Baby will not feed
Why is my baby refusing the breast? 8 tips that help | Baby & toddler, Feeding articles & support
Whether your baby refuses the breast as a newborn or when they’re older, it can be very stressful. Here’s why it might happen and what to try…
Why won’t my newborn baby breastfeed?
Sometimes, newborn babies struggle to latch on to breastfeed after they’re born. It can be worrying for new parents when this happens – you might think something’s wrong.
There may be a simple explanation. This information could help you find your own solution, or decide if you need further support.
Some of the more common reasons for newborn babies finding it difficult to latch onto the breast could be:
- a difficult labour or birth – your baby might feel sore or have a headache if the mother has had interventions in labour or if they were born very quickly
- medication used during labour – anaesthesia, epidural or pethidine can make your baby sleepy or groggy
- your baby being separated from you after birth – even for a few minutes
- discomfort due to a birth injury or bruising
- swallowing mucus at birth can make your baby feel congested, nauseous or uncomfortable
- an early unpleasant experience of attempting to breastfeed, such as being forced onto the breast
- the baby might have tongue-tie
(LLLGB, 2016)
Why won’t my baby breastfeed anymore?
Sometimes, older babies seem to refuse to breastfeed when they’d been breastfeeding just fine until then. This is known as a 'nursing strike.' They might refuse to breastfeed for 2-4 days, but it can be up to 10 days (Mohrbacher, 2013).
Reasons that your older baby might refuse to feed at the breast could include:
- something has changed that makes it difficult for baby to latch
- a strong or fast flow of milk, which your baby is struggling to take
- a painful mouth, due to an infection like thrush or because they’re teething
- being more aware of their surroundings and being easily distracted, for example by noise
- a change in the taste of your milk, such as that due to your menstrual cycle
- the introduction of more solid food
- a small number of babies might struggle because of severe or persistent reflux, known as gastro-oesophageal reflux disease (GORD), so they may link feeding with pain.
(Mohrbacher, 2013; Gonzalez, 2014; BellyBelly, 2016; NICE, 2017; Public Health England, ND)
What can I do when my baby refuses to breastfeed?
8 top tips to help your baby who’s refusing to breastfeed:
1. Try to identify what’s going on for your baby. Knowing the cause can help not only with a plan but it can be reassuring to understand what is happening and know there’s a solution. You could think about the following:
Try to identify what’s going on for your baby. Knowing the cause can help not only with a plan but it can be reassuring to understand what is happening and know there’s a solution. You could think about the following:
- Do they have a cold or an infection?
- Was there something that might have caused them to not want to feed?
- Talk to one of our Breastfeeding Counsellors or contact our Infant Feeding Line on 0300 330 0700 (option 1) for further support. It can be a great way to get some help to find out what’s happening.
- You could also contact a health professional to investigate any medical reasons why your baby might not be feeding.
2. Try to stay calm and not force a feed. Instead, allow your baby to take the lead.
3. Especially for young babies, many mums find skin-to-skin contact in a laid-back position helps to take the pressure out of the situation. It allows your baby to use their own natural instincts to feed (Burbridge, 2017).
4. Don’t worry if your baby bobs their head or moves it from side to side, they’re not rejecting the breast as it might appear. These are your baby’s natural ways of finding your breast (Coulson, 2012).
5. Try a different feeding position to see if you can get your baby more comfortable. Some babies find a laid-back breastfeeding (also called biological nurturing) position helpful if they are struggling to get a deep latch or if you have a strong let-down of milk (Coulson, 2012).
6. Sometimes, feeding your baby while they’re sleepy or even asleep can be helpful. Many mums say that these ‘dream feeds’ can be very effective for a baby who is uninterested when awake (Pitman and Bennett, 2008).
7. You could try feeding your baby while rocking them or walking around, singing or playing with them or playing white noise or background music to them (Australian Breastfeeding Association, 2017).
8. You might want to try feeding in a quiet room, away from distractions, as some babies are so keen to be involved that they limit their feeds (Gonzalez, 2014).
You might want to try feeding in a quiet room, away from distractions, as some babies are so keen to be involved that they limit their feeds (Gonzalez, 2014).
What can I do if I’ve tried everything but my baby still won’t breastfeed?
One of the key things to consider is maintaining your milk supply. You might need to consider expressing, either by hand or with a pump. You can find more information about expressing and storing your milk here.
Another consideration is making sure your baby is getting enough milk. How might you know how much milk your baby is getting, you might ask. The answer lies in their dirty and wet nappies. You can expect six wet nappies in 24 hours if your baby is over a week old (UNICEF, 2016). If you’re unsure, it’s best to ask for support from your health visitor, GP or NCT breastfeeding counsellor.
In the short term, you might need to look at alternative ways to feed your baby if you think they’re not getting enough milk. A newborn baby needs to be fed regularly and parents can use syringe or cup feeding as an alternative to a bottle in the early days (Flint et al, 2016; NHS, 2016).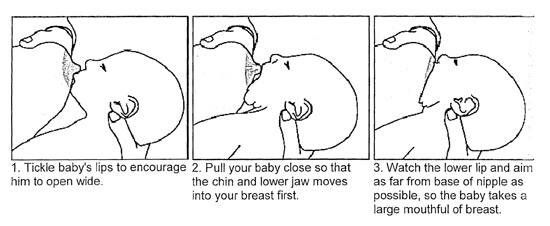
If you decide to use a bottle, it might be helpful to feed with plenty of skin-to-skin contact (UNICEF, 2018). Gently offering the bottle to your baby by tickling their top lip, waiting for the wide-open gape might also help mimic a breastfeed (UNICEF, 2019). That can support the transition back to the breast.
Taking frequent breaks during the bottle feed, and perhaps swapping sides, can be helpful (UNICEF 2018). Continuing to have skin-to-skin time with your baby and allowing them access to the breast will help this. It’ll also be a bonding and calming experience for you both.
How can I deal with the stress of my baby refusing to breastfeed?
When a newborn refuses the breast, or an older baby goes through a nursing strike, it can be very upsetting for both you and your baby. You’re definitely not alone in struggling with the emotions of breastfeeding problems. So here are some tips that might help:
- Try to take time to enjoy plenty of extra cuddles and quiet time together.

- Many mums find a ‘babymoon’ helpful for allowing their baby access to the breast in a non-pressurised way. A babymoon means spending some hours together in a relaxed setting, such as lying down snuggling in bed. This can allow you to enjoy your baby without worrying about feeding.
- For older babies, some mums find that having a bath with their baby or bringing their baby into bed with them helps their baby to latch.
- Try to find some support from other mums and trained breastfeeding supporters. Chatting with other people about this can help to unburden the stresses and worries you might be feeling. Breast refusal is not uncommon and you might find that chatting to someone who understands is invaluable while you’re struggling.
- For many mums, time and patience can help the situation. Your baby’s instincts and behaviour can change and develop, especially in the early days.
- If you’re struggling, do contact the NCT Infant Feeding Line and speak to a breastfeeding counsellor.
