Baby makes clicking noise when bottle feeding
Why does my baby click when they eat? — Mattos Lactation
Read time | 10 minutes
When I wrote on the causes of clicking during breastfeeding last year, I had no idea that it would quickly move to the first page of google.
I knew hearing clicking noises during feeding was a common occurrence for parents, but I couldn't have imagined that a short, poorly written post would become my highest performing post to date, with over 3,050 views since posting.
While my understanding of clicking during infant feeding hasn't changed much, my ability and desire to create easy to understand, in-depth blog posts has increased.
Therefore, I want to tackle this topic again, but in a manner that is true to me, resulting in an article that I don't shake my head and wonder, "Shondra, what were you thinking to post this unhelpful, pointless trash?"
What is Clicking?
In this context, clicking describes a short, sharp sound created from a baby's mouth. It sounds similar to a "tsk tsk" sound one makes if they're demonstrating disapproval (or "tut-tut" for my UK folks), though some might better relate to the ICONIC tongue popping sound popularized by the queen Alissa Edwards.
When it comes to baby, the clicking sound isn't as sharp or consistent as tongue pops made by adults, but once you're familiar with the general sound, identifying clicking variations during infant feeding becomes easy.
What causes clicking?
Clicking is caused whenever there is a loss of suction. This can happen both at the breast or on the bottle, and may or may not be seen in conjunction with more obvious signs of "breaking the seal" such as leaking.
How the clicking noises sound- sharp and bright or muffled- can depend on which part of the tongue loses suction, which also explains why for some, milk spilling from the baby's mouth accompanies the clicking, and for others, there's just the sound.
Note: There can be leaking without clicking too, which also provides useful information for troubleshooting feeding difficulties.
Is clicking a problem?
Though I would argue that clicking sounds aren't normal, I wouldn't say it's always a problem.
For example, if your baby makes the occasional clicking noise or if it's during a time of intense breast fullness, there's generally nothing to worry about.
Consistent clicking during feeding, however, especially in conjunction with other signs of feeding difficulties, such as nipple pain, slow weight gain, coughing, choking, gasping, panting, unlatching, grimacing, should be evaluated, even if it occurs during bottle-feeding.
Why is my baby making clicking noises?
There are many reasons possible causes for clicking.
Poor positioning/latch
A strong, forceful letdown
Engorgement
Poor tongue mobility/function (Such as tongue tie)
A weakness of the tongue
Inability to maintain a seal due to weak muscles or restricted lip (lip tie)
Body tension or physical limitations such as Torticollis
Hard Palate abnormalities
Submucosal cleft
Ear Infections
Thrush
Let's take a look at each case separately.
Poor latch & positioning
Oft, the phrases latch & position are used synonymously. Still, they describe two distinct steps- the latch refers to how your baby's mouth attaches to the breast or bottle and position relates to your baby's physical arrangement and orientation in space and in regards to the feeding parent.
To make it easy
Latch = mouth. Position = body. Latch =/= position.
A baby's position can, and often does, affect how effectively a baby latches and how well they can transfer milk ( a whole different & distinct step of feeding!)
An issue with the latch OR the position can cause clicking in some babies, in which case, mastering the latching technique and finding the right feeding position to support your baby's feeding ability may be all that's needed to achieve quiet feeding.
The act of mastering latching is many times easier said than done. Even after reading this excellent FREE 24-page latching guide, some parents will need additional latching support and troubleshooting.
Even after reading this excellent FREE 24-page latching guide, some parents will need additional latching support and troubleshooting.
Luckily, even if you live in an area short on IBCLC's, there are often many experienced lactation professionals who can help with latching basics and refer when necessary if tailored latching help doesn't resolve the issue.
A strong, forceful letdown
Just as some are "blessed" (or "cursed" depending on who you ask) with very robust milk supplies, some are "blessed" with an extraordinary rate of milk flow.
Though forceful letdowns & oversupply often go hand and hand, forceful letdowns (Overactive Milk Ejection Reflex [MER]) can happen in those with "typical" milk supplies. However, the underlying cause may be different. For example, full breasts often accompany oversupply, which may result in a forceful letdown due to the pressure build-up inside the mammary glands. The first letdown, and even the second, may be mighty as the breast releases the milk with a force that rivals Niagra Falls.
