5 month baby not feeding well
Why Is Baby Not Drinking Enough Milk? – Baby Care Advice
It’s obvious when a bottle-fed baby is not drinking as much milk as expected. But does this mean she’s not drinking enough? Maybe ‘yes’. Maybe ‘no’. This article explains how to tell if your baby is underfeeding and the various reasons why babies don’t drink enough milk.
How to tell if baby is underfeedingAre you worried that your baby is not drinking enough because she’s not drinking as much as you have been told she needs? Or because her weight gain is low?
The fact that a baby doesn’t eat as much or gain as much as expected is not proof that she’s not eating enough. It could be that her milk needs have been overestimated or that expectations about her growth are unrealistic given her circumstances.
The first step toward solving this puzzle is to identify if your baby is underfeeding. Underfeeding means a baby is not ingesting enough milk to meet her growth and energy needs.
So how can you tell if your baby is underfeeding? There are physical signs and behavior that indicate if a baby’s nutritional needs are met or not. These are listed in the table below.
Signs of a baby’s nutritional statusGrowth is not a reliable indicator of a baby’s current nutritional state. A baby’s prior growth could be poor but the problem having caused this may be resolved. So, while a baby might be underweight, she could still be well fed at present. Or it could be that baby’s growth is perceived as being poor when in reality it’s not. There are a number of reasons why a thriving baby’s weight gains can appear to be poor. (See Growth false alarms and Variations of normal growth.)
If you have now confirmed that your baby is not drinking enough milk to meet her nutritional needs, the next step is to identify the cause.
Reasons for baby not drinking enoughThere are a number of reasons why a baby might not drink enough to meet her needs; these include:
- Baby chooses to avoid feeding.

- Baby is too tired to feed effectively.
- Baby has poor appetite.
- Baby is prevented from effectively accessing the food (something is making it difficult for her to drink enough).
- Baby has impaired ability to suck.
- Baby is not offered enough milk (breastmilk or infant formula).
Why would a hungry baby choose to avoid feeding? If she finds the experience of feeding to be unpleasant, stressful, or painful she might. Reasons a baby may prefer to go hungry than to eat include:
- Feeding aversion
- Sensory processing disorder
A feeding aversion is one of the most common reasons for physically well babies and children to reject bottle/ breast or solids and consume less than they need. An unresolved feeding aversion can cause poor growth
Babies can become averse to one, two or all three feeding methods, i. e., breastfeeding, bottle-feeding or eating solids. Typically, a baby who has developed a feeding aversion willingly eats only when ravenous, and then only a little. She’s tense and upset at feeding times. She might scream at the sight of the bottle, when placed into a feeding position, or at some point during the feed, for example after being burped. She stops sucking and turns away or arches her back in an upset manner. Some babies, who have become averse to feeding will feed better in a sleepy state because they’re then less aware that they’re feeding.
e., breastfeeding, bottle-feeding or eating solids. Typically, a baby who has developed a feeding aversion willingly eats only when ravenous, and then only a little. She’s tense and upset at feeding times. She might scream at the sight of the bottle, when placed into a feeding position, or at some point during the feed, for example after being burped. She stops sucking and turns away or arches her back in an upset manner. Some babies, who have become averse to feeding will feed better in a sleepy state because they’re then less aware that they’re feeding.
Because a feeding aversion means a baby tries to avoid eating and doesn’t willingly eat enough for healthy growth, parents understandably feel they have no option other than to continue to pressure their baby to eat. But this makes the situation worse. More often than not the reason babies and children don’t want to eat is because they’re repeatedly pressured to eat.
Sensory processing disorderBabies can develop an oral aversion due to a sensory processing disorder. Babies who have a sensory processing disorder perceive sensations differently to others and become upset by situations and things that don’t trouble most other babies. They may find a particular smell, taste, or feel of certain foods or feel of the nipple of a feeding bottle and other objects in their mouth objectionable. Or they may be less aware or hypersensitive to the sensation of hunger.
Babies who have a sensory processing disorder perceive sensations differently to others and become upset by situations and things that don’t trouble most other babies. They may find a particular smell, taste, or feel of certain foods or feel of the nipple of a feeding bottle and other objects in their mouth objectionable. Or they may be less aware or hypersensitive to the sensation of hunger.
Oral aversion is not the same as a feeding aversion.
A baby may be mistakenly diagnosed as having an oral aversion when in reality she has a feeding aversion. It’s important to make the distinction between oral and feeding aversion because the treatment for each is very different.
In the case of an oral aversion, a baby typically objects to anything in her mouth including the nipple of a feeding bottle. Whereas in the case of a feeding aversion, baby is happy to have things in her mouth just so long as it’s not the nipple of a bottle (or breast or spoon or food in the case of these types of feeding aversions).
A feeding aversion is often mistaken as an oral aversion. A feeding aversion is FAR more common than oral aversion. Therefore, it’s important that a feeding aversion is ruled out before assuming an oral aversion is the cause.
2. Baby is too tired to feed effectivelyA baby could become too tired to feed effectively or too exhausted to wake for night feeds for the following reasons.
