do this, put the baby on his back, and use a stopwatch to count the number of breaths. Since babies "breathe" with their tummies, such a calculation is easy to make. The main condition for performing this procedure is that the child must be calm.
When there is no reason to worry
The nervous system of young children is still imperfect, so they cannot control their breathing. During active games and crying, the frequency of respiratory movements increases, and in a dream they often sniffle. If such features are observed sporadically, you should not worry. The sniffing nose can be washed with boiled water, and then carefully remove the dried mucus. nine0003
What should cause alarm
You need to see a doctor if the baby:
- holds his breath for a long time;
- exhales noisily;
- if breathing is accompanied by wheezing and wheezing.
Typically, such symptoms can be traced against the background of an acute period of respiratory diseases. Timely treatment will help to quickly eliminate these negative signs, after which the child will be able to breastfeed normally again.
Which symptoms require special attention
We have listed physiological breathing problems. But sometimes the situation is much more serious than the usual runny nose. We list the signs that should be a strong argument for parents to urgently visit a pediatric cardiologist.
But sometimes the situation is much more serious than the usual runny nose. We list the signs that should be a strong argument for parents to urgently visit a pediatric cardiologist.
- Cyanosis
If holding the breath during feeding is accompanied by a blue nasolabial triangle, this sign indicates a lack of oxygen. In severe forms of cardiac pathologies, the chin and fingers of the baby turn blue. This symptom is characteristic of congenital malformations of both the heart and vascular anomalies. nine0003
- Shortness of breath
This symptom also indicates a lack of oxygen. Since the child has to expend more energy during sucking, this symptom is more pronounced than at rest. A cause for concern can be considered frequent breaks for rest during suckling. Normally, there are no more than two such pauses, and a child with heart disease takes breaks after 2-3 sips.
- Fatigue
Infants with congenital heart defects are much less active than healthy children. They are not able to suck out the norm during feeding, so they lose weight. The problem is aggravated by frequent breathing. The child simply suffocates under tension. nine0003
They are not able to suck out the norm during feeding, so they lose weight. The problem is aggravated by frequent breathing. The child simply suffocates under tension. nine0003
- Chest pain
Infants may not complain of such a symptom, but an observant mother will notice under what circumstances and how often the child begins to worry.
If all the described signs are repeated from the baby during feeding regularly, it is urgent to consult a pediatric cardiologist. A full-scale examination will determine the cause of the problem, and an experienced pediatric cardiologist will prescribe adequate therapy for the child. nine0003
Peculiarities of diagnosing infants
Babies under one year old cannot describe the symptoms that prevent them from developing normally. Therefore, all hope for an objective examination. During the initial examination of the infant, the pediatric cardiologist:
- evaluates the general condition;
- notes the color of the skin;
- listens to the baby's heart;
- performs heart rate monitoring and saturation level measurement.

The doctor pays special attention to taking an anamnesis, since such information can indicate the cause of the problem. For example, an infection transmitted by a woman during her mother's pregnancy can provoke the development of congenital heart defects. An important factor is heredity, especially if there were cases of premature death (up to 50 years) among close relatives in the family. After collecting the data, the pediatric cardiologist will definitely prescribe the following types of diagnostic procedures:
- ECG with daily monitoring;
- ultrasound of the heart;
- Chest x-ray;
- Laboratory tests.
Instrumental methods of examination with the use of modern devices will clarify the parameters of the baby's heart and the features of its anatomical structure. Ultrasound diagnostics helps to identify defects in the heart chambers and great vessels. Having the data of all studies at hand, the pediatric cardiologist will draw up an individual treatment program, or prescribe additional procedures. In severe cardiac pathologies and rhythm disturbances, the question of a surgical way to eliminate the problem can be decided. nine0003
In severe cardiac pathologies and rhythm disturbances, the question of a surgical way to eliminate the problem can be decided. nine0003
Examination and treatment in the center "Edkarik"
Among our guarantees:
- professionalism of doctors;
- high quality service;
- comfortable conditions in the clinic;
- individual approach;
- a wide range of services;
- accompanying patients during the rehabilitation period.
Our clinic is known not only in Kaliningrad, but also in other regions of the country. Parents and their kids will feel comfortable in our center, because there is everything you need to make sick children feel at home with us. You can make an appointment with a pediatric cardiologist on the official website of our center. There are also contact numbers where parents can consult on issues of concern to them. nine0003
Feeding children with special needs
American Academy of Pediatrics and The American College of Obstetricians and Gynecologists. Breastfeeding Handbook for Physicians 2006). - American Academy of Pediatrics and American College of Obstetrics and Gynecology. "Medical Guide to Breastfeeding", 2006.
Breastfeeding Handbook for Physicians 2006). - American Academy of Pediatrics and American College of Obstetrics and Gynecology. "Medical Guide to Breastfeeding", 2006.
Lawrence , R . A . & Lawrence , R . M . Breastfeeding : a guide for the medical profession ( Elsevier Mosby , Maryland Heights , MO , 2011). - Lawrence R.A., Lawrence R.M., "Breastfeeding: A guide for healthcare professionals." (Publisher Maryland Heights , Missouri, USA: Elsevier Mosby; 2011. )
)
Prime, D.K. et al. Simultaneous breast expression in breastfeeding women is more efficacious than sequential breast expression. Breastfeed Med 7, 442-447 (2012). - Prime D.K. et al., “During the breastfeeding period, pumping both breasts simultaneously is more productive than sequential pumping.” nine0129 Brest Med (Breastfeeding Medicine) 7, 442-447 (2012).