 They’ll listen, offer you information and will support you to find your own path.
They’ll listen, offer you information and will support you to find your own path.
This page was last reviewed in August 2019.
Further information
NCT supports all parents, however they feed their baby. If you have questions, concerns or need support, you can speak to a breastfeeding counsellor by calling our helpline on 0300 330 0700, whether you are exclusively breastfeeding or using formula milk. Breastfeeding counsellors have had extensive training, will listen without judging or criticising and will offer relevant information and suggestions. You can also find more useful articles here.
National Breastfeeding Line (government funded): 0300 100 021.
NHS information on mastitis.
Best Beginnings - Bump to Breastfeeding DVD Chapter 7 'Overcoming Challenges'.
Healthtalkonline.org: Managing Breastfeeding – dealing with difficult times.
References
Australian for Breastfeeding Association (2017) Breast refusal. https://www.breastfeeding.asn.au/bf-info/breast-refusal [Accessed 22nd February 2019]
https://www.breastfeeding.asn.au/bf-info/breast-refusal [Accessed 22nd February 2019]
BellyBelly. (2016) Breast refusal – 13 tips for a baby that refuses the breast.
https://www.bellybelly.com.au/breastfeeding/breast-refusal/ [Accessed 22nd February 2019]
Burbridge A. (2017) Nursing strikes. La Leche League GB. Available at: https://www.laleche.org.uk/nursing-strikes/ [Accessed 1st August 2019]
Coulson S. (2012) Biological nurturing: the laid-back breastfeeding revolution. Midwifery Today, 101 Available at: https://midwiferytoday.com/mt-articles/biological-nurturing/ [Accessed 1st August 2019]
Flint A, New K, Davies MW. (2016) Cup feeding versus other forms of supplemental enteral feeding for newborn infants unable to fully breastfeed. Cochrane Database Syst Rev. (8):CD005092. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD005092.pub3… [Accessed 1st August 2019]
Gonzalez C. (2014) Breastfeeding Made Easy. London: Pinter &Martin
LLLGB. (2016) My baby won’t breastfeed. Available at https://www.laleche.org.uk/my-baby-wont-breastfeed/ [Accessed 1st August 2019]
(2016) My baby won’t breastfeed. Available at https://www.laleche.org.uk/my-baby-wont-breastfeed/ [Accessed 1st August 2019]
Mohrbacher N. (2013) Is your formerly nursing baby refusing to breastfeed? Breastfeeding Reporter Blog. Available at http://www.nancymohrbacher.com/articles/2013/1/26/is-your-formerly-nursing-baby-refusing-to-breastfeed.html?rq=refusing [Accessed 1st August 2019]
NICE. (2017) Breastfeeding problems. National Institute for health and Care Excellence, Clinical Knowledge Summaries. Available at: https://cks.nice.org.uk/breastfeeding-problems#!scenario [Accessed 1st August 2019]
Pitman T, Bennett H. (2008) 0-1 year: nursing strikes; breastfeeding while baby’s falling asleep may help end a nursing strike. Today’s Parent. 7:137.
Public Health England. (ND) Breastfeeding challenges. NHS, Start 4 life. Available at: https://www.nhs.uk/start4life/baby/breastfeeding/breastfeeding-challenges/reflux/ [Accessed 1st August 2019]
UNICEF. (2016) Breastfeeding checklist for mothers – How can I tell that breastfeeding is going well? UNICEF UK Baby Friendly Initiative. Available at https://www.unicef.org.uk/babyfriendly/wp-content/uploads/sites/2/2016/10/mothers_breastfeeding_checklist.pdf [Accessed 1st August 2019]
Available at https://www.unicef.org.uk/babyfriendly/wp-content/uploads/sites/2/2016/10/mothers_breastfeeding_checklist.pdf [Accessed 1st August 2019]
UNICEF. (2018) Skin-to-skin contact. Available from: https://www.unicef.org.uk/babyfriendly/baby-friendly-resources/guidance-for-health-professionals/implementing-the-baby-friendly-standards/further-guidance-on-implementing-the-standards/skin-to-skin-contact/ [Accessed 1st August 2019]
UNICEF. (2019) Responsive bottle feeding. Available from: https://www.unicef.org.uk/babyfriendly/wp-content/uploads/sites/2/2019/04/Infant-formula-and-responsive-bottle-feeding.pdf [Accessed 1st August 2019]
Causes, Emergency Care, and Treatments
“Poor feeding in infants” is a term used to describe an infant with little interest in feeding. It can also refer to an infant who is not feeding enough to receive the necessary nutrition required for adequate growth.
Poor growth associated with lack of feeding can lead to a separate condition called failure to thrive.
Poor feeding is caused by a variety of factors. It differs from picky eating, in which a baby may reject one form of milk for another or a toddler may refuse certain foods.
No matter the precise cause of poor feeding, undernutrition is a top concern. In fact, the World Health Organization (WHO) estimates that 45 percent of child deaths are related to undernutrition.
It is important not to dismiss poor feeding as something that will improve over time. This is a critical point in your child’s life, and missing key nutrients can lead to physical and cognitive concerns.
One of the most common causes of poor feeding is premature birth. Premature babies are typically poor feeders because they often have not yet developed the skills needed to suck and swallow milk.
Still, feeding usually increases as baby grows. If your little one was born prematurely and still has feeding trouble after leaving the hospital, it’s important to continue following up closely with your pediatrician, particularly if feeding concerns worsen or do not improve.
Other causes include congenital conditions such as jaundice and infections such as viral gastroenteritis. Once these conditions are treated, poor feeding usually subsides.
Serious conditions
Poor feeding can also be caused by serious conditions, such as Beckwith-Wiedemann syndrome. This is an overgrowth syndrome that causes infants to be particularly large and grow at a considerably fast pace. It affects an estimated 1 in 13,700 newborns worldwide.
Other serious conditions include:
- congenital hypothyroidism, which occurs when the thyroid fails to develop or function properly
- other genetic conditions, including Down syndrome
- hypoplastic left heart, a rare condition that occurs when the left side of the heart fails to develop properly and is unable to pump blood to the body
- other heart defects
Less serious conditions
Other causes of poor feeding aren’t related to a congenital condition at all. Temporary illnesses can make feeding uncomfortable (and even painful) for infants.
Common ailments that get in the way of feeding include:
- diarrhea
- ear infections
- coughs and colds
- teething
When in doubt, it’s always best to double-check with a pediatrician. You don’t want to assume a minor illness when in fact there could be a serious underlying condition.
Feeding difficulty is a serious matter. When accompanied by other symptoms, emergency care may be required. Seek immediate medical attention if your baby is showing any of the following signs:
- has a fever of over 100°F (37.8°C), an emergency in babies 3 months old and younger
- is vomiting after every feeding
- is vomiting blood
- has a cough with breathing difficulties
- is crying constantly
- has bloody stool
- is wheezing
- is becoming unresponsive to touch
Poor feeding that is caused by an infection will usually stop when the infection is resolved.