With Overactive MER, rather than the force stemming from milk volume, the power is due to an overachiever reaction on the part of the pituitary gland( which sends out the hormone that tells the 'milk sacs' to contract and send the milk out the breast).
As you may imagine, regardless of the cause, your baby can easily become overwhelmed with the rate of milk and release tongue suction to allow milk to spill from the sides of their mouth so they can breathe.
If the flow rate is the cause of the clicking, strategies tailored for managing overactive letdowns, along with more upright & laidback feeding positions, should resolve the clicking.
Engorgement
This cause is pretty simple: Full, taut breasts are hard to grasp on to, so during periods of intense engorgement or fullness, clicking may occur.
Resolve the swelling or reduce breast fullness, and the clicking should stop.
Poor tongue mobility/function (Such as tongue tie)
Poor tongue function is NOT always caused by tongue-tie, however, tongue-tie often causes poor tongue function thus impacting its range of motion (mobility).
There are many stages of the feeding and swallowing process, and a limited function of the tongue can impact each of the required steps.
The clicking sound associated with poor oral function due to tongue-tie can be broken down to this straightforward overview-
A tight frenulum doesn't allow your baby's tongue to raise to the proper placement for easy feeding OR the effort it takes your baby to overcome the resistance of a tight frenulum is such that they quickly get tired and start to lose suction.
Reduced tongue mobility is the most common cause of persistent clicking I see. There is such a strong association with clicking and tongue ties, that clicking alone is enough to prompt a tie suspicion even in the absence of "typical tongue-tie appearance."
A weakness of the tongue
The tongue is a group of muscles, and with any muscles, it can be or become weak. Weakness may be a byproduct, which is commonly seen with tongue-tie and explains the need for tongue strengthening exercises pre and post revision, but can be a stand-alone cause of clicking.
It takes an experienced and highly trained professional (such as IBCLCs who specialize in supporting tied babies) to be able to differentiate between limited tongue function caused by weakness vs. reduced tongue mobility caused by ties.
Inability to maintain a seal due to weak muscles or restricted lip (lip tie)
There is a profound link between tongue mobility and many other structures of the body (see below), to include the lips and surrounding oral muscles. Any weakness or limitation of any oral anatomy has the potential to impact tongue function.
Body tension or physical limitations such as Torticollis
See above. Insert body tension/physical limitation in place of muscle weakness/lip tie.
Hard palate abnormalities
The hard palate is the bony part of the roof of the mouth. We expect the palate to be intact with a gradual slope.
Sometimes there are abnormalities in the palate, be it due to congenital defects (such as cleft palates) or due to abnormal development caused by a lack of appropriate palate pressure in utero (ex: bubble palates).
During breastfeeding and bottle-feeding, the palate provides a platform for stabilizing the breast/teat in the oral cavity. Palatal abnormalities can impact stability, and clicking can result.
Submucosal clefts/ Velopharyngeal insufficiency (VPI)
Generally speaking, clicking sounds often come from the anterior portion of the mouth, and some may argue that clicking doesn't occur with submucosal clefts or VPI.
I wanted to add this category because how parents and providers interpret clicking is subjective. And because clicking noises already vary in sound and intensity, I don't think it's too much of a stretch to include sounds that may be loosely considered clicking.
Milk leaking from the nose during feeding is a classic symptom of submucosal clefts/VPI and will always require a referral for further evaluation. However, sometimes a soft puffy "clicking-esque" noise may be present due to loss of suction of the soft tissues near the throat and would also warrant a referral.
Ear Infections/ Thrush
Thrush & ear infections both can change the way your baby eats, and temporary clicking may occur. Once the thrush or ear infection resolves or the pain disappears, the clicking noises should stop as well.
I'll admit, I'm biased, but ff your baby suddenly starts to click and around the same time, you notice you're having some breast pain, it would be good practice to schedule a lactation consultation. During the consult, we will assess what's causing the pain and develop a care plan to reduce the discomfort.
As you may see, there are a lot of possibilities for your baby’s clicking. In many cases, when clicking persists despite position changes and after engorgement passes, the clicking is due to something structural.
I often find myself asking if there’s any clicking present during feeding when parents complain of pain, slow weight gain/weight loss (baby), and low supply.