- If her tired signs are overlooked.
- If she has learned to rely on sleep associations that cannot be maintained.
- If she is given sedative medications.
Overlooking or mistaking baby’s tiredness cues as hunger or boredom means baby might not get the opportunity to sleep when tired and is then at risk of becoming distressed due to overtiredness, which may then be mistakenly attributed to pain. (See Baby tired signs and How much sleep do babies need?)
Sleep association problemBabies often learn to rely on sleep associations (i. e., props and/or something the parent does) as a way to fall asleep. Learning to rely on sleep associations that cannot be maintained throughout baby’s entire sleep can result in broken sleep. Baby may wake prematurely from sleep still tired and cranky as a result of insufficient sleep. (See Sleep associations for more.)
e., props and/or something the parent does) as a way to fall asleep. Learning to rely on sleep associations that cannot be maintained throughout baby’s entire sleep can result in broken sleep. Baby may wake prematurely from sleep still tired and cranky as a result of insufficient sleep. (See Sleep associations for more.)
A baby could be too sleepy to feed due to receiving sedative medications prescribed to treat colic, such as antihistamines, antispasmodics, or others. (See Colic medications for more.)
3. Baby has poor appetiteThere’s nothing more effective than a hungry tummy to motivate a baby to want to eat. Without hunger a baby has little incentive to eat. The reasons a baby might have a poor appetite for milk feeds include:
- Illness
- Strict feeding schedules
- Solids
Any illness can negatively affect a baby’s appetite. Loss of appetite can be one of the earliest signs of illness before other symptoms become apparent. Weight loss can occur depending on the severity and longevity of the illness. However, once baby has recovered her appetite will return and she may then experience catch-up growth.
Weight loss can occur depending on the severity and longevity of the illness. However, once baby has recovered her appetite will return and she may then experience catch-up growth.
Typically, an ill baby will reject feeds in a passive manner compared to strongly oppositional refusal that occurs when a baby has developed an aversion to feeding.
Strict feeding schedulesWhile many babies thrive on a feeding schedule, not all do. Ignoring a baby’s hunger cues while trying to make her feed at predetermined times can result in underfeeding and poor growth.
You have probably experienced times when you felt pangs of hunger and may have been prevented from eating or chose to ignore these, perhaps because you were dieting. And then found the discomfort disappeared. This is because in the absence of food your body will convert glycogen stores and body fat into energy and so the desire to eat, though still present becomes less urgent. This would undoubtedly occur when babies are kept waiting too long for food when hungry.
Another problem with strict feeding schedules is that a ravenous baby can become distressed and disorganized, reject feeds or feed poorly. If she was also prevented from sleeping due to hunger this will add to her disorganized state.
SolidsMilk (breastmilk or infant formula) is the most important food for a baby during the first year of life. While solids are important to complement a baby’s diet, starting from 4 to 6 months of age, solids are a poor substitute for milk. Starting solids before the age of 4 months or giving solids at the wrong time in relation to milk feeds can result in a baby not drinking enough milk when offered. (See Starting solids for more.)
4. Baby is not able to access foodA baby could be physically capable of feeding, have a healthy appetite, and be willing to feed, but she could be prevented from feeding effectively because of the following reasons.
- Poor positioning
- Equipment problems
- Latch problems
Baby could be held in a position that makes it difficult for her to feed. For example, her neck could be twisted and her head is facing to the side, or her head could be flexed or extended in a way that makes it difficult for her to suck or swallow.
For example, her neck could be twisted and her head is facing to the side, or her head could be flexed or extended in a way that makes it difficult for her to suck or swallow.
A bottle-fed baby could experience difficulty feeding because of inappropriate or faulty feeding equipment. The hole at the end of the nipple might be blocked; or the nipple may be too short for her to get a proper seal and maintain suction; or the nipple could be too slow for her causing her to wear out before eating enough; or the nipple ring of a non-vented bottle may be screwed on too tightly slowing the flow rate or causing the nipple to collapse; or the venting system of a vented bottle or nipple might be faulty, also affecting flow rate.
Latch problemsA breastfed baby could have a problem latching to the breast. For example, her mother might have flat or inverted nipples, or her mother might not provide the support she needs to effectively latch. Or she may be held in a position that makes it difficult to latch or remain latched.
Or she may be held in a position that makes it difficult to latch or remain latched.
A tiny percentage of babies have physical impairments that affect their ability to suck. These fall into two categories.
- Structural problems
- Functional problems
A structural problem means baby has a physical abnormality affecting her ability to feed effectively, for example cleft palate, tongue-tie, or underdeveloped sucking pads (the fat pads in baby’s cheeks, which is usually only problematic for scrawny newborns).
Functional problemsEven though there may be no observable physical abnormality, baby might not be able to suck effectively due to a neurological impairment, an absence of sucking reflex, or due to nerve compression or damage occurring during birth.
Both structural and functional problems will be evident soon after baby’s birth. If your baby fed well and thrived after birth, you can probably rule out these problems.
If your baby fed well and thrived after birth, you can probably rule out these problems.