Treatment of poor feeding depends on the cause. This can involve changing the feeding schedule to consist of smaller, more frequent meals. If a milk-based intolerance is suspected, your doctor will work closely with you to find a formula and feeding plan that suits your baby.
This can involve changing the feeding schedule to consist of smaller, more frequent meals. If a milk-based intolerance is suspected, your doctor will work closely with you to find a formula and feeding plan that suits your baby.
While serious cases of poor feeding require prompt medical care, other causes can be resolved at home with the advice of a pediatrician.
If your baby is breastfeeding or chestfeeding, try to avoid:
- certain medications that can enter breast milk
- applying lotions and other skin products to your breasts
- high levels of stress — this may also make your milk taste differently
Other considerations may concern formula feeding as well as infants who have started solid foods.
Formula feeding
While breastfeeding is the method of feeding for infants recommended by health agencies such as WHO, it is a fact that not all babies are successful with this method — and not all nursing parents may want or be able to breastfeed.
If your baby doesn’t seem to latch on despite repeated attempts, you may consider talking with your doctor about formula feeding. You may still be able to try breastfeeding or chestfeeding, even when supplementing with formula, if you’d like.
The key is that your baby gets adequate nutrition. A lactation consultant may be helpful, if available to you.
“Picky eating”
After baby reaches 6 months of age, your pediatrician may encourage you to introduce solids to their diet. While solids shouldn’t replace breast milk at this phase of your child’s life, most infants require additional nutrients around the 6-month mark.
Examples include:
- rice cereal
- pureed fruits and vegetables
- pureed or soft meats
Introducing solid foods can be exciting for both caregiver and child. However, some infants don’t take to solids as readily as other babies.
This can be alarming, but the issue may be solved by:
- mixing cereal with solid foods
- offering solids in small increments
- only giving solids two to three times per day
- starting with one food at a time, then introducing others as your baby gets used to solids
When an infant doesn’t like solids, it’s easy to jump to the conclusion that they are a “picky eater. ” However, this phase doesn’t usually start until your baby becomes a toddler.
” However, this phase doesn’t usually start until your baby becomes a toddler.
Stress management
When your baby is eating poorly, it’s easy to get stressed out. This is especially true for new parents who may not yet know the distinctions between serious conditions and minor feeding concerns.
Remember that stress can worsen feeding concerns. It may interfere with attempts at feeding if your infant senses something is wrong.
Managing your stress won’t treat all causes of poor feeding, but it can help in many cases.
It’s difficult to find time for yourself during this busy stage of your life — even a few minutes a day can help. When you feel stress coming on during feedings, take a moment for some deep breathing.
Poor feeding in infants can lead to serious issues, such as malnutrition and stunted growth. It is essential that babies consume and digest the necessary nutrients to thrive and develop.
Any infant who is feeding poorly should be taken to a pediatrician for evaluation. After a proper diagnosis, treatment may be necessary.
After a proper diagnosis, treatment may be necessary.
In other cases, poor feeding can be resolved through refined techniques and perseverance at home. If you suspect feeding difficulties may be causing other concerns, call a doctor right away.
Solutions to six breastfeeding problems in the first week
Are you having difficulty breastfeeding your newborn baby? Read on for expert advice on tackling the main challenges of the first week of breastfeeding.
Share this information
Cathy Garbin, child health nurse, midwife and lactation consultant:
Cathy, a mother of two, was a research fellow at the renowned Human Lactation Research Institute, founded by Peter Hartmann, for seven years, providing support to breastfeeding mothers in clinics and at home. Today, she still works as a family counselor, and also conducts seminars for attending physicians and speaks at international conferences.
Breastfeeding is not always easy, so if
you are having difficulty, know that you are not alone. A US study found that out of 500 new mothers surveyed, 92% experienced breastfeeding problems by the third day. 1 Fortunately, most early breastfeeding problems are easy to resolve. Below you can read recommendations for solving the main problems that mothers often face in the first week of feeding.
A US study found that out of 500 new mothers surveyed, 92% experienced breastfeeding problems by the third day. 1 Fortunately, most early breastfeeding problems are easy to resolve. Below you can read recommendations for solving the main problems that mothers often face in the first week of feeding.
Problem #1. Breastfeeding hurts!
Pain during feeding is usually associated with tenderness or inflammation of the nipples, especially when milk "comes" on the second to fourth day after birth. 2 The baby will beg for a breast every couple of hours, and this can quickly aggravate the problem: some mothers' nipples crack, bleed, or blister. This is, of course, very annoying.
Solutions 3
- Check how the baby latch on. An incorrect latch is one of the most common causes of pain during breastfeeding. A newborn baby should take most of the lower half of the areola (dark skin around the nipple) into his mouth, and your nipple should rest against his palate, supported from below by the tongue.

- Contact a lactation consultant or healthcare professional to make sure your baby's mouth and torso are properly positioned during feeding and there are no other latch-on problems. The doctor may also examine the baby's mouth for physical abnormalities.
- Try other feeding positions. Reclining, cross cradle, underarm, or lying positions can relieve pressure on the most painful areas of your breasts.
- Gently wipe soaked nipples with water-soaked cotton swabs after each feed to remove milk residues that can cause infection.
- Air dry nipples or blot with a clean, soft muslin or flannel cloth to prevent bacterial growth in a humid environment. Use disposable or reusable bra pads to absorb leaking milk and remember to change them regularly.
- Soften your nipples. An ultra-pure lanolin treatment will help relieve inflammation and dry skin. You can also apply a few drops of your own breast milk to your nipples.
 In both cases, you do not have to wash your breasts before the next feeding. You can also apply refrigerated hydrogel pads* to your nipples. They soothe the nipples and help relieve pain during feeding, as well as speed up healing.
In both cases, you do not have to wash your breasts before the next feeding. You can also apply refrigerated hydrogel pads* to your nipples. They soothe the nipples and help relieve pain during feeding, as well as speed up healing. - Protect your nipples. Nipple shields* protect the sore area from rubbing against clothing.
- Be patient. The inflammation usually resolves after a few days as your body adjusts to breastfeeding and your baby learns to suckle.
- Seek medical attention, if pain during feeding does not go away after a few days. Constant inflammation of the nipples may indicate an infection that requires prompt treatment.
Problem #2. Baby doesn't latch on properly
Some newborns do not latch on properly right away. Maybe both of you just need more time to learn how to breastfeed, or maybe the baby was born prematurely, feels unwell after a difficult birth, or mom has flat or inverted nipples.
Solutions
- Contact a lactation consultant or healthcare professional who can help identify the cause of the problem and suggest solutions.
- Flat or inverted nipples must be pulled out. Nipple formers* fit comfortably in the bra and apply gentle pressure to the nipples to help them come out for easier feeding.
- Try different positions and ways to support your newborn. The baby needs to feel supported. He must be comfortable and breathe freely in order to suckle properly. Do not hold the child by the head and do not put pressure on it. Lean back and let your child take the lead. This stimulates his natural reflexes and helps him find and latch on to his breasts. 4
- When feeding, try to find the optimal position. Instead of putting your baby on and off, stressing both of you, try to position him in a way that is easy and comfortable for him.
