Why does my baby leaks milk when bottle feeding
Correctly bottle feeding your baby
Before becoming a NICU nurse, I didn’t even know there were different “ways” to hold your baby while feeding. I had only ever seen – and done – the “crook of the arm” feeding. This is the way babies, in my mind, were always fed!
Well, the NICU quickly changed that!
Did you know that the instinct to feed is not generally seen in babies less than 36 weeks gestation? This means that babies born before 36 weeks (also known as late preterm) may not show signs that they are ready to take a feeding by mouth (bottle or breast).
For this reason, it’s not uncommon to see premature + late preterm babies with a nasogastric (NG) tube. This tube allows baby to be fed breastmilk or formula straight into their tummy without the actual act of eating.
As babies approach their due date and become “term” (36-37 weeks+, sometimes a bit earlier), we test their readiness to feed by bottle.
We give them little tastes of milk on a pacifier to help them learn how to suck, swallow, and breathe correctly (we even give preemies a swab of breastmilk very early on to get them familiar with the taste!).
But giving tastes does more than just familiarize them with the taste and smell of milk – it actually tells us A LOT of information!
We can gather baby’s interest in feeding, neurological readiness (sleepy preemies can’t take a bottle!), and read their cues. Have they developed a negative association with oral stimulus (paci, bottle) from having a breathing tube for so long?
Is their reflux so painful that they associate feedings with pain? Are they overwhelmed while feeding (sleepy at the bottle, breathing fast, dropping their heart rate low, sticking their tongue out and pushing the bottle out?)
Suck, swallow, breathe is a coordination skill that some babies need a little help in mastering.
I say this all the time to my clients, but LOOK at your baby and LISTEN to cues as you feed! We can gather SO MUCH information by looking at our baby feed – including signs of hunger, satiety, oral aversion, reflux, etc.
We understand that bottle feeding can be challenging! We are here to help you! Click here to learn more about the supportive services we offer!
My baby isn’t a preemie. Do I still need to watch them closely while they feed?
Do I still need to watch them closely while they feed?
Yes! Bottle feeding should still be to your term baby’s cues. Feeding and taking a bottle is a skill that baby needs to learn how to do.
And bottle feeding positioning is important for many reasons which we will get into below.
Why is it so important to know your baby’s feeding cues while bottle feeding?
It tells us a lot about how baby is feeling during a feed:
- It tells us if baby needs to slow down the pace (size down on a nipple) or speed up the pace (upsize the nipple). See below.
- It tells us if baby is full. We often try to feed all the contents of the bottle – but baby may not want all the contents. It’s MORE important for baby to control the amount they take in and have a positive experience, than accidentally force feeding.
- It tells us if baby is still hungry BUT prevents overfeeding. If a bottle is completely finished, and baby is rooting or sucking, they may want more.
 We will talk about side lying feeding in a bit, but basically by following baby’s cues with side lying, baby is controlling the pace of the bottle.
We will talk about side lying feeding in a bit, but basically by following baby’s cues with side lying, baby is controlling the pace of the bottle. - So if baby does want more, it is available to take at their pace, rather then dripping out of the bottle due to gravity. Signs of being done with the bottle include yawning, sneezing, pushing out of the tongue, pushing the bottle out with the tongue, arching back away from the bottle, gazing up and away from the bottle.
- It tells us if baby is overwhelmed. Persistent hiccuping, sneezing, yawning, gagging, or pushing out of the tongue all are signs of being “done” or overwhelmed with the bottle.
- It prevents oral aversion. You wouldn’t like it either if someone was forcefully sticking food in your mouth! Repetitive accidental force feeding creates an oral aversion, refusal of the bottle, fussiness, and refusal to eat by bottle.
- Try allowing baby to open BEFORE you place the bottle in baby’s mouth by gently tickling their upper lip with the bottle.
 Once baby opens, they are ready to latch and feed.
Once baby opens, they are ready to latch and feed.
But who CARES?! My baby hasn’t shown any of these things and feeds just fine the way I feed her.
YOU are the parent! You have every right to make the decision for your baby! I am here to inform and help you prevent or reverse some possible negative symptoms of gravity-lead bottle feeding positioning.
Does it matter if the contents are formula or breastmilk?
No! Anytime you are bottle feeding, no matter the contents, side-lying is the way to go.
Correctly bottle feeding
SO – What do I DO?