The reason?
Babies need a proper seal to maintain vacuum pressure to transfer milk effectively and efficiently.
Many times parents are told that clicking is typical, or that there are no issues with their baby’s noisy eating, even though they sound similar to the baby below.
The baby in this clip is NOT feeding efficiently at all. Continued poor feeding is often very stressful for babies (and parents) and can lead to long term feeding aversions. Clicking may be the only noticeable sign of dysfunctional feeding, especially when babies are gaining weight or having appropriate diaper output.
If your baby is making clicking noises that persists or if they leak, gulp, gasp, pant, pop off or grimace and fuss while feeding (bottle or breast), please download this DIY Oral Assessment worksheet.
Once completed, you will have a better understanding of your baby’s oral strengths and weaknesses. The sooner we find solutions to make feeding easier for your baby, the better. You can book an appointment here.
The sooner we find solutions to make feeding easier for your baby, the better. You can book an appointment here.
You may also like:
Shondra MattosComment
0 LikesWhy Does My Baby Click When Bottle Feeding (Is it a Problem?)
Feeding your baby should be a straightforward process that causes no concerns. But what happens when you hear clicking sounds or noises during the bottle feeding? Is it a sign something is wrong?
Clicking sounds while bottle-feeding are caused by a loss of suction. The clicks may be attributed to milk flow, hunger level, or a tongue-tie. Most clicks can be remedied by tracking your baby’s feeding times and ensuring both the position and nipple are best for your little one. If that doesn’t help, have your child evaluated for a tongue-tie.
Read on to get a better understanding of why there is clicking during bottle feedings. Knowing the cause could help you determine what to do to stop it.
Knowing the cause could help you determine what to do to stop it.
Table of Contents
Why do babies make a clicking noise while bottle feeding?
Many parents researching clicking noises will come across a lot of resources regarding clicking that is associated with breastfeeding, but why would your bottle-fed baby be making clicking sounds while feeding?
While it can be hard to imagine what a clicking baby sounds like, if you’ve heard it, you know what I’m talking about. It doesn’t sound like when an adult clicks or pops their tongue, but you might recognize it as a much lighter, more muted version of the sound. The sound may or may not be accompanied by your baby leaking milk or formula out of their mouth.
The overall reason your baby will make clicking sounds while bottle feeding is that they are losing suction. This may be because:
- Milk flow is too strong – This may be caused either by a too-large nipple opening or a feeding position that is increasing milk flow and not allowing your baby to swallow before their mouth is filled again.

- Your baby is not actually hungry – If your baby is holding the bottle and chewing on the nipple instead of actually eating, they may be comfort feeding rather than actually in need of sustenance.
- A tongue-tie may be obstructing your baby’s suction – This is a band of tissue in your baby’s mouth that is overdeveloped and impeding your baby’s tongue motion. It may require medical intervention, but it’s a minor procedure that many babies have.
For reasons your baby is dribbling milk while feeding, check out this resource.
Does a clicking sound mean my baby is tongue-tied?
If it’s your first time hearing the term tongue-tie, you are probably wondering what that is. The medical term for tongue-tie is ankyloglossia.
Babies with a tongue-tie have a problem latching or maintaining a latch while feeding because of an abnormality in the lingual frenulum. In this case, the lingual frenulum (the bit of tissue connecting the tongue to the bottom of the mouth) is either shorter or tighter than is typical and limits the tongue’s movement.
Tongue-tie is more likely to affect boys than girls, and will likely require a professional such as a lactation consultant or ENT to diagnose.
While a clicking sound does not necessarily mean your baby has a tongue-tie, you should consider having your little one checked if the sound persists despite attempts to resolve any feeding issues (tips below!).
How to stop baby from clicking when bottle-feeding
Before you can begin to consider ways to stop your baby from clicking, you have to know and understand the reasons behind the sound.
Is your baby comfort feeding? Is the milk/formula coming out too fast for them? How are they positioned while being fed? What stage are they at developmentally? Are they teething?
The best ways to stop your baby from clicking while bottle-feeding are:
- Proper feeding position
- Change bottle nipple size
- Track feeding time
- Evaluate for tongue-tie
- Wait it out
Proper feeding position
It is possible that your baby is losing suction because their feeding position is restricting your baby’s ability to swallow the milk or formula as it flows out of the bottle.