 Hold the torso and legs of the baby close to you, support him by the shoulders and hold him firmly so that he feels safe. Let the baby's head rest freely on your arm so that he can tilt it back slightly and breathe freely. The chin should be pressed against your chest. If these small adjustments don't make feeding more comfortable for your baby, seek help from a lactation consultant or healthcare professional.
Hold the torso and legs of the baby close to you, support him by the shoulders and hold him firmly so that he feels safe. Let the baby's head rest freely on your arm so that he can tilt it back slightly and breathe freely. The chin should be pressed against your chest. If these small adjustments don't make feeding more comfortable for your baby, seek help from a lactation consultant or healthcare professional. - Use nursing pads. If your baby is having difficulty latch-on, a lactation consultant or healthcare professional may suggest trying nursing pads*. A nipple with an overlay is more convenient to take in the mouth, so it is larger and more rigid. Do not use nursing pads for a long time.
Problem #3. Not enough breast milk
You will produce little breast milk at the very beginning, as the hormonal changes that trigger milk production occur slowly and do not end until the second or fourth day after birth. 2 You may be worried that your baby is not getting enough milk, but in the early days his stomach is still too small and feedings are frequent, so don't worry. The only things to worry about these days are excessive weight loss, too few wet and soiled diapers, or signs of dehydration in the baby. For more information on how often a newborn should urinate and void, see Breastfeeding Newborns: What to Expect in the First Week.
The only things to worry about these days are excessive weight loss, too few wet and soiled diapers, or signs of dehydration in the baby. For more information on how often a newborn should urinate and void, see Breastfeeding Newborns: What to Expect in the First Week.
Solutions
- Contact a Lactation Consultant or your healthcare provider who can determine if you have problems with milk production. The sooner you do this, the better.
- Feed your baby on demand, not on a schedule. In the first week after birth, your baby will ask to breastfeed every two to three hours (or more often!), both day and night. Such frequent feeding helps to establish the production of breast milk.
- Take care of yourself. It's not always easy with a newborn, but try to rest whenever you can, eat right, and accept any help around the house or with older children that your loved ones can give you to fully focus on breastfeeding.
- Try expressing milk. If a baby is feeding frequently but not gaining any weight, a lactation consultant or doctor may recommend pumping to increase breast milk production. If milk is not coming out at all, you can try the Medela Symphony Dual Electric Clinical Breast Pump**. It features an Initiate program that mimics a baby's natural sucking rhythm for the first few days.
Problem #4. Breast full and heavy
Your breasts will become fuller and heavier as milk comes in.
If the baby suckles well and often, this should not cause any problems. However, in some women, the breasts become so full that they become hard and painful. This condition, called breast swelling, can cause discomfort. The swollen chest seems to be “burning”, now all the activity of your body is concentrated in it, resembling a busy traffic at rush hour. Fortunately, this condition usually resolves within 24 to 48 hours. However, due to the swelling of the mammary glands, the nipples can become flat and the baby may have difficulty latch-on. 5
5
Solutions
- Feed your baby often. Try to breastfeed at least 8-12 times a day. This is the main way to alleviate this condition. For more tips and tricks, see the article on Breast Swelling. 6.7
- Call your healthcare provider, if symptoms persist for more than 48 hours, you have a fever, or your baby is unable to breastfeed due to swelling.
Problem #5. Milk is leaking
Breast leakage is very common in the early days of breastfeeding when milk production begins. Milk may leak from one breast while you are feeding the other, when you sleep on your stomach, or when something accidentally triggers the milk flow reflex, such as when you hear a baby crying in a store. The leakage usually stops after about six weeks.
Solutions
- Protect clothes from stains will help disposable or reusable bra pads to be used day and night.
- Don't waste precious drops! Breast milk collection pads* fit inside the bra and allow you to collect any leaking milk. This is a very useful thing when there is too much milk and the pads are not absorbing well, or when one breast is leaking while you are feeding the other. If you want to save the collected milk, use only the milk collected at the feeding. Place it in a sterile container and refrigerate immediately if you are not supplementing with it right away. Collected milk must be used within 24 hours. The breast milk collection sleeves should not be worn for more than two to three hours at a time.
Problem #6. There seems to be too much milk
Sometimes when milk comes in, too much is produced! In the first few weeks there may be an overabundance of milk, but usually everything returns to normal soon. 7 Up to this point, the breasts may be heavy and sore almost all the time, even immediately after a feed, and a lot of milk may leak. A strong flush can cause a baby to cough or choke, vomit immediately after a feed, have tummy discomfort, or have hard, frothy, greenish stools. These are all signs that you are having too much milk, but the problem may resolve itself as your breasts get used to the new function.
A strong flush can cause a baby to cough or choke, vomit immediately after a feed, have tummy discomfort, or have hard, frothy, greenish stools. These are all signs that you are having too much milk, but the problem may resolve itself as your breasts get used to the new function.
Solutions
- Express some milk by hand at the beginning of each feed to ease the force of the flush.
- Try to feed while leaning back: this will help your baby control the flow of milk. The "cradle" position is also good: hold the baby obliquely by the shoulders so that the head can lean back slightly while on your arm. The torso of the baby will be located diagonally on you.
- Be kind and patient. Let your baby rest and absorb milk both during and after feeding. Don't move your baby too much or too fast, as this can make him nauseous. As the baby grows, he will learn to better cope with the rush of milk, which is likely to weaken anyway.
- Use the towel or swaddle to soak up spilled milk if the baby can't handle the flush, and place the breast milk collection pad on the other breast to catch any spilled milk.
- Contact a lactation consultant or doctor if problems persist after a few weeks . He will examine you and may suggest one-sided feedings or hourly breast changes (“breast duty”) to reduce your milk supply.
Related materials: Difficulties in breastfeeding in the next few weeks and problems with breastfeeding after the first month
Literature
1 Wagner EA et al. Breastfeeding concerns at 3 and 7 days postpartum and feeding status at 2 months. Pediatrics . 2013: peds -2013. - Wagner I.A. et al., "Breastfeeding Problems at Days 3 and 7 of a Child's Life and Type of Feeding at 2 Months". Pediatrix (Pediatrics). 2013:e865–e875.
2 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
3 Cadwell K. Latching - On and Suckling of the Healthy Term Neonate: Breastfeeding Assessment. J Midwifery & Women ’ s 2007;52(6):638-642. — Cadwell, K., "Latching and sucking in healthy newborns: evaluation of breastfeeding." F Midwifery Women Health. 2007;52(6):638-642.
4 Colson SD et al. Optimal positions for the release of primitive neonatal reflexes stimulating breastfeeding. Early Hum Dev . 2008;84(7):441-449. - Colson S.D. et al., "Optimal Positions for Provoking Primitive Innate Reflexes to Induce Breastfeeding." Airlie Hume Dev. 2008;84(7):441-449.
2008;84(7):441-449. - Colson S.D. et al., "Optimal Positions for Provoking Primitive Innate Reflexes to Induce Breastfeeding." Airlie Hume Dev. 2008;84(7):441-449.