SIDE LYING POSITIONING + INCLINED!
What the heck is side lying + inclined positioning?
Side lying positioning is when baby is laying on their side (ear, shoulder, and hip should all be aligned). Then, incline their head slightly with your hand or a pillow (I even just cross my legs!).
Why is side lying + inclined feeding important?
Side lying + inclined feeding mimics breastfeeding – both in position and flow. It allows baby to control the flow of the bottle, leading to a positive experience with the bottle, less choking and coughing, less flooding, and LESS EAR INFECTIONS!
It allows baby to control the flow of the bottle, leading to a positive experience with the bottle, less choking and coughing, less flooding, and LESS EAR INFECTIONS!
A bottle has an opening at the nipple. This opening is consistently open, whether baby is sucking or not. Test by holding a bottle upside down – it drips!
This dripping also happens in baby’s mouth when we hold the bottle in a downward position where gravity is pulling the milk out of the bottle, not baby, such as in the “crook of the arm” feeding position.
When gravity pulls out the milk (aka dripping of the bottle), baby is actually getting more milk flow than they are sucking out. This causes baby to get flooded – meaning there is too much milk in baby’s mouth.
This makes it hard to baby to keep up with the amount of milk in their mouth – leading to gulping, choking, coughing, milk dripping out of the side of their mouth.
This can happen with a “crook of the arm” positioning because the nipple is angling down, allowing gravity to do the work.
Think about if you were trying to drink something using a straw. Then, someone was simultaneously pushing more liquid in your mouth.
It would be really hard for us to keep up! If this was consistently happening, we would pretty soon say, “I’m not drinking out a straw anymore!”
This same thing happens to baby – they simply can’t keep up and may start to associate the feeds negatively.
How do I feed baby in side lying position?
- Bend your knees and elevate your legs on a coffee table or ottoman. If you don’t have those available, cross your legs or place a pillow on your lap.
- Place baby in side lying position on your lap with their head closest to your knees.
- Support baby’s head and neck with your non-dominant hand.
- Hold the bottle parallel to the floor.
- Feed baby.
Tip: Watch my reels on how to correctly bottle feed your baby and how to burp your baby!
Ear infections + how they related to feeding positionEar infections are also called otitis media. They are very common, especially in infants. Side note – ear infections are NOT contagious.
They are very common, especially in infants. Side note – ear infections are NOT contagious.
The eustachian tube in the ear connects the middle ear with the back of the throat. If formula or breastmilk continually is entering the eustachian tubes, this causes bacteria from the mouth (naturally occuring bacteria) to enter the middle ear, causing ear infections.
Bacteria feed on the nutrients in breastmilk and formula, making easy for them to multiply, causing and infection.
“Crook of the arm” is gravity lead, which leads to flooding, making the risk of formula or breastmilk entering the eustachian tubes much higher (and therefore the middle ear), which in turn increases the risk for ear infections.
Side lying feeding is baby lead, meaning baby is pulling the amount they can handle from the bottle. This prevents flooding, and therefore, the risk of ear infections is much lower.
I heard that breastfeeding lowers the chance of ear infections. Is that true?
To an extent. Breastmilk does contain antibodies that can help prevent infections, including ear infections. However, bottle-fed breastmilk poses basically the same risk as formula since the positioning is actually what causes the ear infections.
Breastmilk does contain antibodies that can help prevent infections, including ear infections. However, bottle-fed breastmilk poses basically the same risk as formula since the positioning is actually what causes the ear infections.
Breastfeeding from the breast does help reduce the risk for ear infections due to proper positioning and flow, however, it does not eliminate the risk.
I see air in the nipple. Should I be concerned?
No. Air at the top of the nipple is normal – the milk still fills the tip of the nipple so baby won’t suck in air.
My baby is gulping and chokes on the bottle. What can I do?
Your baby may need a smaller size nipple. If you’re already using the smallest size, try paced feedings. Paced feedings allow baby to “catch up” and swallow the milk in their mouth, then breathe, then suck.
Too much milk will cause them to gulp, not be able to take a breath, etc. Click here for a demonstration.
My baby gets frustrated at the bottle and when I take the bottle out, the nipple is completely flat and collapsed.
Time to move up to the next size nipple! Baby is sucking harder than the nipple flow allows.
It takes FOREVER for my baby to feed from the bottle, more than 45 minutes. What can I do?