Not offering baby enough to eat is frequently believed to be the cause when a baby doesn’t gain as much weight as expected. While this is a common cause of poor growth in third world countries where food is scarce or expensive, it’s rarely the reason for babies in developed countries to underfeed or display poor growth. In general, parents in developed countries offer their babies as much milk as their baby is willing to take. The problem is that baby is not taking enough either because she’s not willing to or because she’s prevented from doing so.
Health professionals often advise parents to make sure their baby drinks a minimum specified amount at each feed. However, to make sure a baby drinks the recommended amount might involve some form of pressure. Repeatedly pressuring a baby to feed against her will is likely to cause her to develop a feeding aversion, which in turn will cause her to underfeed. So, what eventuates are repeated feeding battles that stress baby and parents.
So, what eventuates are repeated feeding battles that stress baby and parents.
If a baby is not eating enough, there is a reason. Pressuring or forcing a baby to feed or eat is NOT an effective solution. It’s likely to create greater problems.
MisdiagnosisThe two most common reasons that a baby might be assumed to be underfeeding are because:
- Baby is not drinking as much as expected.
- Baby is not gaining as much weight as expected.
In many cases where parents worry that their baby is not eating enough, there’s nothing wrong with baby’s milk intake or growth.
Baby is not drinking as much as expectedIf your baby displays visible signs that indicate she’s getting enough (described in the table above) then the problem might lie with your expectations or baby’s healthcare professional’s expectations about how much milk she needs.
There are numerous reasons why a baby might drink more or less than parents and health professionals expect. See How much milk does a baby need? for these.
Baby is not gaining as much weight as expectedIf your baby displays signs that indicate she’s well fed then it’s likely that what is perceived as poor growth is due to a false alarm, a variation of normal growth, or that the problem that caused her growth to falter has already been resolved.
Unrealistic expectations can occur as a result of mistakes made by health professionals when assessing a baby’s growth. (See Top 10 baby growth mistakes.)
How we can help- Your Baby's Bottle-feeding Aversion book
- Baby Care Advice consultation
- Rowena Bennett's Online Bottle-Feeding Aversion Program
In my book, ‘Your baby’s Bottle-feeding Aversion’, I have described physical and behavioral reasons for babies to develop an aversion to bottle-feeding. How to identify the cause and the solutions to match. Included are step-by-step instructions on how to regain your baby’s trust and resolve a feeding aversion caused or reinforced by repeated pressure to feed.
How to identify the cause and the solutions to match. Included are step-by-step instructions on how to regain your baby’s trust and resolve a feeding aversion caused or reinforced by repeated pressure to feed.
While the book was written for bottle-fed babies, many nursing mothers have found that applying the same strategies has also helped them to successfully resolve a breastfeeding aversion.
You might find that reading this book is all you need to do to understand the steps you need to take to resolve your baby’s feeding aversion and get him back to the point of enjoying eating until satisfied.
Baby Care Advice ConsultationIf you would like an individualized assessment of all reasons for infant feeding problems, not just feeding aversion, we also provide a consultation service. Baby Care Advice consultants have extensive experience in pinpointing the cause of feeding aversion and other behavioral feeding problems such as those related to equipment and the parent’s feeding practices. (For more on what’s included in a consultation).
(For more on what’s included in a consultation).
Six time-saving modules to help your family enjoy feeding again with Rowena's step-by-step plan. Enjoy additional tools to manage anxiety, troubleshoot any issues, introduce new carers, how to manage illness/teething and much more.
- Module 1: Understanding feeding aversions
- Module 2: Identify the cause
- Module 3: Prepare for success
- Module 4: How to resolve your baby's bottle-feeding aversion
- Module 5: What to expect
- Module 6: Troubleshooting
- BONUS: Guided meditations
By Rowena Bennett, RN, RM, CHN, MHN, IBCLC.
© Copyright www.babycareadvice.com 2021. All rights reserved.
 Permission from author must be obtained to reproduce all or any part of this article
Permission from author must be obtained to reproduce all or any part of this articleCauses, Emergency Care, and Treatments
“Poor feeding in infants” is a term used to describe an infant with little interest in feeding. It can also refer to an infant who is not feeding enough to receive the necessary nutrition required for adequate growth.
Poor growth associated with lack of feeding can lead to a separate condition called failure to thrive.
Poor feeding is caused by a variety of factors. It differs from picky eating, in which a baby may reject one form of milk for another or a toddler may refuse certain foods.
No matter the precise cause of poor feeding, undernutrition is a top concern. In fact, the World Health Organization (WHO) estimates that 45 percent of child deaths are related to undernutrition.
It is important not to dismiss poor feeding as something that will improve over time. This is a critical point in your child’s life, and missing key nutrients can lead to physical and cognitive concerns.
One of the most common causes of poor feeding is premature birth. Premature babies are typically poor feeders because they often have not yet developed the skills needed to suck and swallow milk.
Still, feeding usually increases as baby grows. If your little one was born prematurely and still has feeding trouble after leaving the hospital, it’s important to continue following up closely with your pediatrician, particularly if feeding concerns worsen or do not improve.