5 Jacobs A et al. S3-guidelines for the treatment of inflammatory breast disease during the lactation period. Geburtshilfe Frauenheilkd. 2013;73(12):1202-1208. - Jacobs A. et al., "Recommendations S -3 for the treatment of inflammatory diseases of the breast during breastfeeding. Geburtskhilfe und Frauenheilkünde. . ABM Clinical Protocol# 4: Mastitis , Revised MARCH 2014. Breastfeed - 9020: 5): 5) H., Academy of Breastfeeding Protocol Committee, AVM Clinical Protocol #4: Mastitis, March 2014 edition of Brestfeed Med (Breastfeeding Medicine). 2014;9(5):239-243.
7 Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol # 20: Engorgement. Breastfeed Med . 2009;4(2):111-113. - Protocol Committee of the Academy of Breastfeeding Medicine, "AVM Clinical Protocol No. 20: Engorgement, Revision 2016". Brestfeed Med (Breastfeeding Medicine). 2009;4(2):111-113.
Breastfeed Med . 2009;4(2):111-113. - Protocol Committee of the Academy of Breastfeeding Medicine, "AVM Clinical Protocol No. 20: Engorgement, Revision 2016". Brestfeed Med (Breastfeeding Medicine). 2009;4(2):111-113.
Read instructions before use. Consult a specialist about possible contraindications.
* RU No. ФСЗ 2010/07352 dated 07/19/10
** RU No. ФСЗ 2010/06525 dated 03/17/2021
Feeding the baby with breast milk on demand
You can often hear from a nursing mother: "I feed on demand, my baby requires a breast every 3.5 hours." Or: “I have always fed on demand. In a year, we already had 1 feeding in the evening, and my child calmly refused to breastfeed. Before talking about the demand of the child, it is necessary to find out what modern women mean when they say - "I breastfeed."
Modern mothers consider breastfeeding necessary for feeding their baby. Just for feeding. Breast milk is food, the mother supplies the baby with the nutrients necessary for growth and development. When a baby suckles at the breast, he eats. Breastfeeding makes sense only as a process of supplying proteins, fats, carbohydrates, vitamins and microelements.
Breast milk is food, the mother supplies the baby with the nutrients necessary for growth and development. When a baby suckles at the breast, he eats. Breastfeeding makes sense only as a process of supplying proteins, fats, carbohydrates, vitamins and microelements.
During suckling, the baby receives the nutrients it needs with mother's milk. This is the absolute truth. There is another unconditional truth, which is not given any importance in modern society, it is not taken into account and is not considered. Breastfeeding for a child is communication with the mother. We need to figure out how the child understands feeding on demand? Can he understand anything at all? Is there any difference for him how he is fed, for 15-20 minutes after 3.5 hours or in some other way?
What is on-demand feeding
On-demand feeding of a newborn baby means putting it to the breast for every squeak or search. Squeak and search movements in newborns, even as early as the second or third day of life, begin to appear much more often than after 3.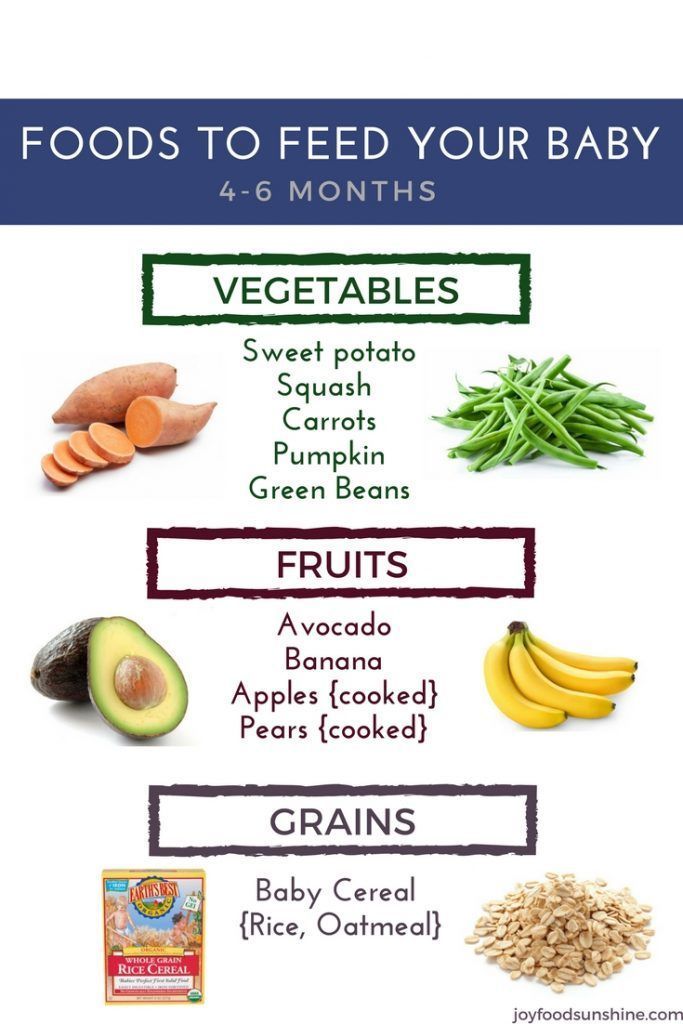 5 or 2.5 hours. The need for attachments increases rapidly, and by the 10-12th day of life, the need to attach to a child may occur 15-16 or more times a day. Applications vary in duration. The baby can fall asleep and sleep while sucking for, for example, 1.5-2 hours. Can release the breast after 1-2 minutes. And then ask her again. Why does a child need such frequent contact with his mother's breast?
5 or 2.5 hours. The need for attachments increases rapidly, and by the 10-12th day of life, the need to attach to a child may occur 15-16 or more times a day. Applications vary in duration. The baby can fall asleep and sleep while sucking for, for example, 1.5-2 hours. Can release the breast after 1-2 minutes. And then ask her again. Why does a child need such frequent contact with his mother's breast?
That's why. Being in the mother's belly, in a calm, familiar environment, listening to the noises of the mother's body, being in a warm, cramped, confined space, the baby sucked his fist, fingers, loops of the umbilical cord, swallowed amniotic fluid. Learned to suck and swallow. After birth, experiencing discomfort for any, the most insignificant reason, the baby tries to get rid of it. You can get rid of discomfort by getting into the usual conditions of a comfortable stay. The only place where the baby after birth can feel the sensations familiar to him is in the arms of the mother. The only familiar action is sucking. The only familiar taste and smell is the taste and smell of milk and lube in the areola. Milk and lubricant have an odor and taste similar to the taste and smell of amniotic fluid. Therefore, experiencing discomfort, the baby squeaks, or begins to look for an object to suck with his mouth. Ideally, it is immediately applied to the chest. The baby becomes warm, cramped, he hears the beating of his mother's heart, breathing, grumbling in the intestines, he sucks and feels the familiar taste and smell. If such an action happens constantly, the baby gains confidence, no matter what happens, he will solve all his problems with his mother. The place of comfort is now under the breast, and you can suck on the breast.