Try upsizing the nipple! If baby is dripping, gagging or choking, the flow is too fast and move down a nipple size. Or try paced feedings with the larger nipple.
My breastfed baby WILL NOT take a bottle. HELP!
Your wish is my command! We offer 1:1 virtual consults from the comfort of your own home to introduce the bottle to your breastfed baby in a way that promotes a positive association with the bottle.
We also offer in home bottle feeding consultations for the Chicagoland area!
Click here to view the consultations we offer!
Watch our workshop! Watch our recorded workshop, “Bottle Refusal and Tips.” Join Lauren, NICU RN and mother of 2, discuss tips for bottle refusal in infants. She discusses different strategies for avoiding bottle refusal along with tips and tricks for reversing bottle aversions. She also goes over alternative methods for giving breast milk/formula to babies who have ongoing issues with bottle refusal.
She also goes over alternative methods for giving breast milk/formula to babies who have ongoing issues with bottle refusal.
WATCH BOTTLE WORKSHOP NOW
Have more questions? Schedule a text or video chat consult with Kate, Lauren or Natalie (NICU RNs) and they can help answer any questions that you have!
BOOK CONSULT NOW
PRO TIP: I highly recommend these Lansinoh bottles (I use them all the time in consultations). I also really like these Evenflo bottles for newborns too!
Other helpful blog posts:
- How to supplement with formula
- Everything you need to know about acid reflux
- Transitioning from formula to milk
- Everything you need to know about formula
- Diaper bag essentials
- How to travel with kids
**This post is educational and not meant to take the place of your provider. Bumblebaby makes a small commission on some of the items listed above
Bumblebaby makes a small commission on some of the items listed above
Baby Always Dribbles Milk (Nursing, Bottle Feeding, or Both)
Babies are constantly learning and growing in every aspect of their lives – including in basic skills such as eating. While most babies can drink milk or formula immediately after birth, some little ones seem to always lose their milk out the side of their mouth as they’re eating.
Although your baby’s leaking milk can be caused by conditions such as tongue-tie or problems with the nipple size or assembly that you’re using, some babies who dribble milk are simply messy eaters. If your little one seems to be getting enough food (he’s growing well and peeing on schedule), then his milk dribbles shouldn’t be a concern.
If your baby seems constantly hungry and still dribbles most of his meal while eating, there may be a problem. Keep reading to learn about the most common reasons for babies to dribble milk, and for tips on how to help.
Table of Contents
Baby always dribbles milk when feeding
It can be a real pain if your baby leaks their meals all over the place. Not only are you worried that your precious little one might not be getting enough to eat, but you’re having to manage the piles of milk-soaked laundry. And if your child has been dribbling milk for weeks, you may even begin to worry that there might be something wrong.
While some babies are just messy eaters, there can also be underlying issues at play causing milk dribbling. Tongue-tie is one such problem and results in restricted tongue mobility that can make it hard for a baby to form a proper latch on the breast or bottle. Another common problem is the speed at which babies are given milk.
In breastfed babies, mothers with an oversupply of milk may be producing more than their baby can swallow at any given time. In bottle-fed babies, a large nipple size might be flooding the baby’s mouth with too much milk.
If your baby constantly dribbles large amounts of milk when feeding (whether they’re breast- or bottle-fed), you may want to consult with their pediatrician or a lactation consultant to see if your child might have a tongue-tie. If their mouth anatomy seems normal, then it might be worth switching up feeding methods by trying new nursing positions or switching nipples if bottle feeding.
Is baby getting enough milk
One of the biggest worries with milk-dribbling babies is that they might not be swallowing enough food. It can be particularly difficult to tell how much milk your little one is drinking if you’re breastfeeding.