Other causes include congenital conditions such as jaundice and infections such as viral gastroenteritis. Once these conditions are treated, poor feeding usually subsides.
Serious conditions
Poor feeding can also be caused by serious conditions, such as Beckwith-Wiedemann syndrome. This is an overgrowth syndrome that causes infants to be particularly large and grow at a considerably fast pace. It affects an estimated 1 in 13,700 newborns worldwide.
Other serious conditions include:
- congenital hypothyroidism, which occurs when the thyroid fails to develop or function properly
- other genetic conditions, including Down syndrome
- hypoplastic left heart, a rare condition that occurs when the left side of the heart fails to develop properly and is unable to pump blood to the body
- other heart defects
Less serious conditions
Other causes of poor feeding aren’t related to a congenital condition at all.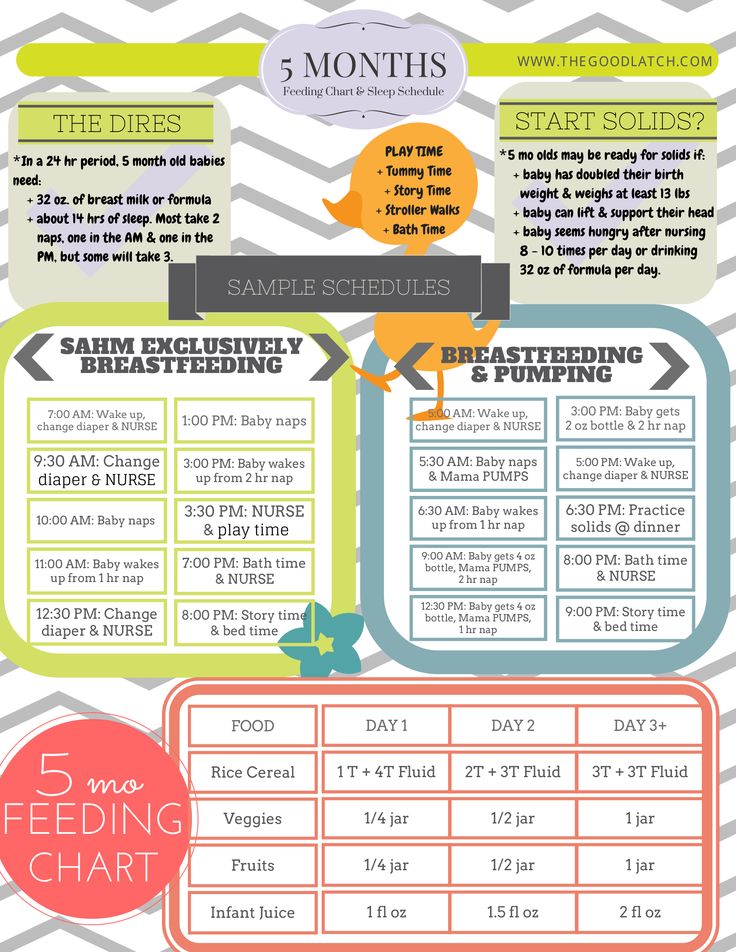 Temporary illnesses can make feeding uncomfortable (and even painful) for infants.
Temporary illnesses can make feeding uncomfortable (and even painful) for infants.
Common ailments that get in the way of feeding include:
- diarrhea
- ear infections
- coughs and colds
- teething
When in doubt, it’s always best to double-check with a pediatrician. You don’t want to assume a minor illness when in fact there could be a serious underlying condition.
Feeding difficulty is a serious matter. When accompanied by other symptoms, emergency care may be required. Seek immediate medical attention if your baby is showing any of the following signs:
- has a fever of over 100°F (37.8°C), an emergency in babies 3 months old and younger
- is vomiting after every feeding
- is vomiting blood
- has a cough with breathing difficulties
- is crying constantly
- has bloody stool
- is wheezing
- is becoming unresponsive to touch
Poor feeding that is caused by an infection will usually stop when the infection is resolved.
Treatment of poor feeding depends on the cause. This can involve changing the feeding schedule to consist of smaller, more frequent meals. If a milk-based intolerance is suspected, your doctor will work closely with you to find a formula and feeding plan that suits your baby.
While serious cases of poor feeding require prompt medical care, other causes can be resolved at home with the advice of a pediatrician.
If your baby is breastfeeding or chestfeeding, try to avoid:
- certain medications that can enter breast milk
- applying lotions and other skin products to your breasts
- high levels of stress — this may also make your milk taste differently
Other considerations may concern formula feeding as well as infants who have started solid foods.