The only familiar action is sucking. The only familiar taste and smell is the taste and smell of milk and lube in the areola. Milk and lubricant have an odor and taste similar to the taste and smell of amniotic fluid. Therefore, experiencing discomfort, the baby squeaks, or begins to look for an object to suck with his mouth. Ideally, it is immediately applied to the chest. The baby becomes warm, cramped, he hears the beating of his mother's heart, breathing, grumbling in the intestines, he sucks and feels the familiar taste and smell. If such an action happens constantly, the baby gains confidence, no matter what happens, he will solve all his problems with his mother. The place of comfort is now under the breast, and you can suck on the breast.
This whole process is justified from a biological point of view. A newborn child does not feel the feeling of hunger, this feeling is not formed in him. It will begin to form at about two months of age. How to feed a creature that does not experience hunger ?! How to encourage him to take some action to get food? This can be done only at the expense of some other incentives. This stimulus for the newborn is constant bodily discomfort, thanks to which he wants to suckle all the time! The most intense, frequent and prolonged sucking in infants is observed in the first two or three months of life. It is in these first months that the main weight gain of the baby occurs.
This stimulus for the newborn is constant bodily discomfort, thanks to which he wants to suckle all the time! The most intense, frequent and prolonged sucking in infants is observed in the first two or three months of life. It is in these first months that the main weight gain of the baby occurs.
Feeding in the first month
Baby falls asleep with the breast in his mouth, sleeps sucking for a while. Falling asleep deeply, lets go of the chest. After sleeping for a while, he wakes up, and is applied on waking. After sleep, he can stay awake for some time, for example, an hour and a half. During wakefulness, he may feel discomfort 2-3 times, for example, from a completely natural desire to pee, and having called his mother for help, having kissed for a couple of minutes, he will do his deeds. Then he will want to sleep, feel discomfort and, kissing his chest, will again fall asleep sucking. After some time, he will wake up and attach again. Then again a little "walk". And after some time, he will fall asleep at the chest again.
The daytime naps of a one-month-old baby feeding on demand vary in duration and number. There can be 4-6 dreams during the day, and they can last from 5-15 minutes to 2-2.5 sometimes 3 hours. "Around" each dream, the baby is applied to the chest, and applied between dreams several times. At night, the child falls asleep at the breast. Usually in the early morning hours, he begins to fuss and apply. In the morning, he almost never fully wakes up. The baby sleeps, from time to time, sucking on his mother's breast. Waking up in the morning, the baby is again applied to the chest. If you count all the attachments that have happened in a baby of one month of age, then approximately 16-20 attachments are obtained. This is how a newborn human cub behaves if it is given the opportunity to behave in accordance with physiological and psychological needs, which, by the way, are genetically determined. The child of the first months of life does not separate his personality from the personality of the mother and from her breast.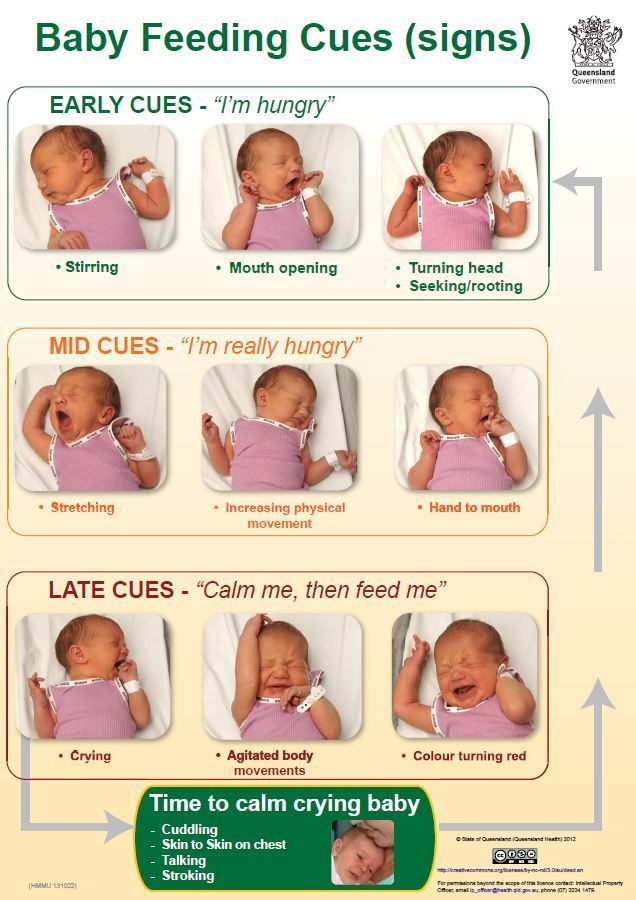 Mom and her breasts, and everything connected with them, are the universe of the baby and himself.
Mom and her breasts, and everything connected with them, are the universe of the baby and himself.
In most cases, a modern woman, being afraid to “accustom a child to hands”, strives to limit his requests for sucking. A pacifier and a bottle of tea or water come to her aid in this matter. They, too, can be sucked ... The need for sucking seems to be satisfied. But only the need for communication with the mother during suckling is not satisfied, the peculiar chain of mutual assistance and cooperation between mother and baby is destroyed, the formation of maternal affection and concentration is disrupted. Is the difference in the two actions noticeable to the reader: the baby cried, the mother took him, put him to her chest and started rocking him, or gave him a pacifier and started rocking the stroller, even with the words “Why are you crying, my sun?”
The modern woman who gives a pacifier and pumps a stroller is not a bad person who deliberately harms an infant. She is simply in captivity of prejudices regarding the relationship between mother and baby. She does not know how to behave correctly, does not know what to do in accordance with the natural needs of the child. If you tell her what the child really needs, she will exclaim in horror: “What is it, don’t let him get away with?!” Indeed, the child of the first months of life must not be let off the hook. For a woman who does not know how to comfortably carry a baby, and who does not know how to feed him in various positions (sitting, lying, standing and even moving), this can be very difficult. Especially if she is not sure of the correctness of her actions.
She does not know how to behave correctly, does not know what to do in accordance with the natural needs of the child. If you tell her what the child really needs, she will exclaim in horror: “What is it, don’t let him get away with?!” Indeed, the child of the first months of life must not be let off the hook. For a woman who does not know how to comfortably carry a baby, and who does not know how to feed him in various positions (sitting, lying, standing and even moving), this can be very difficult. Especially if she is not sure of the correctness of her actions.
An action that should become automatic for the mother of a newborn: when the baby cries or shows other signs of anxiety, put the baby to the breast.
What's next?
The baby is growing. A fairly stable rhythm of daytime sleep begins to form in him, and a 3-4-month-old baby behaves quite differently from a newborn. Feeding on demand at this age looks something like this...
- At three months, the baby has 10-12 feeds during the day and 2-4 at night.