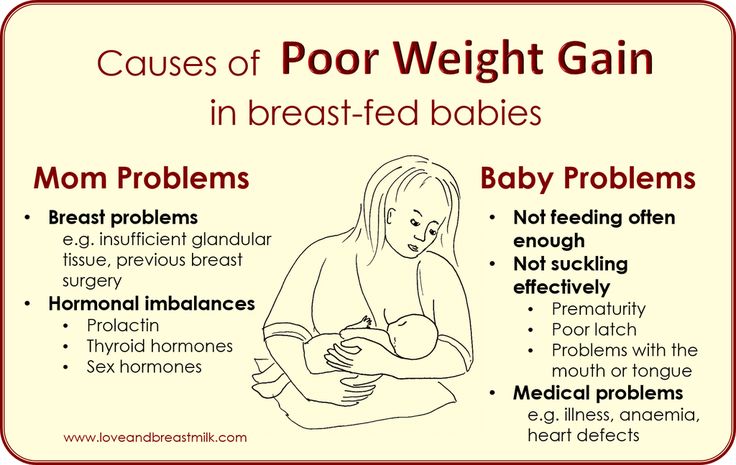
Generally, if your baby seems content after eating and is gaining weight as predicted, they’re eating enough. In contrast, if your baby seems extra sleepy and isn’t gaining weight as expected, they might not be getting enough milk.
Signs that baby is getting enough milk
If your baby appears to be growing and developing fine, then it’s likely not a problem if she’s also dribbling milk.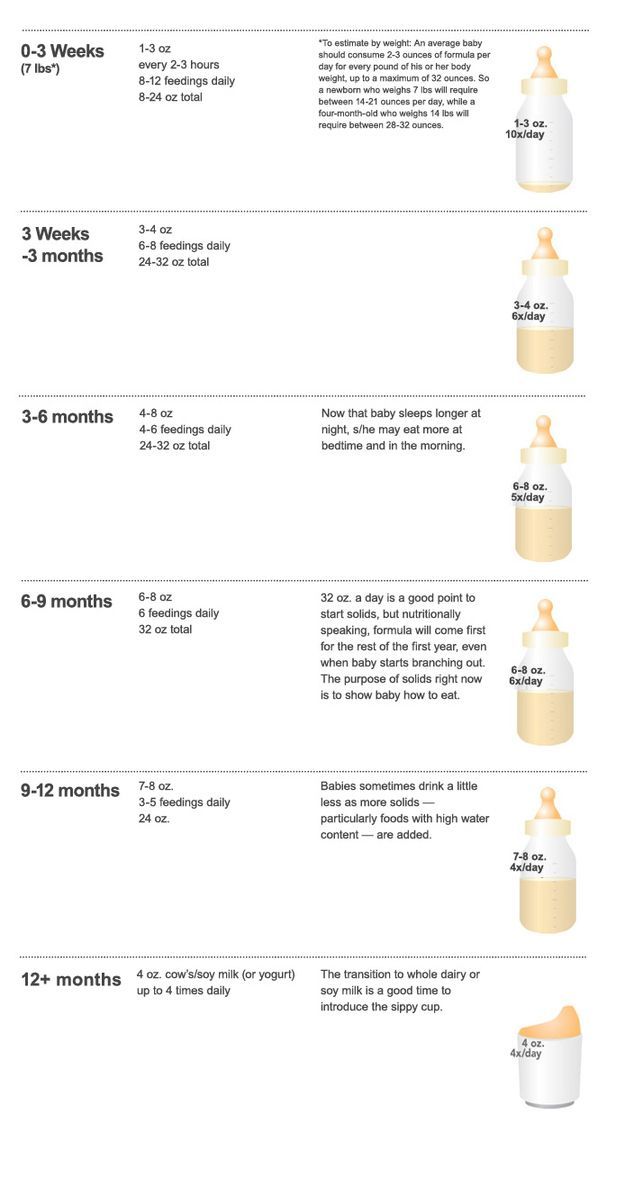
If your baby is getting enough milk, she may:
- Nurse or eat frequently and on a consistent schedule
- Seem content and happy after eating
- Gain approximately 5.5-8.5 ounces of weight per week until 4 months of age
- Clearly swallow while breastfeeding, or empty a bottle
- Fill diapers with light-colored urine on a consistent schedule
- Appear alert and active, and meet developmental milestones
While it can be frustrating to lose so much breastmilk or formula (not to mention deal with the additional laundry), it should be comforting to know that your little one is still happy and healthy.
Signs that baby isn’t getting enough milk
If your baby isn’t swallowing enough milk, she may:
- Seem extra sleepy or even lethargic
- Sleep more than 4 hours at a time
- Take a very brief or very long time nursing or working at a bottle
- Consistently fall asleep while feeding
- Have a shallow or painful latch while nursing
- Gain less weight than expected (5.
 5-8.5 ounces per week is normal)
5-8.5 ounces per week is normal) - Have dark urine or dry diapers
If your child doesn’t seem to be getting enough milk, it’s important to consult with a pediatrician or lactation consultant right away. If you’re ever concerned about your baby, trust your instincts and seek medical care.