Formula feeding
While breastfeeding is the method of feeding for infants recommended by health agencies such as WHO, it is a fact that not all babies are successful with this method — and not all nursing parents may want or be able to breastfeed.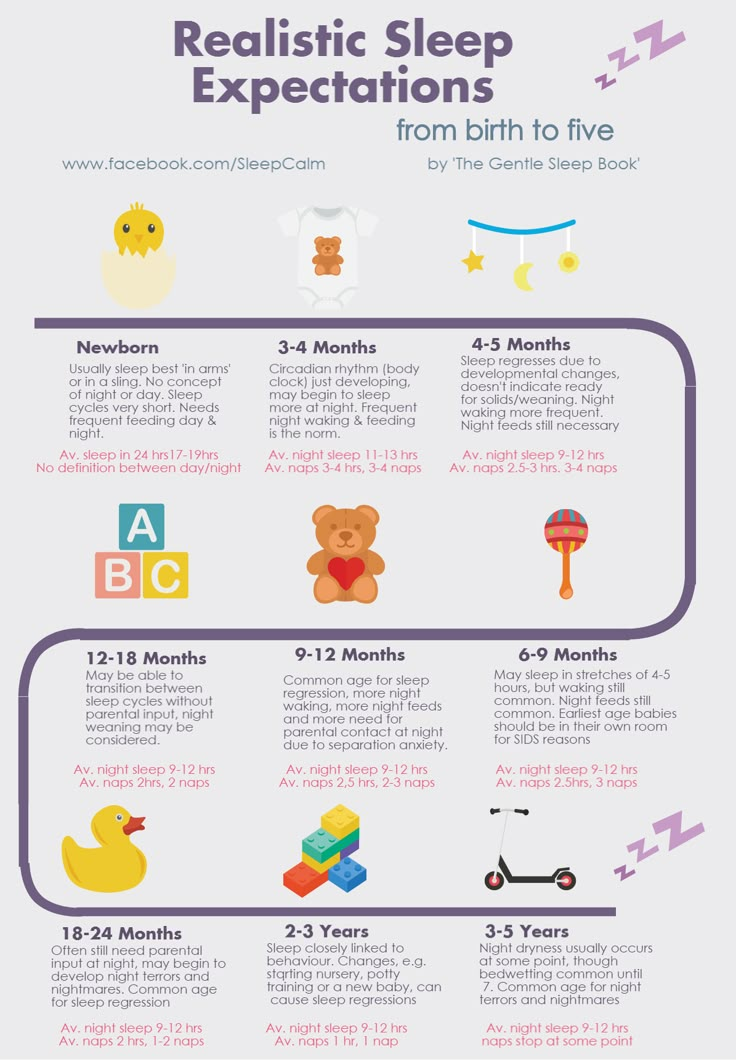
If your baby doesn’t seem to latch on despite repeated attempts, you may consider talking with your doctor about formula feeding. You may still be able to try breastfeeding or chestfeeding, even when supplementing with formula, if you’d like.
The key is that your baby gets adequate nutrition. A lactation consultant may be helpful, if available to you.
“Picky eating”
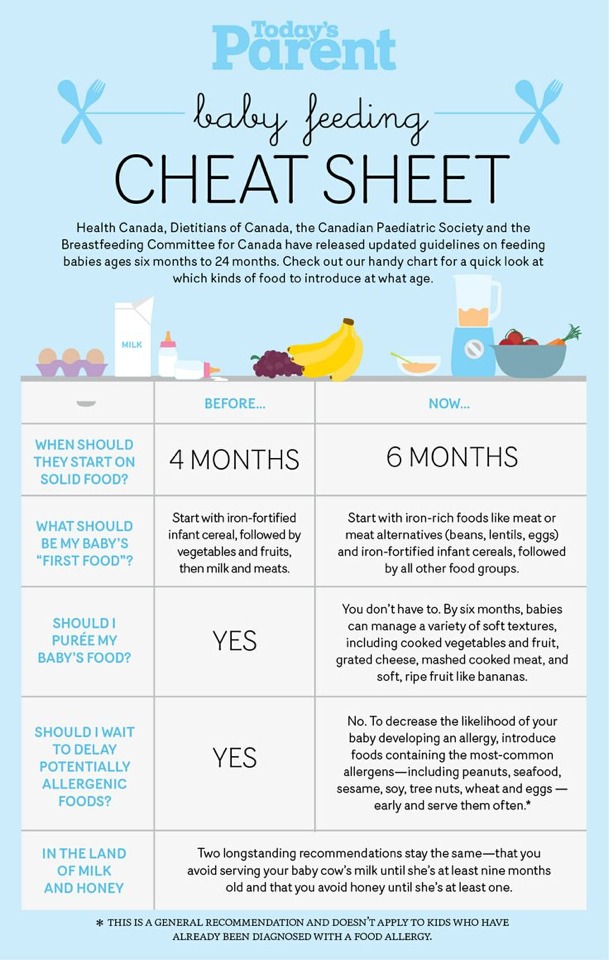
After baby reaches 6 months of age, your pediatrician may encourage you to introduce solids to their diet. While solids shouldn’t replace breast milk at this phase of your child’s life, most infants require additional nutrients around the 6-month mark.
Examples include:
- rice cereal
- pureed fruits and vegetables
- pureed or soft meats
Introducing solid foods can be exciting for both caregiver and child. However, some infants don’t take to solids as readily as other babies.