 There are frequent applications for a short time, but their number is reduced. There may be a long night break in feedings, about 5 hours, but this is very rare. Much more often the night break is 2.5-3.5 hours. By this age, the baby's body is noticeably rounded.
There are frequent applications for a short time, but their number is reduced. There may be a long night break in feedings, about 5 hours, but this is very rare. Much more often the night break is 2.5-3.5 hours. By this age, the baby's body is noticeably rounded. - At four months, the baby begins to breastfeed noticeably less frequently. The main feedings are associated with sleep: the baby suckles before bedtime, during awakening and during sleep, both daytime and nighttime. In this regard, he has a fairly accurate feeding regimen. And many babies stop breastfeeding when they wake up after daytime sleep, sometimes as early as 2.5-3 months.
- At five months, the baby has 8-10 daytime feedings and 2-3 nighttime feedings, as well as in the fourth month of life, they are organized around dreams - the baby eats when going to bed and some babies suckle when they wake up.
- At six months, the feeding regimen changes. The most active sucking shifts to the last 2-3 hours before waking up from a night's sleep.
 The period of daytime wakefulness can be divided into two periods: in the morning, when the baby sucked during the night is rarely applied to the breast, and in the evening, when attachments become very frequent. In total, there can be 7-10 day applications and 3-4 night applications. At this age, the baby begins a period of acquaintance with new food - pedagogical complementary foods. Sometimes there are attachments associated with the introduction of complementary foods, the baby “washes down” samples of new food with mother's milk. But many children do not want to drink complementary foods. When complementary foods are introduced to an on-demand baby, it is never meant to replace feedings with complementary foods. This is practically impossible, because the main feedings of the baby are associated with sleep, and mother's breakfasts, lunches and dinners, during which the baby gets acquainted with new food, are located between the baby's dreams, during his wakefulness.
The period of daytime wakefulness can be divided into two periods: in the morning, when the baby sucked during the night is rarely applied to the breast, and in the evening, when attachments become very frequent. In total, there can be 7-10 day applications and 3-4 night applications. At this age, the baby begins a period of acquaintance with new food - pedagogical complementary foods. Sometimes there are attachments associated with the introduction of complementary foods, the baby “washes down” samples of new food with mother's milk. But many children do not want to drink complementary foods. When complementary foods are introduced to an on-demand baby, it is never meant to replace feedings with complementary foods. This is practically impossible, because the main feedings of the baby are associated with sleep, and mother's breakfasts, lunches and dinners, during which the baby gets acquainted with new food, are located between the baby's dreams, during his wakefulness. - At seven months, the frequency of applications is about the same.
- At eight months, the feeding regimen changes. Since the baby shows high motor activity and is very busy exploring the surrounding space, in the daytime he forgets to breastfeed. In this regard, the number of daily feedings can be reduced to 6-8 times. The baby compensates for the reduction in daytime feedings by increasing the frequency and duration of nighttime feedings up to 6 times.
- In the second half of the year, babies who stopped breastfeeding when waking up after daytime naps recall this habit again. The baby’s daytime sleep in the second half of life, as well as in the region of a year and older, looks something like this: the baby falls asleep sucking, sleeps quietly for a while, for example 1-1.5 hours, then starts tossing and turning, fiddling, worrying, at this moment the mother lies down next to , gives him a breast and the baby can fill up 10-15-30 minutes sucking. Mom may well use this time for her own rest - lie down, read, while the baby sleeps while sucking.
 I know my mother, a lover of embroidery, who used this time specifically for embroidery ...
I know my mother, a lover of embroidery, who used this time specifically for embroidery ... - Breastfeeding becomes more frequent at nine to ten months. In the daytime, this is 4-6 full feedings and about the same number of attachments for various reasons. The baby has new reasons for attachment. If, during active actions to master the world, the baby fills a bump or gets scared, he calms down with his mother's breast. There may be situations when you can comfort the baby by sitting next to him and hugging him. At night, 4-6 feedings remain, the baby begins to suckle more actively in the morning between 3 and 8 hours.
- At eleven months, a baby can already have 2-3 complete complementary foods. Initiation to adult food in the mind of a child is not associated with breastfeeding: attachment to the mother's breast is something other than the desire to get enough of the product they like. As a rule, after the baby has eaten, he feels the need to attach himself to the breast.
 The number of daily feedings remains the same in the child, but the number of short-term attachments increases. There are active mid-morning feedings between 4 and 8 o'clock in the morning.
The number of daily feedings remains the same in the child, but the number of short-term attachments increases. There are active mid-morning feedings between 4 and 8 o'clock in the morning. - At ten or twelve months, the baby, if he is already walking, can sometimes breastfeed every time he comes to his mother, i.e. about every 15-30 minutes. Attachments around dreams and night sucking persist. Therefore, if a mother says that a child suckles once or twice a day, this means that there is no feeding at the request of the child. There are restrictions imposed by the mother, with which the baby has come to terms. He treats breast sucking like food, sucks on a pacifier or a finger to fall asleep or soothe, or falls asleep just like that, without calming down.
- At twelve months, the baby is applied in about the same way.
- At the age of one and a half years, there may already be one daytime nap, so there are fewer attachments associated with sleep. Preserved for morning sucking.
 The baby is very free with his mother's breasts. Sometimes it happens that he comes up to suck just for pleasure. For example, like this: he comes up, climbs on his knees, looks into his mother’s face, smiles, starts to swarm in his shirt, gets breasts, smiles at his breasts, sucks for 30 seconds and leaves.
The baby is very free with his mother's breasts. Sometimes it happens that he comes up to suck just for pleasure. For example, like this: he comes up, climbs on his knees, looks into his mother’s face, smiles, starts to swarm in his shirt, gets breasts, smiles at his breasts, sucks for 30 seconds and leaves.
As for the number of feedings per day when feeding a child on demand, their number is almost never less than 12. A newborn has 12 or more feedings, mostly they are all associated with dreams. And a child, say 1.5-2 years old, can also have about 12 attachments, only 3-4 are associated with sleep, and the rest are short-term attachments for various reasons. I suggest to all mothers reading this text - do not count the application, do not notice their duration. Breastfeed your baby as often as he asks, when you feel the need to.
Mothers who do not think about breastfeeding without looking at the clock may get the impression that when feeding on demand, the mother can do nothing but feed the baby. This is not true. After the birth of a baby, a mother begins another life, she is called life with a baby. That's all. The child is with the mother, not the mother with the child! Feel the difference! You need to be able to organize your life in a different way, in the first months, of course, the help of loved ones is very necessary. In the tradition of many peoples, it was customary for the first 40 days after childbirth to remove a woman from any housework and household chores, she was engaged only in a child. In some nations, objects that the mother of a newborn touched were considered “unclean”, therefore, they preferred to protect the mother from the rest of the household, allocating her a separate “corner” of the house, where no one bothered her and she did not interfere with anyone. Among the Slavs, such a restrictive custom was called a six-week. By 1.5-2 months, the rhythm of daytime dreams begins to form, and the baby has a kind of “regime”, the mother becomes more free.