Breastfed baby dribbles milk when nursing
When breastfed babies dribble milk while nursing, there are two main culprits: tongue-tie and oversupply.
Tongue-tie affects your baby, essentially restricting the mobility of their tongue so that it’s hard for them to get a good latch on the breast (hence, the leaking milk).
Oversupply occurs in the mother when she produces more milk than her baby needs, leading to her baby spluttering, gasping, and dribbling milk.
Tongue-tie
Tongue-tie, or ankyloglossia, occurs when the lingual frenulum (the part of the mouth that anchors the tongue to the mouth floor) is extra tight or short.
Though it may not seem like a big deal, a tongue-tie can restrict tongue mobility and be of particular concern in babies. Breastfeeding requires careful coordination of a baby’s mouth muscles in order to latch, suck, and swallow effectively, and tongue-tie can hamper that motion, leading to difficulty latching and/or swallowing quick-flowing breast milk.
A baby with a tongue-tie will likely dribble milk while attempting to feed, an occurrence that can be uncomfortable for both baby and mother. While it is possible for babies with tongue-tie to breastfeed, they may experience more difficulty with the process than they might otherwise.
Oversupply
‘Oversupply’ refers to an overabundance of breast milk produced by a mother – much more milk than her baby needs.
Too much of a good thing can be a bad thing, and having extra breast milk doesn’t actually mean a better-fed baby. Instead, the flow of breast milk can be hard for the little one to process. It can be a bit like drinking from a firehose for the baby, and can lead to difficulties with nursing.
It can be a bit like drinking from a firehose for the baby, and can lead to difficulties with nursing.
Some signs of oversupply include:
- Baby may cough, choke, or splutter while nursing
- Baby may be restless during feeding
- Feedings may be short and frequent
- Mother might have a strong, forceful milk release
- Mother’s breasts might always feel full, or refill quickly after a feeding
- Frequent plugged ducts or mastitis
- Baby may ‘dribble’ milk while eating
Baby always dribbles milk from a bottle
Babies can dribble milk from bottles just as they do while nursing, and the culprits are often similar: tongue-tie and extra milk flow.
Tongue-tie
Tongue-tie, or ankyloglossia, occurs when the lingual frenulum (the membrane that secures the tongue to the bottom of the mouth) is too tight or short.
Tongue-tie can restrict tongue mobility, which can make it difficult for a baby to master the complex action of drinking from a bottle. A baby with tongue-tie may dribble milk while feeding.
Milk flow is too fast/strong
While bottles can be a convenient way for babies to eat, they can sometimes be too convenient. Babies can only swallow so much milk or formula at a time, and if the flow out of their bottle is too fast or strong, it can cause problems.
Each bottle brand has a different speed of milk flow, which can make it tricky to tell exactly how much milk is entering your baby’s mouth per second. And each baby has a different limit for what constitutes a ‘comfortable’ speed.
Nipple too big
One way to control the milk flow in a bottle is through the nipple size.
Different brands have different variations in size, but most begin with a ‘preemie’ or ‘newborn’ level and go on up from there. There are often guidelines for when to use which size nipple, but the ranges can vary, and each child is different. A too-big nipple on a bottle can lead to a strong flow of milk that might be too hard for your baby to keep up with.
A too-big nipple on a bottle can lead to a strong flow of milk that might be too hard for your baby to keep up with.
When your baby can’t swallow all the milk that enters their mouth, the excess will dribble out the side.
Anti-colic nipple incorrectly assembled
Anti-colic nipples can work wonders by minimizing the amount of air a baby swallows while drinking, helping to reduce gassy bellies. The catch?
In order to keep the bottles and nipples clean, they come apart. And if they aren’t reassembled correctly, then milk or formula can leak all over the place.
Some of the most popular anti-colic nipples are manufactured by:
- Phillips Avent
- Dr. Brown
- Comotomo
- NUK
- Playtex
- MAM
How to keep baby from dribbling milk
While some babies are just messy eaters, you don’t have to resign yourself to endless cycles of laundry just yet.
If your baby has a tongue- or lip-tie, look into correcting it. If you’re bottle-feeding, try a different nipple size or shape, check the bottle assembly, or switch up the position you use to feed your baby.