The ideal position for bottle-feeding is to hold your baby at a 45-degree angle with the bottle tilted so that the milk or formula completely fills the nipple (this will help reduce the amount of air swallowed). This position will help avoid choking and gagging on the milk or formula, which is what leads to the clicking.
When feeding your baby, it’s important to find a comfortable position for both you and your baby.
Change bottle nipple size
If the milk or formula is flowing too fast for the baby, you will notice your baby breaking the suction and the milk escaping out the side of their mouth.
In this case, changing the nipple size of the bottle will be beneficial. You want to go down in size so that your baby will have better control of their swallowing.
Track feeding time
Understandably, one of the first things that parents turn to when their baby is crying or fussy is a bottle. However, what if the baby is not due for a bottle and therefore is not hungry?
If your baby is sucking on the bottle instead of trying to feed, they are called comfort feeding. Basically, your baby is using the bottle as a pacifier. If you suspect your baby is comfort feeding, try tracking their feeding to keep better tabs on when your baby may be due for another feeding.
Basically, your baby is using the bottle as a pacifier. If you suspect your baby is comfort feeding, try tracking their feeding to keep better tabs on when your baby may be due for another feeding.
You may also notice there is frequent loss of suction and milk dribble in this case.
Evaluate for tongue-tie
As mentioned earlier, tongue-tie could be a cause for clicking and it may not be easily detected by a non-professional.
Your pediatrician or pediatric specialist can examine your baby. If he has tongue-tie, a procedure called frenotomy can be performed in-office to stop the clicking. By getting your baby’s tongue-tie issue resolved or fixed you can help improve your baby’s suction and therefore stop the click.
The procedure itself is rather straightforward. The doctor will use a sterile instrument, probably a pair of scissors, to cut or divide the frenulum (the tissue that is connecting the tongue to the floor of the mouth) to give your baby’s tongue more range of motion.
If you’re concerned about subjecting your little baby to a medical procedure, watch this video. Your baby may cry, but that is likely to be more because a stranger is holding him down and messing with his mouth, rather than actual pain.
Once done your baby should have better control of their tongue and better suction.
Wait it out
As parents, one of the most difficult things to do is nothing. Not being proactive for your baby when you notice a change could be a real test of patience and resilience.
When it comes to clicking, if your baby is experiencing a developmental change (such as teething) or is sick, the click could be temporary and you just have to wait it out.
Your baby may be teething, which means their mouth is constantly sore. During this stage, they may be breaking the suction on the bottle to get relief from a sore mouth or just because they are not yet accustomed to this new sensation. Once your baby gets used to the growing teeth and the soreness is no longer a factor, they will return to their normal suction.
During this stage, they may be breaking the suction on the bottle to get relief from a sore mouth or just because they are not yet accustomed to this new sensation. Once your baby gets used to the growing teeth and the soreness is no longer a factor, they will return to their normal suction.
In terms of sickness, if the baby is ill and in pain, it could throw off or change the way they suck and swallow, especially if their nose is clogged. As with the teething scenario, once they are better, they should return to their normal suction.
How to breastfeed - Tips for feeding with and without a bottle from Philips-Ukraine
search support iconSearch Keywords
Shopping Cart
There are currently no items in your shopping cart.