This can be alarming, but the issue may be solved by:
- mixing cereal with solid foods
- offering solids in small increments
- only giving solids two to three times per day
- starting with one food at a time, then introducing others as your baby gets used to solids
When an infant doesn’t like solids, it’s easy to jump to the conclusion that they are a “picky eater.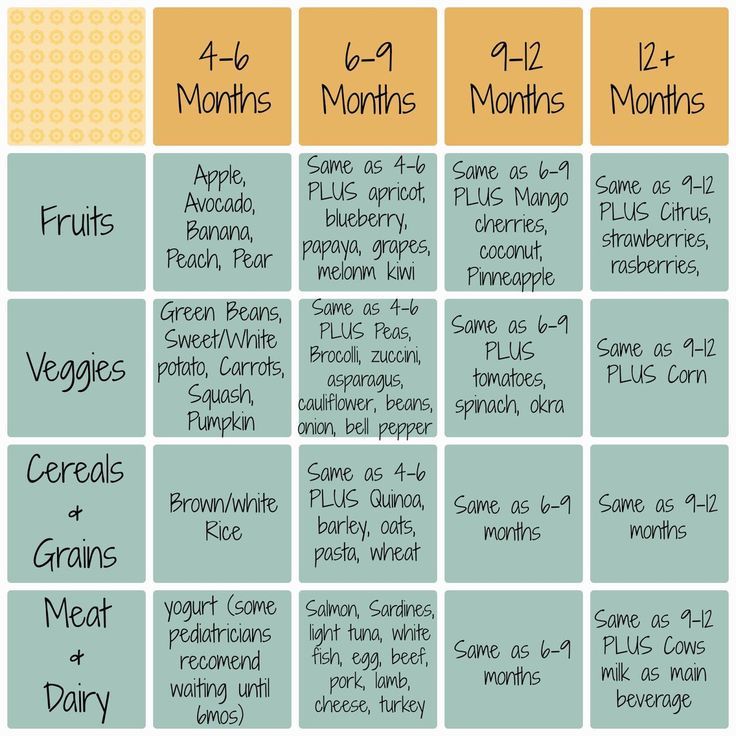 ” However, this phase doesn’t usually start until your baby becomes a toddler.
” However, this phase doesn’t usually start until your baby becomes a toddler.
Stress management
When your baby is eating poorly, it’s easy to get stressed out. This is especially true for new parents who may not yet know the distinctions between serious conditions and minor feeding concerns.
Remember that stress can worsen feeding concerns. It may interfere with attempts at feeding if your infant senses something is wrong.
Managing your stress won’t treat all causes of poor feeding, but it can help in many cases.
It’s difficult to find time for yourself during this busy stage of your life — even a few minutes a day can help. When you feel stress coming on during feedings, take a moment for some deep breathing.
Poor feeding in infants can lead to serious issues, such as malnutrition and stunted growth. It is essential that babies consume and digest the necessary nutrients to thrive and develop.
Any infant who is feeding poorly should be taken to a pediatrician for evaluation.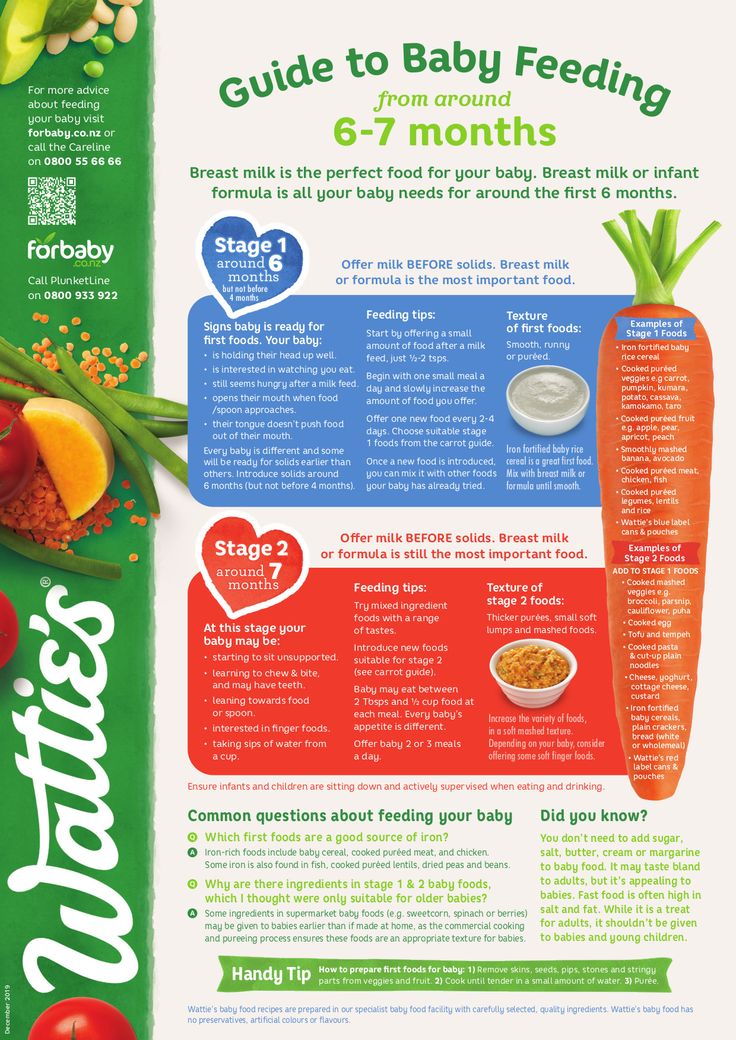 After a proper diagnosis, treatment may be necessary.