Tongue and lip tie correction
If your baby has been diagnosed with tongue- or lip-tie (thickened mouth membranes that restrict movement) you can look into a surgical correction.
While surgery isn’t often necessary, it can help improve breastfeeding, especially in cases where the baby isn’t gaining weight properly. Surgical correction can also prevent dental or speech problems later in life.
Try a different nipple size
Smaller bottle nipples can help reduce dribbled milk by limiting the amount of milk flowing into a baby’s mouth at one time.
A too-large bottle nipple is one of the most common causes of dribbled milk, so this is one of the best solutions to test out first.
Try a different nipple shape
Some brands have differently shaped nipples that might work better for your messy eater.
Babies need to latch onto bottle nipples just like they do while breastfeeding, and mixing up the shape of the nipple can lead to a better latch (and fewer spills!)
Ensure anti-colic nipple correctly assembled
Yes, putting back anti-colic nipples can be complicated, but it’s important to double-check that they’re assembled properly.
The seals in the nipple should be air (and liquid) tight, otherwise, you’ll have unwanted spills.
Bottle feed baby sitting up
Drinking while lying down is just plain hard, even for babies.
If your baby is dribbling milk, try feeding them a bottle while they’re sitting up. Keeping a baby upright during feedings can also reduce gas and colic in addition to minimizing milk dribbles.
Artificial feeding of babies | Bebbo
Submitted by Ilya Danshyn on Wed, 12/08/2021 - 18:40
Sometimes the baby cannot breastfeed, so you have to express milk and bottle feed the baby. Some babies are formula fed because for some reason breastfeeding is not possible, or lactation has stopped prematurely, or you have chosen to formula feed your baby.
Some babies are formula fed because for some reason breastfeeding is not possible, or lactation has stopped prematurely, or you have chosen to formula feed your baby.
- Make sure that the rate of milk flow from the bottle through the nipple is appropriate for the baby.
- To check this, turn the filled bottle upside down.
- Milk should drip quickly, not squirt. If you have to shake the bottle hard to make the milk drip, it means that the nipple is not providing the normal intensity of feeding.
- The baby can fall asleep even before he has eaten everything from the bottle.
- It is normal for a small amount of milk to leak from the corners of the mouth; it will stop when the child gets older.
- If you can't find the perfect nipple, choose the one that produces the most milk; it's okay if you have to go through how many nipples before you find one that's right for you and your baby.
How to bottle feed your baby
- Sit back and hold your baby in your arms, gently but firmly.
 It is better for the baby to be in a more upright position, similar to the position when breastfeeding.
It is better for the baby to be in a more upright position, similar to the position when breastfeeding. - Place the pacifier between the baby's lips; he will open his mouth and start sucking.
- Hold the bottle at an angle so that the nipple and neck of the bottle are constantly filled with milk; this will prevent the child from swallowing air.
- When the baby stops actively sucking or has eaten half the milk from the bottle, carefully remove the bottle and check if he wants to burp; after that, you can continue feeding.
- Change the position of the baby during feeding or at least at each feeding; this allows even stimulation of the baby's sensations on both sides of the body and prevents positional deformation of the head.
How much milk does a baby need?
- The number of meals and the amount of milk is determined by the baby! Different babies require different amounts of breast milk or formula. Feeding time is not always evenly distributed over the time of day, sometimes children eat more during the day, followed by a long night break.
- If you are formula feeding, check the chart on the box. Of course, the recommended serving size for your age will only serve as a guideline and may not necessarily be appropriate for your child.
- When a baby begins to receive complementary foods, as the amount of solid food increases, the baby's need for milk decreases.
- The amount of formula your baby eats will decrease when he switches from bottle to cup.
- By the age of 12 months, when a baby can switch to cow's milk, he usually receives 500-600 ml of breast milk or formula per day.
Some babies never eat the recommended amount of milk for their age and height. For some, this "recommended" volume is not enough. At least six wet diapers during the day, constant but not excessive weight gain, a healthy and active child - all this indicates that everything is in order. If you are concerned that your baby is not getting enough milk or formula, contact your doctor.
Responsive feeding from the bottle in accordance with the needs of the child
- Feed the baby when he shows that he is hungry and not on the schedule, follow his signals.

- Do not feed the baby if he is not hungry, just because the formula is already prepared - this can lead to overfeeding the baby.