- {{#each curatedBundle.items}}
- {{#if miniCartProductpath}} {{/if}} {{#if miniCartProductpath}} {{/if}}
{{#if miniCartProductpath}} {{/if }}
{{#iff curatedBundleQuantity 'gt' '1'}} {{curatedBundleQuantity}} x {{/iff}} {{#if familyName}} {{familyName}} {{/if}} {{#if descriptor}} {{descriptor}} {{/if}}
{{#if miniCartProductpath}} {{/if}}
{{/each}} {{#if isPersonalizedBundle}}
{{#if curatedBundle. price}}
price}}
{{curatedBundle.price }}
{{curatedBundle.discountPrice}}
{{/if}}
{{/if}} {{#if isSubscriptionBundle}}
{{#if curatedBundle.displayPrice}}
{{curatedBundle.displayPrice}}
+{{curatedBundle.displayRecurringCharge.totalFormattedValue}} / {{curatedBundle.ratePlanDuration}}
{{/if}}
{{/if}} {{/if}} {{#if isBundle}} {{#each bundle}}
{{#if bundle.label}}{{bundle.label}}{{else}}Bundled Item{{/if}}
{{#if totalPrice}} {{#if formerPrice}}
{{formerPrice}}
{{/if}}
{{totalPrice}}
{{/if}}
{{/each}} {{/if}} {{#if isSingleItem}}
-{{discountValue}}
{{/if}}{{#if miniCartProductpath}}
{{/if}}{{#iff quantity 'gt' '1'}} {{quantity}} x { {/ff}} {{#if familyName}} {{familyName}} {{/if}} {{#if descriptor}} {{descriptor}} {{/if}}
{{#if miniCartProductpath}}{{/if}} {{#if sellerName}} {{soldBySiteText}} {{sellerName}} {{/if}}
{{#if totalPrice. formattedValue}} {{#if formerPrice.formattedValue}}
formattedValue}} {{#if formerPrice.formattedValue}}
{{formerPrice.formattedValue}}
{{/if}}
{{totalPrice.formattedValue}}
{{/if}}
An error occurred while deleting an item from the cart. Try again
{{/if}} {{/each}}
{{#iff cart.attributes.pricing.orderDiscountNoDelivery.value 'gt' 0}}
Discount: - {{cart.attributes.pricing.orderDiscountNoDelivery.formattedValue}}
{{/ iff}}
Shipping cost: {{#iff cart.attributes.pricing.totalDelivery.value 'gt' 0}} {{cart.attributes.pricing.totalDelivery.formattedValue}} {{else}} FREE {{/iff }}
Subtotal: {{cart.attributes.pricing.total.formattedValue}}
Like all the best things in life, breastfeeding can be both exciting and daunting. Preparing for breastfeeding brings many delightful moments, but for many mothers-to-be, they are overshadowed by thoughts about the problems that breastfeeding can bring. Understand that concerns are part of the process, but clear answers to questions about breastfeeding will help you calm down and gain confidence and peace of mind.
Understand that concerns are part of the process, but clear answers to questions about breastfeeding will help you calm down and gain confidence and peace of mind.
Is your baby not latch on? Are your nipples cracked? Are you experiencing pain while breastfeeding? Know you are not alone. On this page you will find tips and tricks to help you solve these problems. We are always there and ready to help, but our advice does not replace the advice of your doctor. If you are concerned about problems with breastfeeding, be sure to consult with a specialist.
1. "My baby can't latch"
Baby needs time to learn how to latch on properly. Don't be too hard on yourself, you'll be fine. A baby's inability to latch on properly is one of the most common breastfeeding problems and one of the reasons why breastfeeding sometimes hurts.
If your baby does not latch on, you may have problems. When, despite efforts, you are unable to achieve proper fixation of the nipple, you need to seek help. How to understand that the baby takes the breast incorrectly?
How to understand that the baby takes the breast incorrectly?
- You feel pain in your nipples while feeding.
- Baby only latch on to the nipple.
- The baby draws in his lips.
- Baby makes clicking noises or smacks loudly.
- The child is nervous after trying to feed.
- Your milk supply decreases over time even though you feed regularly.
- The baby is losing weight.
Here are some breastfeeding tips to help your newborn learn to latch on properly:
- Create a calm atmosphere. The secret to successful feeding is to always stay calm and relaxed. Lie down on a bed with pillows under your back, or sit in a comfortable chair.
- Make skin-to-skin contact with baby . Place your baby on your bare chest so that his skin touches yours. Body contact will help both of you relax.
- Don't force your baby to breastfeed. Let him take the initiative during feeding.
 You will want to guide and support the child in his efforts, but in no case force this process.
You will want to guide and support the child in his efforts, but in no case force this process. - Find a comfortable position. Sometimes it's all about position. Some positions work, others don't. Try to vary them during feeding and find one in which it will be easier for your baby to latch onto the breast.
- Use correct technique. Place your nipple on your baby's nose and lightly tickle it to activate his instinct. Then the baby will open his mouth wide and will be able to capture most of the areola.
2.