After a proper diagnosis, treatment may be necessary.
In other cases, poor feeding can be resolved through refined techniques and perseverance at home. If you suspect feeding difficulties may be causing other concerns, call a doctor right away.
If the child does not eat well: what to do and what not to do
What to do if the child does not want to eat.
- Malyusik, well, one more spoon - and that's it! Last! I ate only two, let's have a little more, here's the most delicious piece for you! - says the average mother, offering a spoon with one hand, playing the accordion with the other, showing the trick with the disappearance of the handkerchief with the third, turning the cutlets over with the fourth, while doing somersaults on one leg.
Sound familiar?
Every dad has an instinct to bring home food, and mom has to feed the baby food. And if he refuses to eat, a signal is triggered - "I'm a bad mother" or "the child is sick."
In this case, the most important thing for a parent to understand is whether the child DOES NOT WANT or CANNOT eat?
If the baby is running around, having fun and looking good, without showing any signs of illness, then most likely he does not want to eat. There can be many reasons:
There can be many reasons:
- A breastfeeding child prefers milk and dairy products, intuitively understanding that he needs calcium, and now milk is healthier for him than soup.
- The child wants a cookie, not vegetables.
- He really wasn't hungry. For example, his metabolism is slow, breakfast has not yet been digested, and lunch is already being offered. Or the child was sitting in front of the TV after breakfast and his appetite had not yet had enough time to play out. Compared to the boy next door who was outside all day.
- If a child is not genetically destined to become Uncle Styopa, then he can eat much less than his peer, who has tall parents.
- Psychological problems. If earlier you accidentally gave your child a bitter cucumber, then he may refuse any green food. Or you yell at the child during the meal, and for him the food is perceived as a trauma.
If your child is lively, but at the same time he has a "bad appetite", then this is not his problem, but yours - the psychological problem of an unsatisfied instinct.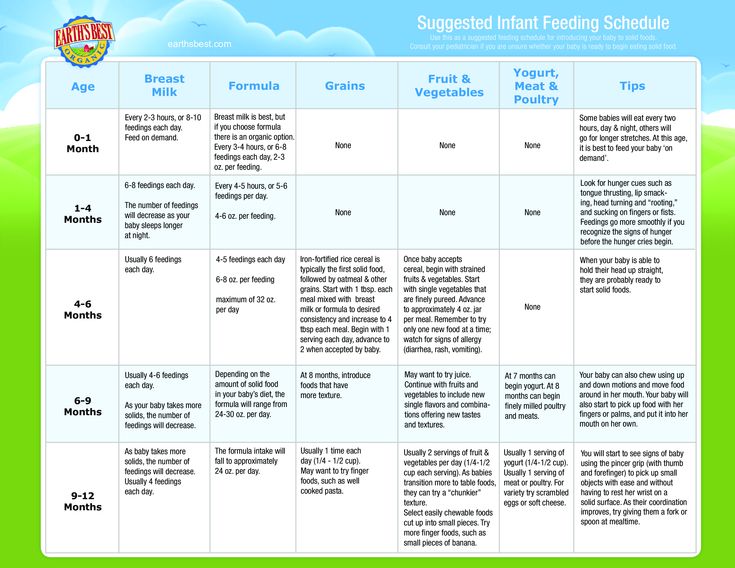 If a child jumps, jumps, he has healthy nails, hair, etc., think less about what he lacks. Better think about something nice))
If a child jumps, jumps, he has healthy nails, hair, etc., think less about what he lacks. Better think about something nice))
An active child = not a hungry child.
Wait for the natural desire and correctly distribute energy costs - walk more often, send the child to the sports section, or simply say: “If you don’t want to, take a walk, dinner is not earlier than seven and no snacks.” That is, if your child simply does not want to eat, normalize feeding - strictly at a certain time and without snacks. The body will get used to secrete gastric juice strictly according to the schedule.
And one more thing. There are no rules about how much a child should eat. He can eat a kilo (and make you very happy) and 9Send 00 grams to the toilet. Or eat 100 g and learn everything.
But it is much more difficult if the child CANNOT eat.
Causes:
- If you are breastfeeding, you may have “tight breasts”, when it is very difficult for the baby to suck milk.
- The child has a runny nose, and when he eats, he begins to choke.
- Food hot, cold, sour, bitter.
- He has sores in his mouth (for example, from toys), and they hurt when food gets on them.
- Teeth are cut, gums hurt.
- Bowel problems. The stomach starts to hurt while eating.
- The child simply fell ill (cold, SARS, poisoning, influenza, etc.). If the child is sick, and he is not dystrophic, then you should not force him to eat. The body fights infections better when it's hungry. But be sure to drink.