This is not true. After the birth of a baby, a mother begins another life, she is called life with a baby. That's all. The child is with the mother, not the mother with the child! Feel the difference! You need to be able to organize your life in a different way, in the first months, of course, the help of loved ones is very necessary. In the tradition of many peoples, it was customary for the first 40 days after childbirth to remove a woman from any housework and household chores, she was engaged only in a child. In some nations, objects that the mother of a newborn touched were considered “unclean”, therefore, they preferred to protect the mother from the rest of the household, allocating her a separate “corner” of the house, where no one bothered her and she did not interfere with anyone. Among the Slavs, such a restrictive custom was called a six-week. By 1.5-2 months, the rhythm of daytime dreams begins to form, and the baby has a kind of “regime”, the mother becomes more free.
For a mother who can't imagine breastfeeding without looking at the clock, and who is sure that the “right” baby is the baby lying quietly in her crib all the time, feeding on demand will be a complete hassle.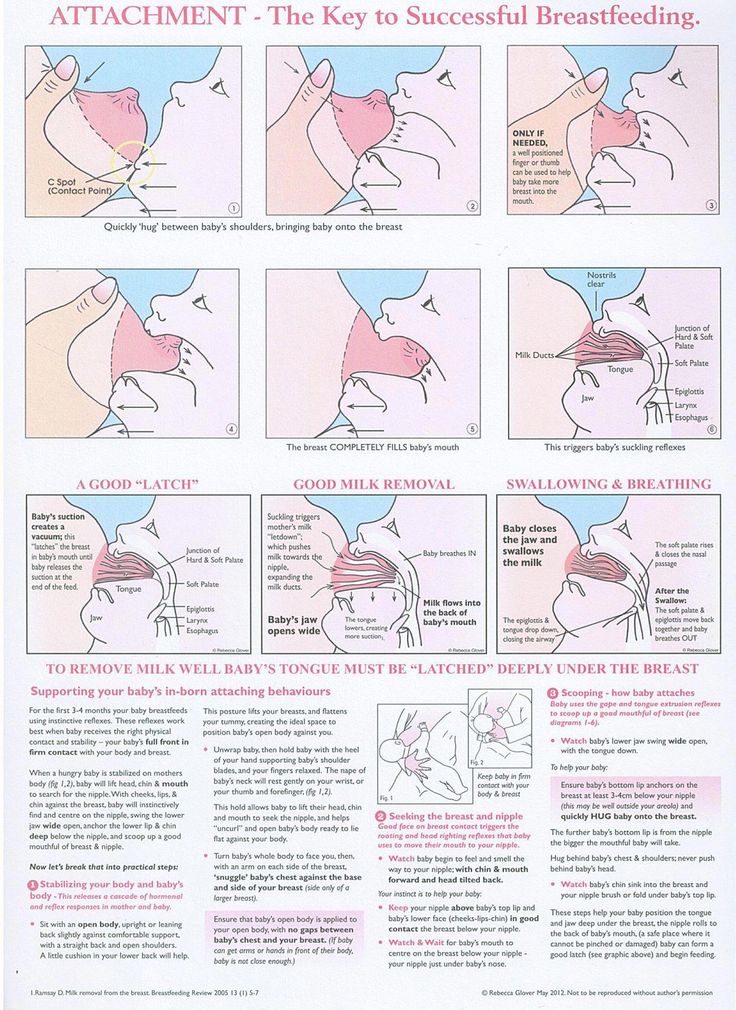 It will be much easier for such a mother if she stops looking at the clock and ties the baby to herself with a large scarf or uses a patchwork holder (sling). It will become easier for her if she stops running between the nursery and the kitchen, but takes the baby with her to the kitchen and carries him around the house with her, doing housework, in a box, a cradle, a special chair, if she tries not to put him off often, and pick up as soon as possible, postponing the baby only in case of emergency and not for long.
It will be much easier for such a mother if she stops looking at the clock and ties the baby to herself with a large scarf or uses a patchwork holder (sling). It will become easier for her if she stops running between the nursery and the kitchen, but takes the baby with her to the kitchen and carries him around the house with her, doing housework, in a box, a cradle, a special chair, if she tries not to put him off often, and pick up as soon as possible, postponing the baby only in case of emergency and not for long.
Breastfeeding is not the same as house arrest. In the conditions of modern society, it is possible to organize the exit of a nursing mother to work from about 6 months of age of the baby. If necessary, you can start working from the age of 4 months, but, of course, it is better not every day of the week and not full time. It is the responsibility of a breastfeeding consultant to help a mother organize her return to work.
Sometimes, when counseling mothers on breastfeeding, I suggest that they forget for a second that they are already living in the 21st century. I propose to return, for example, to the cave and ask what they will do if the child woke up at night, how to calm him down? If you are walking through the forest and trying not to attract the attention of predators, how to make the baby silent? If the child is thirsty, what will you give him? What is the baby used to, for thousands of years of its existence? To the fact that he sleeps on his mother while she wanders through the forest with a digging stick in search of roots, and wakes up when mother stops. Since mom stopped, then there is time to wake up and suck. Therefore, even now the child sleeps well, tied to the mother with a patchwork holder, wakes up when the mother, having done a few household chores, sits in a chair to take care of the baby.
I propose to return, for example, to the cave and ask what they will do if the child woke up at night, how to calm him down? If you are walking through the forest and trying not to attract the attention of predators, how to make the baby silent? If the child is thirsty, what will you give him? What is the baby used to, for thousands of years of its existence? To the fact that he sleeps on his mother while she wanders through the forest with a digging stick in search of roots, and wakes up when mother stops. Since mom stopped, then there is time to wake up and suck. Therefore, even now the child sleeps well, tied to the mother with a patchwork holder, wakes up when the mother, having done a few household chores, sits in a chair to take care of the baby.
Some mother, reading about the cave, will be offended, saying that she is a civilized creature. But please think. Man, mother's breast and mother's milk have been created by evolution over millions of years. They are made for each other. Baby food has created progress and more recently. The skills of motherhood and breastfeeding have also been lost by our society quite recently. A person is not physiologically adapted to artificial feeding and a pacifier. The mother's breast will not produce enough milk at 6-7 feedings per day. Nature did not know, when creating man as a mammal, that the time would come when the need for breastfeeding would be satisfied by some kind of pacifiers and nipples.
Baby food has created progress and more recently. The skills of motherhood and breastfeeding have also been lost by our society quite recently. A person is not physiologically adapted to artificial feeding and a pacifier. The mother's breast will not produce enough milk at 6-7 feedings per day. Nature did not know, when creating man as a mammal, that the time would come when the need for breastfeeding would be satisfied by some kind of pacifiers and nipples.
Changes that occur during the formation of the personality of a child who did not have full contact with the mother during prolonged breastfeeding are noted by modern research by psychologists and sociologists. These are changes with a minus sign. It would be better if they were not, these changes.
Breastfeeding is important not only for the baby, it is also important for the mother. During on-demand feeding, the woman's feelings change, a stronger attachment to the baby is formed, the woman becomes more sensitive to the needs of the baby.