"My nipples hurt"
You may experience sore nipples in the first few days after giving birth. But that doesn't mean you have to endure the pain. Breastfeeding pain can have several causes, from skin sensitivity to uncomfortable nursing positions. The following tips will help you solve the problem in the first few days:
- Express milk. It is very important that the baby emptys the breast completely during feeding.
 If you feel that after feeding you have milk left, it is better to express it.
If you feel that after feeding you have milk left, it is better to express it. - Get into the correct starting position. Make sure your baby latch on properly during feeding. With proper feeding, the nipple and the lower part of the areola are in the baby's mouth.
- Try hot and cold compresses. Use a gel pad to cool your breasts or apply a warm compress. Compresses combined with massage will help relieve inflammation of the nipples.
If the pain persists, seek the advice of a lactation specialist who can help you choose the right treatment. Don't let the problem run its course. If timely action is not taken, milk production may decrease or mastitis may develop.
3. "My nipples are cracked"
Another problem well known to breastfeeders is cracked nipples. It often occurs as a result of a shallow latch on the breast, when the baby does not latch on enough breast tissue and instead sucks only on the nipple. As a result, the nipples become inflamed and cracks appear on them. Measures should be taken in a timely manner to relieve pain and eliminate the risk of infection.
As a result, the nipples become inflamed and cracks appear on them. Measures should be taken in a timely manner to relieve pain and eliminate the risk of infection.
Our recommendations will help relieve sore nipples and make breastfeeding comfortable for you and your baby:
- Wet nipples with expressed breast milk. Don't be surprised! Breast milk can be successfully used to heal cracked nipples. Apply a few drops of breast milk to sore nipples and let it dry naturally.
- Stimulate milk flow before feeding. Apply a warm compress to the inflamed area and express before feeding. This will stimulate the flow of milk.
- Protect sore nipples with special nipples. During the treatment of sore nipples, wear special pads. They can help relieve chest pain while breastfeeding. In addition, nipple shields will relieve any discomfort you may experience while breastfeeding. After each feeding session, apply a special cream to the nipples, it will moisturize the nipples and help relieve inflammation.

- Protect your nipples between feedings. Use a protective pad to protect sore nipples from chafing on clothing between feedings. Place pads in your bra cups to help prevent nipple irritation. In addition, the pads will collect excess milk. Bra pads can be used to prevent breast milk stains on clothes.
- Choose the best feeding position . Usually, in order to keep the baby at chest level, it is enough to put a pillow. You can choose any other position, as long as it does not cause pain and cracking of the nipples.
- Feel free to ask for help . If the cracks don't heal or you have other problems, don't hesitate to ask for help. Talk to your doctor.
4. “My baby is coughing while breastfeeding”
New mothers usually experience a large flow of breast milk during lactation. If the flow is too strong at the time of feeding, the baby begins to choke, cough or spit up milk.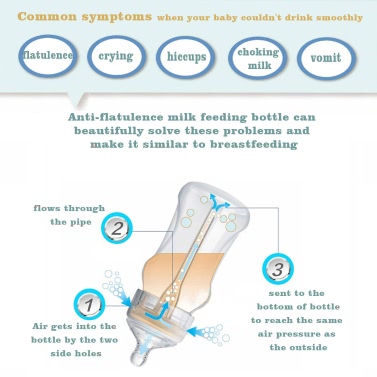 Usually this problem goes away on its own when milk production stabilizes, but it's good to know a little trick to help control the situation:
Usually this problem goes away on its own when milk production stabilizes, but it's good to know a little trick to help control the situation:
- Scissorhands technique. Control the flow during feeding by gently pinching the nipple between your index and middle fingers and applying pressure to the areola.
- Reclining position or pumping before feeding. To reduce milk flow, try feeding your baby in a semi-recumbent position. Expressing a small amount of milk before feeding will also help reduce flow
5. "I have flat or inverted nipples"
Every woman's body is beautiful in its own way, and no two pairs of breasts are the same. Women's nipples come in many shapes and sizes. For some they are flat, for others they are retracted, for others they are large.
It is important for successful feeding that the baby latch on well. Extra effort is required to help the baby latch on to an inverted or flat nipple. If you are the owner of such nipples, know that in fact you are not alone: up to 10% of women have a similar feature 1 . Here are some helpful tips for breastfeeding moms with flat or inverted nipples.