If a child at first shows appetite and interest in food, but refuses to eat through a spoon or two, then, most likely, the process of eating causes him certain difficulties.
If the baby CANNOT eat and you can't identify or eliminate the cause, the best thing to do is contact your pediatrician. The doctor will accurately determine the problem and give the necessary recommendations.
Our clinic has a wonderful pediatrician Yuliya Vladimirovna Sinyagina with 17 years of experience! You can sign up to her))
Bon appetit everyone! As well as strength, patience and satisfied instincts!
Back to the list of articles
What to do if the child does not eat well.

Child needs to eat instinctively from birth . If the child is healthy, he eats as much as his body requires. Over the years, our instincts weaken and eating behavior begins to rely not only on the needs of the body, but also on:
- socio-psychological environment
- experience
- emotional state
It is very important to be able to distinguish between a true decrease in appetite and a false one. If false, there are no problems with food or health, but at the same time, parents are unhappy with the amount of food eaten.
To diagnose a child's eating behavior, it is necessary, first of all, to clarify the general state of the child's health, his activity, growth and weight indicators and their dynamics, and especially the rhythm of nutrition.
Types of refusal to eat:
- A child older than 1.5–2 years does not eat certain food groups. For example, refuses vegetables, meat or cereals.
- The child bites and eats mainly junk food: sweets, fast food and processed meat (sausages, sausages).
- A child older than one and a half years old eats only liquid, homogeneous food (for example, milk, formula or puree).
- The child refuses any food and goes on hunger strikes
- The child experiences fear when eating due to some trouble that occurred while eating.
- For diseases of the oral cavity and disorders of the digestive system. The child avoids pain when eating or after eating.
- The child may not eat well when he is not feeling well. This is a normal human reaction to the disease.
- Increased nervous excitability. An excited child can hardly secrete the required amount of saliva, so it is difficult for him to have dryish food. If you are under a lot of stress, you may have trouble swallowing due to throat spasms.
Consequences of refusal to eat:
- the child does not gain weight for a long time, growth and lags behind in physical development
- chronic eating disorder, deficiency of vitamins and microelements layer is very thin.
 There is a decrease in immunity, a tendency to frequent infections and their protracted course; fatigue and general weakness.
There is a decrease in immunity, a tendency to frequent infections and their protracted course; fatigue and general weakness. If diseases are ruled out, in most cases the problem of the child's selective appetite can be solved by parents on their own.
What to do?
Lots of recommendations. To normalize the appetite will have to spend a lot of time and effort. Therefore, be patient.
- There is one simple rule that helps to determine the amount of food a child needs: the number of spoons of each meal eaten must be at least the number of full years . You can conclude a kind of contract to comply with this rule. If the child understands the agreements, he can correctly calculate his strength and build expectations . Large plates can scare a child, as can huge portions.
- Think about how a child usually eats. If it is filled with persuasion, quarrels, threats of punishment, then a decrease in appetite is quite natural.
 Our psyche is arranged in such a way that the emotional coloring of events occurring simultaneously is mixed and attached to each other . If food becomes a cause of conflict with parents, the child experiences unpleasant emotions - resentment, shame, anger, etc. These emotions are superimposed on all meals. Try not to force him to finish his plate, do not threaten punishment. The more you force, the more the child will resist. Make your meal a pleasant event of the day in a warm family circle with a beautiful table setting.
Our psyche is arranged in such a way that the emotional coloring of events occurring simultaneously is mixed and attached to each other . If food becomes a cause of conflict with parents, the child experiences unpleasant emotions - resentment, shame, anger, etc. These emotions are superimposed on all meals. Try not to force him to finish his plate, do not threaten punishment. The more you force, the more the child will resist. Make your meal a pleasant event of the day in a warm family circle with a beautiful table setting. - However, the opposite situation also happens: the mother, on the contrary, does not offer food too persistently. There is an opinion: you need to make 8 to 15 unobtrusive attempts, preferably in a playful way, so that the child gets used to unfamiliar food. Use little tricks. Offer new foods to your child to choose from - for example, from 2-3 dishes. This will help him understand that his opinion is taken into account in the family.
 Replace products. Try different types of meat - the child will surely choose something for himself, because he needs iron in an easily digestible form, which can only be obtained from meat products. Add mince to vegetables. Use different cooking methods.
Replace products. Try different types of meat - the child will surely choose something for himself, because he needs iron in an easily digestible form, which can only be obtained from meat products. Add mince to vegetables. Use different cooking methods. - Selective appetite develops in children of parents who use food as a reward or as blackmail: "If you don't eat soup, you won't go for a walk." Pediatricians emphasize that food is a source of nutrients, fuel for the body, and not a means of manipulation.
- You should not feed a child mechanically when he is engrossed, say, in playing or watching a movie - many children eat well under advertising or on a tablet, not feeling the taste of food at all, which ultimately only reduces their appetite.
- Children are much more willing to eat what has been cooked with them, so feel free to involve them in the cooking process. Turn cooking into an exciting joint creativity, and you will see how the child gradually changes his attitude to food.