Morton, J., Hall, J.Y., Wong, R.J., Benitz, W.E. & Rhine, W.D. Combining hand techniques with electric pumping increases milk production in mothers of preterm infants. J Perinatol 29, 757–764 (2009). — Morton J., Hall J.I., Wong R.J., Benitz W.I. and Rhine, W.D., "Manual pumping combined with an electric breast pump increases breast milk production in mothers of preterm infants." J Perinatol (Journal of Perinatology) 29, 757-764 (2009)
Hill, P.D., Aldag, J.C., Chatterton RT. Initiation and frequency of pumping and milk production in mothers of non-nursing preterm infants. J Hum Lact . 2001;17(1):9–13 - Hill P.D., Aldag J.S. and Chatterton, R.T., "Onset and frequency of expression and milk production in mothers who have given birth to premature babies and have not breastfed them." J Hum Lakt (Journal of the International Association of Lactation Consultants) 17, 9-13 (2001).
J Hum Lact . 2001;17(1):9–13 - Hill P.D., Aldag J.S. and Chatterton, R.T., "Onset and frequency of expression and milk production in mothers who have given birth to premature babies and have not breastfed them." J Hum Lakt (Journal of the International Association of Lactation Consultants) 17, 9-13 (2001).
Hill, P.D., Aldag, J.C., Chatterton RT, Zinaman M. Comparison of Milk Output Between Mothers of Preterm and Term Infants: The First 6 Weeks After Birth. J Hum Lact . 2005 February 1, 2005; 21(1):22–30. - Hill P.D., Aldag J.S., Chatterton R.T., Zinaman M., "Comparison of the amount of milk in mothers of full-term and premature babies in the first 6 weeks after birth." J Hum Lakt (Journal of the International Association of Lactation Consultants) 2005, 21(1): 22-30.
Parker, L.A., Sullivan, S., Krueger, C.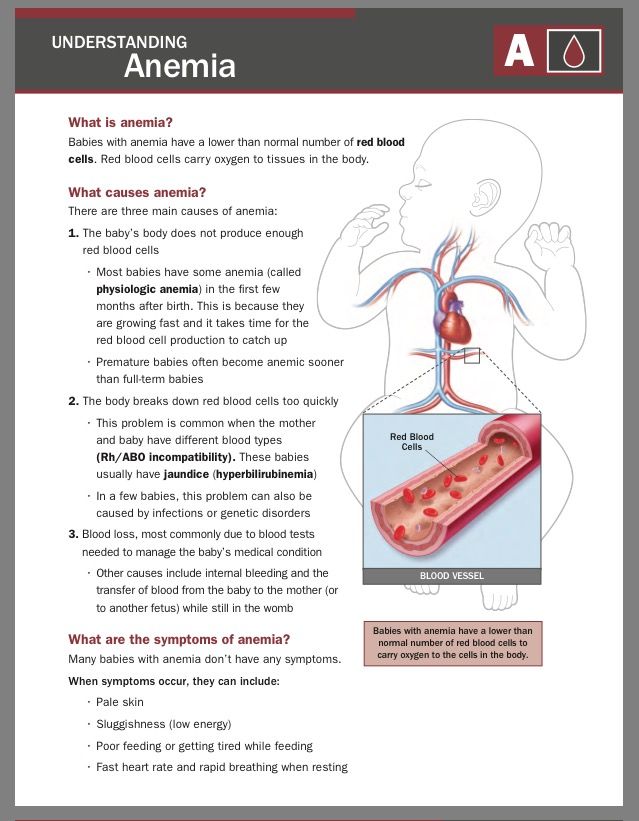 & Mueller, M. Association of timing of initiation of breastmilk expression on milk volume and timing of lactogenesis stage II among mothers of very low-birth-weight infants. Breastfeed Med (2015). - Parker L.A., Sullivan S., Kruger S., Kelechi T. and Muller M., "Association of the time of onset of pumping with the amount of milk and the timing of the second stage of lactogenesis in mothers of children who had extremely low birth weight" . nine0129 Brestfeed Med (Breastfeeding Medicine) (2015)
& Mueller, M. Association of timing of initiation of breastmilk expression on milk volume and timing of lactogenesis stage II among mothers of very low-birth-weight infants. Breastfeed Med (2015). - Parker L.A., Sullivan S., Kruger S., Kelechi T. and Muller M., "Association of the time of onset of pumping with the amount of milk and the timing of the second stage of lactogenesis in mothers of children who had extremely low birth weight" . nine0129 Brestfeed Med (Breastfeeding Medicine) (2015)
Meier, P.P., Engstrom, J.L., Janes, J.E., Jegier, B.J. & Loera, F. Breast pump suction patterns that mimic the human infant during breastfeeding: Greater milk output in less time spent pumping for breast pump-dependent mothers with premature infants. J Perinatol 32, 103-110 (2012). - Meyer P.P., Engstrom J.L., Jaynes J.I., Jaegier B.J., Loera F. "Pumping patterns that mimic breastfeeding behavior: more milk and less time for constant pumping mothers of premature babies".