Extra effort is required to help the baby latch on to an inverted or flat nipple. If you are the owner of such nipples, know that in fact you are not alone: up to 10% of women have a similar feature 1 . Here are some helpful tips for breastfeeding moms with flat or inverted nipples.
- Help yourself with your fingers . Try to grab the nipple with your fingers and pull it back.
- Consult a doctor. If you are concerned about the condition of the nipples, do not hesitate to contact a specialist.
Take good care of your breasts
If you feel pain or discomfort when breastfeeding, know that it happens, but this is not a reason to endure gritting your teeth. Whether it's your first breastfeeding or your fourth, the mother-baby duet sounds different each time, and each new feeding experience is unlike the last. If you learn how to properly care for your breasts, the process of feeding will bring you real pleasure.
Getting to know your baby every day is part of the amazing journey of motherhood. Breastfeeding will allow you and your baby to experience many precious moments together, enjoying intimacy and well-being.
1. https://www.sciencedirect.com/science/article/abs/pii/S09609776976
You may need
Philips Avent
900CF05 Manual Breast Pump with Bottle0003
-
-{discount-value}
Join Philips Avent and
get 25% off your next purchase Any links to third party websites that may be included on this site are provided solely as a convenience to you. Philips makes no warranties regarding any third party websites or the information they contain.
Philips makes no warranties regarding any third party websites or the information they contain. I understand
You are about to visit a Philips global content page
Continue
You are about to visit the Philips USA website.
I understand
90,000 too strong tide of milk- On the center
- doctors
- price
- Obstetrics and gynecology
- Pediatrics
- Special children
- Psychology
- 9000 Children
- Motherhood
- Psychology
- Development
- TUTTA TV
- Special children
Home > ARTICLES > Maternity > TOO STRONG MILK FLUSH REFLEX
A baby who eats too much milk too quickly may be restless, irritated at the breast, and you might think that he has "colic". Usually such a child gains weight very quickly. Also a typical picture: the child begins to suck and, after a few seconds or minutes, begins to cough, choke and “fight” with the breast. It can come off the breast - and you see that mom's milk is gushing out. After that, the child sucks again, but again begins to worry - and the performance is repeated. He may be dissatisfied with the "fountain", but impatient if the jet flows slowly. This can be a testing time for everyone. In rare cases, a baby may stop breastfeeding altogether, usually around three months of age. What's happening? The baby eats at once a lot of front low-fat milk. It quickly leaves the stomach, and a large portion of milk sugar, lactose, enters the intestines at once. The enzyme (protein) that helps digest lactose may not be able to handle so much at once, and your baby will have symptoms lactase deficiency crying, gas, violent eructations, frequent watery green stools.
Usually such a child gains weight very quickly. Also a typical picture: the child begins to suck and, after a few seconds or minutes, begins to cough, choke and “fight” with the breast. It can come off the breast - and you see that mom's milk is gushing out. After that, the child sucks again, but again begins to worry - and the performance is repeated. He may be dissatisfied with the "fountain", but impatient if the jet flows slowly. This can be a testing time for everyone. In rare cases, a baby may stop breastfeeding altogether, usually around three months of age. What's happening? The baby eats at once a lot of front low-fat milk. It quickly leaves the stomach, and a large portion of milk sugar, lactose, enters the intestines at once. The enzyme (protein) that helps digest lactose may not be able to handle so much at once, and your baby will have symptoms lactase deficiency crying, gas, violent eructations, frequent watery green stools.
Symptoms of increased milk flow during feeding:
- The child chokes, swallows quickly and noisily, gasps for air, coughs while sucking, as if milk were rushing into his mouth.

- Pulls down the breast during feeding
- Squeezes the nipple during the rush to slow down the flow of milk
- Makes a clicking sound when sucking
- She spit up a lot, a lot of gases are formed.
- Much pissing, copious, sometimes green frothy stools, sometimes streaked with blood
- Periodically refuses to breastfeed.
- Doesn't breastfeed for comfort.
What to do about it?
There are two ways to remedy the situation: 1) help the baby cope with a strong stream and 2) take steps to adapt the amount of own milk to the needs of the child. Since a large milk release is a consequence of its excess production, most mothers will have to work on both programs. It can take a couple of weeks to deal with excess milk, so try to be patient and don't give up.