- When a baby is bottle fed, there is no difference between foremilk and hindmilk that affects the feeling of fullness in a breastfed baby.
- The child is often held so that the milk simply flows into the mouth rather than actively suckling; in this case, he eats too much milk too quickly.
- During feeding, watch the baby for signs of satiety - he turns away from the bottle, sucks lazily - and stop feeding in time.
- Hold the baby close to you during feeding, hug and talk to him; it stimulates growth and development and also strengthens the bond between you and your child.
- The baby did not eat everything from the bottle and fell asleep while eating.
- Don't worry if the child hasn't eaten everything; he knows how much formula or breast milk he needs.
- If the child falls asleep while eating, put him on your shoulder, stroke or pat him on the back and legs; Changing diapers is also an effective way to wake up a baby.
- Wait until the baby is awake before giving him any leftover milk.
Always empty the remaining milk from the bottle if more than an hour has passed!
Night feeding
- Every baby is different. Some wean from night feeding at four months, and some at two years. From the 6th month of life, healthy children no longer need night feeding. Now it's just a habit that gets harder to change the older the child gets.
- If a baby is bottle fed, this is the last age to stop eating at night! Do not replace milk with juices or other sweetened drinks to protect your child's teeth from cavities.
- If your baby drinks 60 ml or less of milk during the night, you can simply stop feeding at night and calm the baby as you usually do, and then put him back in the crib to fall asleep on his own.
- If your baby eats more than 60 ml every night, gradually reduce the amount of milk over 5-7 nights and lull the baby as you normally do.

Risks of bottle feeding in bed
- If your child gets used to falling asleep with a bottle in bed, it will be more difficult for him to learn to calm down or fall asleep on his own.
- If a child falls asleep with a bottle in his mouth, there is a risk of choking on milk and suffocation. Babies are not as light sleepers as older children and adults, and do not wake up if something prevents them from breathing.
- A mixture left in the mouth during sleep leads to dental caries.
- When a child drinks from a bottle lying down, the risk of ear inflammation increases.
Australian Article
On
Cover Image
Image
© UNICEF/UN0158032/Voronin
KeyWords
Breast Feed
Category
Power
Child Age
1st month
2nd month
3-4 months
003
Share this information
If your baby is unable to breastfeed for health reasons (for example, due to a physical defect, neurological disorder, cleft lip or palate), the SpecialNeeds cup will help you solve this problem. With such disorders, the baby, as a rule, is not able to create a vacuum to suck milk from the breast. The SpecialNeeds sippy cup responds to gentle pressure, allowing your little one to drink effortlessly.
With such disorders, the baby, as a rule, is not able to create a vacuum to suck milk from the breast. The SpecialNeeds sippy cup responds to gentle pressure, allowing your little one to drink effortlessly.
How the SpecialNeeds cup works
Instead of the standard teat, the SpecialNeeds cup has a narrower, longer teat made of ultra-soft silicone. The slit-like valve at the tip of the nipple opens with the slightest squeeze and closes as soon as the baby stops sucking, so that he does not choke on the expressed milk.
The marking on the nipple helps you choose the best feeding position for your baby. When the baby squeezes the nipple in his mouth, the milk flows at different speeds depending on the position of the nipple. In addition, you can lightly squeeze the nipple with your fingers so that the baby can get more milk. The one-way valve between bottle and nipple allows for safe control of milk flow and prevents air from entering.
For little ones, the Mini SpecialNeeds pacifier can be used. Both the standard and mini teats are reusable when cleaned and sterilized according to instructions.
Both the standard and mini teats are reusable when cleaned and sterilized according to instructions.
When should I use the SpecialNeeds Cup?
In some cases, the use of a special bottle, such as the SpecialNeeds cup, eliminates the need for tube feeding. If your baby can latch on but doesn't have the strength or energy to suck out enough milk, a cup can be a great way to supplement your baby with expressed milk to meet his nutritional needs.
This is an important argument in favor of drinking cups, as many babies with special needs are discharged from the hospital as soon as they are able to get enough milk for normal growth. So the SpecialNeeds cup can be the deciding factor in whether your baby goes home or stays in the hospital.
If your baby needs surgery, you can use the SpecialNeeds sippy during the recovery period, while your baby is having trouble suckling or is not strong enough to do so.
Using the SpecialNeeds Cup
If you or your baby need help with breastfeeding, contact your healthcare provider or a lactation consultant or specialist.