Child Help:
- Body position. Position the baby so that he sucks milk as if "uphill", so that the force of gravity prevents the pressure of the jet.
 The most effective positions are when the baby's head and neck are ABOVE the level of the nipple. Here is some of them.
The most effective positions are when the baby's head and neck are ABOVE the level of the nipple. Here is some of them.
- The usual position (see photo # 1), but mom leans back on the pillows.
- The child is like a soccer ball, but the mother leans back (photo # 2).
- The child is like a soccer ball, but raised and as if sitting against the mother's nipple (photo 3)
- Sometimes it helps very well to lie down during feeding. If lying on your side does not help, lie on your back or almost on your back, placing the child on top of you. However, do not use this position often - it can lead to blockage of the ducts.
- Try to give one breast at a time if you are not already doing so. In some cases, you need to feed two or three feedings from one breast, straining the filled adjacent breast to a comfortable state.
- Feed your baby more often - between feedings, less milk will accumulate and it will be easier for the baby to cope with it.

- Feed your baby before he gets hungry like a wolf. Do not delay feeding by giving water (baby does not need water even in very hot weather ) or a pacifier. A brutally hungry baby can lunge at the breast and cause a very active milk flow reflex. Feed your baby as soon as you see signs of hunger.
- Feed your baby when he is half asleep and relaxed - he sucks more gently and the stream is less.
- Feed your baby in a calm, relaxed environment whenever possible. Loud music, bright lights do not contribute to proper feeding.
- When you feel a rush during sucking, take the baby off the breast and let the stream of milk come out onto the diaper. When it weakens, attach the child again.
- If you have time, express some milk before feeding. But don't grab this remedy in the first place (because it stimulates milk production).
- The child may not like the fountain, but also be worried and angry when the jet flows slowly.
 If you suspect the latter, poke your breasts while feeding.
If you suspect the latter, poke your breasts while feeding. - The problem is exacerbated if the baby is not properly attached to the breast. Proper attachment is the key to feeding easily.
- Sometimes it helps to prescribe a lactase preparation to a child, 2-4 drops before each feeding. It is available over the counter but is expensive and only works occasionally.
- You can try a nipple shield if nothing else has worked. This is the second means of despair.
- Finally, you can give your baby expressed milk from a bottle rather than switching to formula.
- Let the child spit up more often if he swallows a lot of air.
- If your baby is gaining weight well, try to feed him from one breast at a time.
- If the baby has finished sucking the first breast and wants to suck more - just attach it again to the same breast.
- If there is discomfort in the second breast, pump it a little, just to get a little relief, and then apply a cold compress.
 Your goal is to pump less and less each time, so that you finally stop needing it.
Your goal is to pump less and less each time, so that you finally stop needing it.
- Avoid stimulating your breasts in any way, such as pumping unnecessarily, showering your breasts for long periods of time, or wearing breast pads to collect milk.
- Between feedings, apply cold compresses to the chest (for 30 minutes, removing for at least an hour). This will reduce blood flow and milk production.
- If feeding from one breast at a time does not help for a week, try putting your baby on one breast for a period of time before switching sides. It's called blocking feeding .
- Start with 2-3 hours and add half an hour if necessary.
- Do not shorten the feeding time in general, but whenever the baby wants to eat again - just give him the same breast during this period of time.
- If there is discomfort in the second breast, express it silently to a comfortable state, and then apply a cold compress.
 Your goal is to pump less and less each time, so that you finally stop needing it.
Your goal is to pump less and less each time, so that you finally stop needing it. - In more stubborn cases, the mother may have to try feeding from one breast for more than 4 hours to determine the amount of time that works best.
- Additional measures for excess milk, which should be used only in the most stubborn cases, are compresses from cabbage leaves and grass.
Even if all these measures do not completely solve the problem, for many mothers, excess milk production and flow to the nipple normalize to some extent around 12 weeks. The hormonal changes taking place at this time make lactation more stable and more appropriate to the needs of the baby.
Sometimes children of mothers with profuse and rapid milk flow get used to this state of affairs very well and become unhappy when the flow decreases in a normal way between 3 weeks and 3 months. Even if the jet is not actually weak, it may seem so to a child. See Let-down Reflex: Too Slow? for tips.